A Novel Approach for Restoration of Hemisectioned Mandibular Second Molar with Modified Tunnel Restoration: A Case Report
Madhu Varma K1, Jyothi Chittem2, Kalyan Satish R3, Sita Rama Kumar M4, Girija S Sajjan5
1 Professor, Department of Conservative Dentistry and Endodontics, Vishnu Dental College, Bhimavaram, Andhra Pradesh, India.
2 Post Graduate, Department of Conservative Dentistry and Endodontics, Vishnu Dental CollegeBhimavaram, Andhra Pradesh, India.
3 Professor, Department of Conservative Dentistry and Endodontics, Vishnu Dental College, Bhimavaram, Andhra Pradesh, India.
4 Senior Lecturer, Department of Conservative Dentistry and Endodontics, Vishnu Dental College, Bhimavaram, Andhra Pradesh, India.
5 Professor & HOD, Department of Conservative Dentistry and Endodontics, Vishnu Dental College, Bhimavaram, Andhra Pradesh, India.
NAME, ADDRESS, E-MAIL ID OF THE CORRESPONDING AUTHOR: Dr. Jyothi Chittem, Post Graduate, Department of Conservative Dentistry and Endodontics, Vishnu Dental College, Bhimavaram-534202, Andhra Pradesh, India. Phone : 09492948165, E-mail : jyothichittem87@gmail.com
Hemisection refers to sectioning of a mandibular molar into two halves followed by removal of the diseased root and its coronal portion. Hemisection of a mandibular molar may be a suitable treatment option when the decay is restricted to one root and the other root is healthy. The retained root is endodontically treated and the furcation area is made self-cleansable. Retained tooth structure is restored as premolar which helps to reduce the masticatory load. Hemisection of mandibular molar was often referred to as premolarization. Studies showed that the remaining coronal structure influenced the fracture resistance of endodontically treated maxillary first premolars. Clinical experience showed the viability of tunnel restoration as an alternative to class II conventional cavity preparation in initial proximal lesion. This article discusses a case that presents the novel technique involved in restoration of the remaining hemisected tooth using modified tunnel restoration.
Hemisection, Mandibular molars, Root canal treatment, Tunnel restoration
Case Report
A 37-year-old male patient reported to the Post Graduate Department of Conservative Dentistry and Endodontics, Vishnu Dental College, Bhimavaram with a chief complaint of food impaction and intermittent pain in the lower left back teeth region since one month. Patient’s medical history was noncontributory and the extraoral findings were within normal limits. Patient underwent fixed partial denture in relation to 23, 24, 25 and restorations in 34 and 35 one year back.
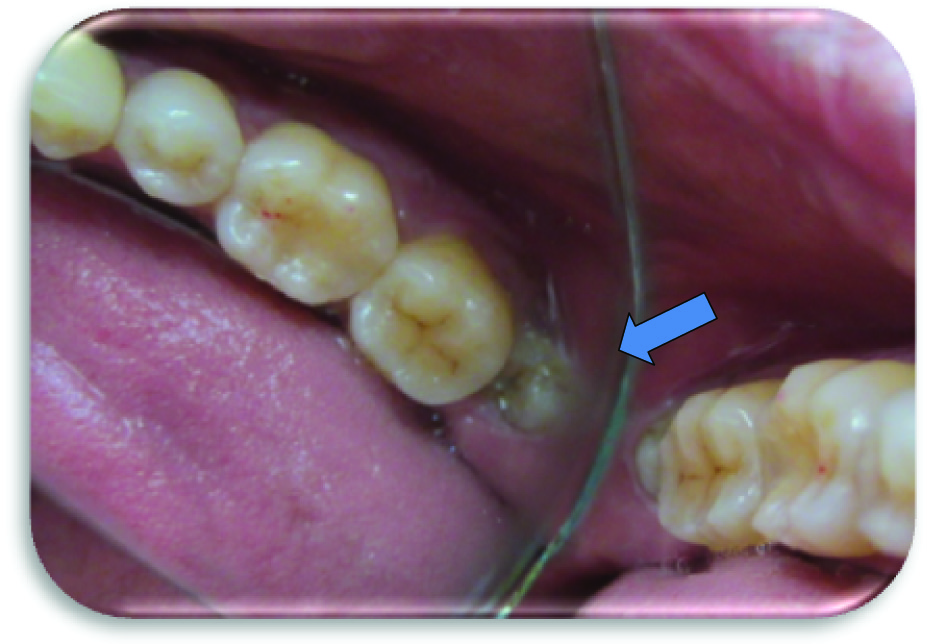
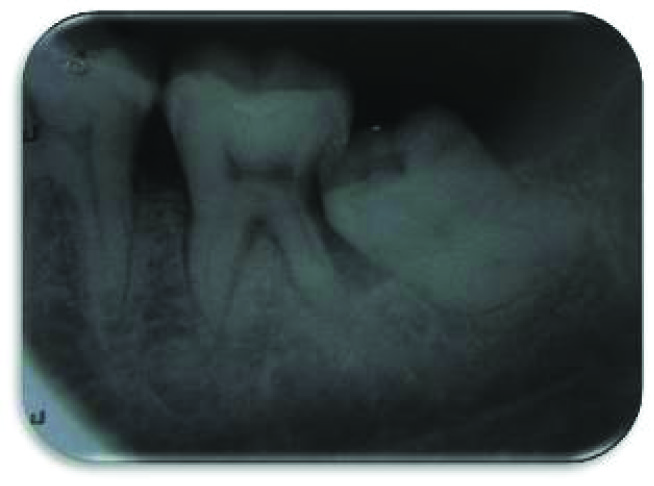
On intra oral examination, it was found that the patient had impacted 38 [Table/Fig-1]. Percussion tests were negative for both 36 and 37. However 37 showed grade I mobility. Vitality tests revealed the irreversible pulpal status in relation to 37. Radiographic examination showed the mesio-angular impaction in relation to 38 and radiolucency in the disto-proximal tooth structure involving dentin and pulp in relation to 37 [Table/Fig-2]. A diagnosis of irreversible pulpitis associating with pressure induced root resorption of distal root was proposed in relation to 37. Various treatment options were considered like extraction of 37 and 38 followed by replacement of 37 with either a dental implant or removable partial denture or cantilever bridge. Finally hemisection of distal root along with surgical extraction of impacted third molar was planned.
Preoperative clinical photograph
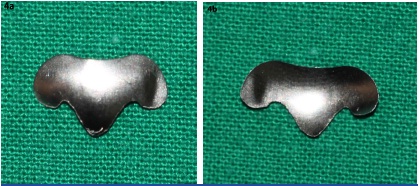
The procedure was performed as follows: After the administration of the local anesthetic, 2% Lignocaine with 1:100,000 epinephrine (Xicaine, ICPA Health Products Ltd, Gujarat, India), conservative oval shaped access cavity (similar to access cavity preparation in mandibular second premolar) was prepared on the mesial one third of occlusal surface of tooth. Pulp extirpation was done. Working length was established for mesial canals with radiographic method and reconfirmed with apex locator (Root ZX, J.Morita USA, Inc.). A coronal slit was prepared at the junction of middle and distal third of occlusal table [Table/Fig-3]. It extends from occlusal table to the cemento enamel junction. The canals were cleaned and shaped with NiTi rotary files (Protaper Universal, Dentsply Maillefer, Ballaigues, Switzerland). Irrigation was done with 5.25 % sodium hypochlorite (V-consept, Vishal Dentocare, India). Master cone was selected and obturation done using guttapercha with resin-based root canal sealer (AH Plus, Dentsply De Trey GmbH, Germany). Modified T-shaped matrix band [Table/Fig-4a,4b] (The Palodent System, Dentsply, Caulk) was placed in the coronal slit area which provides support for the complete flow of flowable composite (Filtek Z 350 XT Flowable Restorative, 3M ESPE) into the irregularities [Table/Fig-5] followed by sealing of access cavity with composite material (Filtek Z 350 XT Universal Restorative System, 3M ESPE). Vertical and sulcular incisions were given to the patient more distally and a full thickness mucoperiosteal flap was elevated to expose the impacted tooth. Through the coronal slit cut was extended to furcation level with the help of slow speed handpiece under abundant coolant hemisection of 37 was completed. Extraction of impacted 38 was done. A finishing diamond bur was used to smoothen the distal area of the mesial root and coronal portion of 37. The flap was repositioned and interrupted sutures were placed using 3/0 black silk sutures (Mersilk - Ethicon, Division of Johnson & Johnson Ltd., Aurangabad, India). Occlusion was verified and adjusted to remove the occlusal interferences.
Coronal slit preparation with access cavity

Modified T- shaped matrix band (Outer and Inner surface)
Modified tunnel restoration with restorative composite material

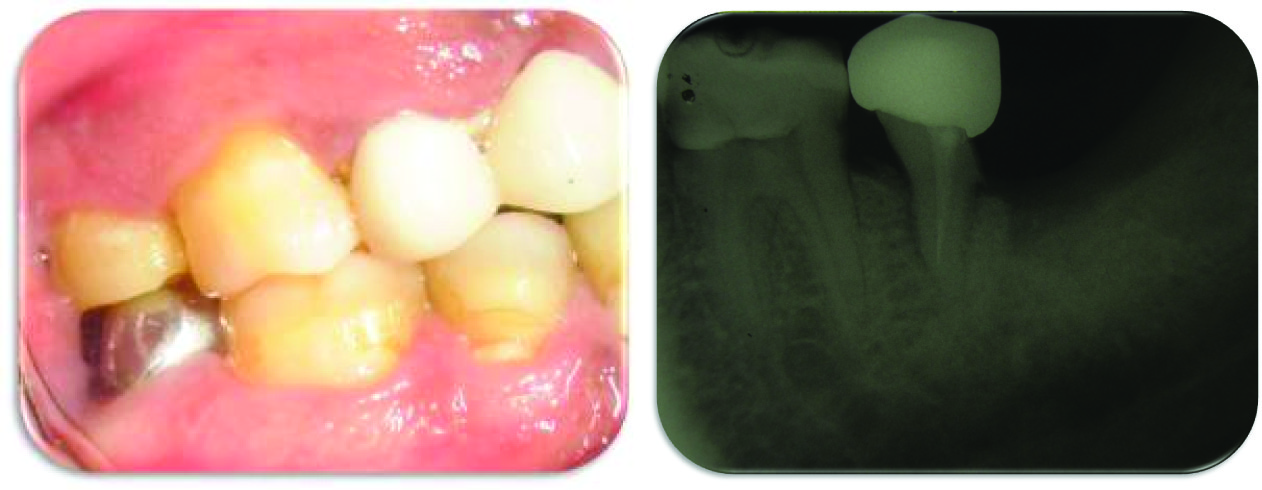
At a follow-up appointment one week later, satisfactory healing was noticed and sutures were removed. When the patient returned after one month, patient was completely asymptomatic. Clinically, satisfactory healing was noticed at the extracted socket. Tooth preparation was done for full metal crown in 37 [Table/Fig-6]. Rubber based impressions (Aquasil, Dentsply, Caulk) were made. A temporary crown was fabricated from BIS-GMA (bisphenylglycidyl dimethacrylate (Integrity, Dentsply, Philadelphia, Penn.) cemented with non-eugenol cement (Temp-Bond NE, Orange, Calif). One week later metal crown was cemented onto hemisected tooth after verification of occlusion with dual cure resin-based cement (Rely X TM, 3M ESPE). Recall was done periodically to assure the healing and success of the restoration. After one year follow-up, occlusion was stable and the patient was satisfied with the outcome [Table/Fig-7,8].
Preservation of distal marginal dentin

One year follow up clinical photograph and radiograph
Discussion
The main aim of hemisection surgery is to preserve as much viable part of tooth as possible to be used as a prosthetic abutment [1]. The factors that favour a favourable prognosis in hemisection surgery include; adequate bone support, high furcation levels and achieving a supra gingival restoration margin [2]. If all these criteria are met, hemisection surgery is an alternative to extraction of a tooth and its replacement with either a dental implant or conventional fixed partial denture [3]. A predictable and good quality of endodontic treatment is of paramount importance and also adequate residual crown structure to provide good resistance and retention for definitive restoration [4]. Preservation of tooth structure is important for its protection against fracture under occlusal loads and may influence the tooth prognosis [2]. The structural strength of a tooth depends mainly on the amount of sound dentin available to support and retain restorations. Many studies [4–6] have shown that fracture resistance of prepared tooth is directly proportional to the amount of remaining tooth structure. In vitro studies [7, 8] showed that the adhesive restorations in premolars restored the strength of undermined marginal ridges in tunnel preparations. Clinical studies [9] confirmed the viability of tunnel restoration procedure as an alternative to conventional Class II cavity restorations for initial proximal lesions. This case report discusses a novel approach for restoration of hemisectioned mandibular second molar with modified tunnel restoration. Hemisection may be a suitable alternative to extraction and implant therapy and should be discussed with patients during consideration of treatment options [3, 10–12]. Hemisection allows for physiologic tooth mobility of the remaining root. Following careful clinical and radiographic examination, hemisection can be selected as an appropriate treatment alternative in cases where one of the roots has a decay which is beyond the scope of restoration [10].
Based on clinical and radiographical examination a diagnosis of pressure induced root resorption was made in relation to 37. Restoring the extensively damaged dentition has always been a difficult decision-making process for the dental practitioner. Decisions to restore these teeth were primarily based on the fact that “fixed” teeth are typically better functionally than “removable” teeth and better esthetically than “no” teeth. Implant therapy is a predictable option with good functionality [3]; however, in this case, distally bone loss extends upto apical third and the resorption was extended subgingivally onto the middle third of the distal root which results in poor restorative prognosis. However, in this case, the patient chose an alternative treatment because of his financial consideration.
Studies [8,13] on tunnel preparation in premolars with adequate amount of remaining marginal ridge and use of adhesive restorative materials showed no significant decrease in strength compared to sound teeth. Fracture of endodontically treated maxillary first premolars is a common problem in the clinical setting [4–6]. The post-core technique has been used to restore these teeth. However, long-term follow-up studies have shown that posts dislodge and root fractures still occur. Some [8,13] believe that there is no appreciable improvement in tooth resistance to occlusal forces and that, when possible, the use of posts should be avoided to provide core retention. Furthermore, insertion of the post results in substantial tooth weakening [4].
The access cavity preparation for mandibular second molar is generally triangular or rhomboidal in shape. But, in this case conservative oval shaped access cavity was prepared to conserve the maximum tooth structure. This procedure conserves the dentin between oval access cavity and distal slit. The conserved tooth structure by its arch form over the pulp chamber along with restorative composite material provides better resistance form to the remaining tooth. A coronal slit was prepared at the junction of middle and distal third of occlusal table and extended upto the cemento enamel junction. During root canal treatment itself coronal slit provides access for the extirpation of pulp from distal canal to control bleeding from distal root. It also provides path for the escape of irrigants and preserves the distal marginal dentin [7,9]. During post endodontic treatment it helps in placement of modified matrix band and retainer to completely seal the distal irregularities of resected tooth [14]. The modified matrix band acts as an artificial barrier that restricts the flow of restorative material distally and aids in proper compaction of restorative composite material [Table/Fig-5]. During tooth preparation for crown, it facilitates the establishment of proper finish line. It also provides guidance for sectioning the distal portion of molar root. Removal of the distal portion of tooth facilitated the extraction of impacted third molar.
Conclusion
This technique provides a new dimension towards conservative restoration of tooth following hemisection. Distal marginal dentin of remaining abutment tooth was preserved. The preserved distal marginal dentin could act as a hypothetical distal marginal ridge of remaining tooth. In a tunnel restoration, restorative material fills the prepared cavity and extends into the proximal caries lesion. Similarly in the above technique, the restorative composite material fills the pulp chamber extending distally into the coronal slit reinforcing the remaining tooth structure. The clinician is provided with a template for tooth preservation, less chair side time and adequate guide for hemisection and finish line preparation. This novel technique aids in maintaining the smaller size of the occlusal table, under-contouring of the embrasure spaces and ensuring that the crown margin encompasses the furcation which could result in higher success rate in hemisection therapy.
[1]. Saad MN, Moreno J, Crawford C, Hemisection as an alternative treatment for decayed multirooted terminal abutment: A case reportJCDA 2009 75:387-90. [Google Scholar]
[2]. Guldener PH, Hemisection, tooth separation and root amputationSSO Schweiz Monatsschr Zahnheilkd 1976 86:795-811. [Google Scholar]
[3]. Gregory-George Z, Hoffmann O, Kasaj A, Mandibular molar root resection versus implant therapy: a retrospective nonrandomized studyJ Oral Implantol 2009 35:52-62. [Google Scholar]
[4]. Nissan J, Barnea E, Bar-Hen D, Assif D, Effect of remaining coronal structure on the resistance to fracture of crowned endodontically treated maxillary first premolarsQuintessence Int 2008 39:e183-87. [Google Scholar]
[5]. Arunpraditkul S, Saengsanon S, Pakviwat W, Fracture resistance of endodontically treated teeth: three walls versus four walls of remaining coronal tooth structureJ Prosthodont 2009 18:49-53. [Google Scholar]
[6]. Bassir MM, Labibzadeh A, Mollaverdi F, The effect of amount of lost tooth structure and restorative technique on fracture resistance of endodontically treated premolarsJ Conserv Dent 2013 16:413-17. [Google Scholar]
[7]. McComb D, Systematic review of conservative operative caries management strategiesJ Dent Educ 2001 65:1154-61. [Google Scholar]
[8]. Ji W, Chen Z, Frencken JE, Strength of tunnel restored teeth with different materials and marginal ridge heightDent Mater 2009 25:1363-70. [Google Scholar]
[9]. Geoffrey MN, The tunnel restoration - nine years of clinical experience using capsulated glass ionomer cements. case reportAust Dent J 1992 37:245-51. [Google Scholar]
[10]. Buhler H, Survival rates of hemisected teeth: an attempt to compare them with survival rates of alloplastic implantsInt J Periodontics Restorative Dent 1994 14:536-43. [Google Scholar]
[11]. Park JB, Hemisection of teeth with questionable prognosis. Report of a case with seven-year resultsJ Int Acad Periodontol 2009 11:214-19. [Google Scholar]
[12]. Kurtzman GM, Silverstein LH, Shatz PC, Hemisection as an alternative treatment for vertically fractured mandibular molarsCompend Contin Educ Dent 2006 27:126-29. [Google Scholar]
[13]. Fasbinder DJ, Davis RD, Burgess JO, Marginal ridge strength in class II tunnel restorationsAm J Dent 1991 4:77-82. [Google Scholar]
[14]. Johannes E, Frankenberger Anselm P, A novel approach for filling tunnel-prepared teeth with composites of two different consistencies: A case presentationQuintessence Int 2012 43:93-96. [Google Scholar]