Dental plaque, a bacterial biofilm, is one of the major aetiologic agents involved in the initiation and progression of dental caries, gingivitis and periodontal disease [1]. Therefore, effective oral hygiene involving removal and control of dental biofilm formation plays a crucial role in prevention and successful treatment of dental disease.
The main measures for controlling bacterial plaque are of a mechanical nature (toothbrushing and dental floss). However, both the absence of hygiene habits and the inability to perform correct toothbrushing can make mechanical plaque control insufficient [2]. In general, individuals remove only around half of the plaque from their teeth even when brushing for 2 min [3]. Whereas the control of interproximal biofilm formation requires use of an interdental oral hygiene aid, one such aid being dental floss [4]. According to American Dental Association, 80% of the plaque can be removed by this method [5].
While mechanical methods of plaque removal are considered the standard for individually applied oral disease preventive practices, the high prevalence of gingival disease has prompted research into and development of adjunctive methods for controlling biofilms [6]. In 2002, data presented at the International Association for Dental Research (IADR) meeting supported the benefit of oral rinsing with chemotherapeutics as an adjunct for controlling plaque and maintain gingival health [7].
Although many products have been used to control plaque and gingivitis, Chlorhexidine (CHX) is one of the most widely used and thoroughly investigated antiseptics. Years of documented research have established that CHX digluconate is safe, stable and effective in preventing and controlling plaque formation, breaking up existing plaque, and inhibiting and reducing the development of gingivitis [8].
However, the efficacy of dental floss and chlorhexidine mouthrinse is well established in reducing interproximal gingivitis, only few studies have been conducted to compare the both. Earlier studies [9] had proven that some adjuncts should be used along with toothbrushing in the control of bacterial biofilm. Hence, this study was conducted to compare the clinical efficacy of dental floss and chlorhexidine mouthrinse as an adjunct to toothbrushing in removing plaque and gingival inflammation.
Materials and Methods
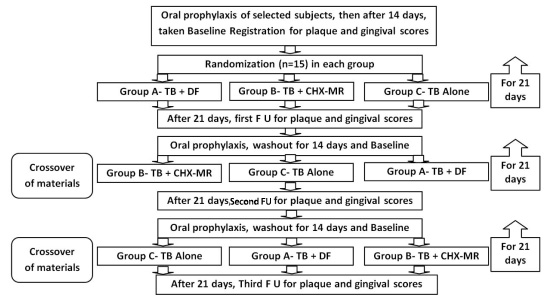
A randomized, double-blind, three-way crossover clinical trial [Table/Fig-1] was conducted among 45 dental students from Kothiwal dental college and research centre, Moradabad for three and a half month from April to July 2013. The protocol of the study was approved by the Institutional Ethical Committee. Informed consent, both oral and written, was sought from all participating subjects after giving a brief description of the purpose, aim, duration, possible benefits and side effects of the study. Inclusion criteria include dentate subjects with atleast 24 natural teeth, systemically healthy, a mild gingival scores between 0.70-0.90 (Loe and Sillness, 1963) and a low plaque scores less than 1 (Turesky modification of the Quigley-Hein Index. Exclusion criteria Included patient undergoing orthodontic treatment, presence of multiple open interproximal surfaces, history of allergic reactions to CHX, proximal carious lesion, use of antibiotics, dental floss and CHX-MR in the preceding 3 months and pregnancy or medication that might interfere with the conduct of the study.
Depicts flowchart for the design of the study; FU – Follow up
Design and Clinical Procedures
Two weeks before the commencement of the study, participants received an intraoral examination and a full mouth oral prophylaxis. The participants were then instructed to continue their usual oral hygiene routine for the following two weeks. Two weeks later, participants underwent baseline registration of gingival inflammation and plaque accumulation. All the subjects were then randomly assigned into three different groups (n=15) with different cleaning regimens i.e. Group A – Toothbrushing with Dental Floss (TB+DF), Group B – Toothbrushing with 0.12% Chlorhexidine Gluconate Mouthrinse (TB+CHX-MR) and Group C – Toothbrushing Alone (TB Alone) by a person not concerning with the study. All subjects had to undergo three different tooth cleaning regimens in a three-way crossover manner for a treatment period of 21d followed by a washout period of 14d. Subjects were then told to brush with a toothpaste and toothbrush which they were using before the start of the study during washout period [Table/Fig-1]. Clinical scores for each parameter were obtained by a single examiner (kappa value 90%) and an ADA Type III Clinical examination [10] was done. Participants received brief instructions for the procedure they had to perform i.e., Flossing and rinsing in addition to their routine toothbrushing. Subjects in the rinsing group were instructed to use 15 ml mouth rinse for 30 sec twice daily, 30 min after tooth brushing. Subjects in the flossing group were given a demonstration of flossing and instructed to floss once daily before going to bed. To achieve standardized conditions, each subject used the same type of new toothbrush and toothpaste and advised to brush twice daily.
Subjects were given an adequate supply of DF and 0.12% CHX-MR and were directed to clean their teeth with an assigned regimen for a period of 21d. During the study period, the use of oral hygiene tools other than the attributed was strictly prohibited. Before each study visit, subjects refrained from oral hygiene for 24 hr.
Clinical parameters evaluated in the study were buccal/ lingual plaque using the Turesky modification of the Quigley-Hein Index Turesky et al., [11], Gingival Inflammation using the Gingival Index GI, Loe et al., [12]. All plaque scores were recorded after gingival assessments, and after tooth surfaces were stained with disclosing solution.
After a 21d trial period, each subject returned for scoring of clinical parameters, oral prophylaxis, baseline registration and instruction for another (of the three) tooth cleaning regimens. The study continued in this manner for a period of three and a half months, allowing each group to follow each of the three regimens for 21d followed by a washout period of 14d to avoid carryover effect. The clinical examiner had no knowledge to which study group patients were assigned to at any time during the study period.
Statistical Analysis
Statistical analysis was done by using the mean and standard deviation (SD). First analysis of variance (ANOVA) test was performed to determine the differences among products tested. In the presence of significant differences, pair wise comparisons were made via post hoc test. p-value <0.001 was considered statistically significant. Change from baseline values were evaluated using t-test.
Result
Statistically significant difference were observed (p<0.001) when the change from baseline was observed at different follow ups in all the regimes allotted. More reduction from baseline was observed at Group B (TB+CHX-MR) followed by Group A (TB+DF) group then toothbrush alone group [Table/Fig-2]. On comparing intergroup difference for different regimes at different follow ups, statistically significant difference were observed (p<0.001) except baseline. While comparing between Group A (TB+DF) and Group B (TB+CHX-MR) at different follow ups, significant difference were observed for gingival and plaque index which is same when the comparison were performed between group B (TB+CHX-MR) and group C (TB Alone). At second and third follow up for group A (TB+DF) and group C (TB Alone) showed no significant difference for both the index though group A showed reduction in mean values but values are not significant [Table/Fig-3]. At different follow ups, the mean values for mandibulars are more than the maxillary teeth for the plaque index and gingival index when compared within the groups for different cleaning regimens [Table/Fig-4]. Also, mandibular lingual surface had more plaque and gingivitis than the maxillary palatal surfaces.
Depicts change from baseline at different follow ups for different allotted regimes using paired t-test., p<0.001 is statistically significant
| Clinical Parameters | Baseline | First Follow Up | P Value | Baseline | Second Follow Up | p-value | Baseline | Third Follow Up | P Value |
|---|
| Group A - Tooth Brush + Dental Floss |
| GI | 0.65±0.03 | 0.27±0.01 | <0.001 | 0.63±0.07 | 0.29±0.03 | <0.001 | 0.66±0.03 | 0.29±0.02 | <0.001 |
| P I | 0.68±0.05 | 0.32±0.03 | <0.001 | 0.68±0.04 | 0.34±0.03 | <0.001 | 0.70±0.07 | 0.40±0.06 | <0.001 |
| Group B - Tooth Brush + Chlorhexidine Mouthrinse |
| GI | 0.63±0.04 | 0.18±0.02 | <0.001 | 0.64±0.03 | 0.17±0.03 | <0.001 | 0.61±0.04 | 0.18±0.01 | <0.001 |
| PI | 0.67±0.07 | 0.23±0.02 | <0.001 | 0.67±0.04 | 0.25±0.01 | <0.001 | 0.69±0.03 | 0.21±0.03 | <0.001 |
| Group C - Tooth Brush Alone |
| GI | 0.64±0.03 | 0.35±0.04 | <0.001 | 0.64±0.07 | 0.35±0.05 | <0.001 | 0.63±0.04 | 0.32±0.04 | <0.001 |
| PI | 0.66±0.07 | 0.43±0.09 | <0.001 | 0.66±0.03 | 0.40±0.01 | <0.001 | 0.69±0.07 | 0.46±0.12 | <0.001 |
Depicts intergroup mean comparison between different regimens for plaque and gingival index using ANOVA followed by post hoc.
| Group A TB+ DF | Group B TB+ CHX-MR | Group C TB Alone | p-value | GP.A VS GP.B | GP.A VS GP.C | GP.B VS GP.C |
|---|
| Diff. | P | Diff. | P | Diff. | P |
|---|
| Gingival Index |
| Baseline | 0.65±0.03 | 0.63±0.04 | 0.64±0.03 | 0.406* | |
| First FU | 0.27±0.01 | 0.18±0.02 | 0.35±0.04 | <0.001 | 0.09 | <0.001 | 0.09 | <0.001 | 0.18 | <0.001 |
| Second FU | 0.29±0.03 | 0.17±0.03 | 0.35±0.05 | <0.001 | 0.13 | <0.001 | 0.06 | 0.118* | 0.18 | <0.001 |
| Third FU | 0.29±0.02 | 0.18±0.01 | 0.32±0.04 | <0.001 | 0.11 | <0.001 | 0.03 | 0.006* | 0.14 | <0.001 |
| Plaque Index |
| Baseline | 0.68±0.05 | 0.67±0.07 | 0.66±0.07 | 0.586* | |
| First FU | 0.32±0.03 | 0.23±0.02 | 0.43±0.09 | <0.001 | 0.09 | <0.001 | 0.11 | <0.001 | 0.19 | <0.001 |
| Second FU | 0.35±0.03 | 0.25±0.10 | 0.41±0.10 | <0.001 | 0.10 | <0.001 | 0.07 | 0.009* | 0.16 | <0.001 |
| Third FU | 0.40±0.16 | 0.21±0.03 | 0.40±0.06 | <0.001 | 0.19 | <0.001 | 0.06 | 0.118* | 0.25 | <0.001 |
* not significant, p<0.001 is statistically significan
Depicts intergroup mean difference for plaque index and gingival index at different follow up for maxillary and mandibular arch
| Maxila | Mandible |
|---|
| TB + DF | TB + CHX-MR | TB ALONE | TB + DF | TB + CHX-MR | TB ALONE |
|---|
| Plaque Index | Baseline | 0.67±0.05 | 0.66±0.06 | 0.65±0.07 | 0.74±0.05 | 0.73±0.07 | 0.73±0.07 |
| First Follow-Up | 0.29±0.03 | 0.22±0.01 | 0.43±0.08 | 0.36±0.03 | 0.24±0.02 | 0.47±0.07 |
| Second follow-up | 0.30±0.03 | 0.23±0.03 | 0.40±0.12 | 0.38±0.04 | 0.33±0.13 | 0.38±0.04 |
| Third Follow-Up | 0.32±0.03 | 0.22±0.01 | 0.41±0.12 | 0.39±0.03 | 0.25±0.01 | 0.25±0.01 |
| Gingival Index | Baseline | 0.64±0.07 | 0.61±0.06 | 0.62±0.06 | 0.67±0.04 | 0.65±0.06 | 0.66±0.06 |
| First Follow-Up | 0.25±0.02 | 0.16±0.04 | 0.34±0.03 | 0.30±0.02 | 0.18±0.03 | 0.41±0.04 |
| Second Follow-Up | 0.26±0.02 | 0.15±0.04 | 0.34±0.04 | 0.31±0.03 | 0.16±0.06 | 0.41±0.04 |
| Third Follow-Up | 0.27±0.04 | 0.15±0.04 | 0.32±0.03 | 0.32±0.05 | 0.19±0.04 | 0.38±0.03 |
Discussion
Since plaque is the main etiological factor for the dental disease to develop. Hence, daily removal of interproximal plaque is an important factor for the maintenance of gingival, periodontal and dental health; as with the development of dental plaque, there is colonization of pathogenic micro-organisms that releases various endotoxins, which causes inflammation of gingiva. By various researches conducted earlier it has been proved that CHX-MR when used as an adjunct to toothbrushing proved to be a “gold standard” for the reduction of plaque from tooth surface preventing plaque induced gingivitis.
A three-way crossover design was implicated in the study, although we have a limited data regarding these trials, though it offers certain advantages. All the participants were assured that sometime during the course of investigation, they will receive a new therapy. These studies economize on the total number of patients required at the expense of the time necessary to complete the study.
The present study showed that rinsing with 0.12% CHX-MR twice daily along with toothbrushing significantly reduced the clinical evidence of gingival inflammation compared to Group A (TB+DF) and a control group (TB Alone).
Among the three follow ups, there is a significant change from baseline and the mean values were statistically significant for plaque and gingival scores. Addition of flossing into an oral hygiene regimen did not show any improvement versus the use of toothbrush alone for plaque and gingival scores which was consistent with the study done by Schiff et al., [13], Zimmer et al., [14], and Halla-Junior and oppermann [15]. But it was in contrast with the study done by Hague and carr [16], Jared et al., [17], Sharma et al., [18] and Bauroth et al., [19] which showed significant reduction for plaque scores but not for gingival inflammation. This may be due to the fact that the percentage of people using floss varies geographically. So, its efficacy was more in the present study where only dental personnel were using it.
The present study depicts that 0.12% CHX-MR in addition to toothbrushing demonstrated an ability to significantly reduce plaque accumulation and gingival inflammation than dental floss group and toothbrush alone group. Optimally, mouthrinsing should be performed twice daily. The substantivity of current mouthrinses is of less than 12 hours duration [20] and after four days of not rinsing, it has been shown that bacterial composition of plaque returns to its baseline level before rinsing was initiated [21] Segreto et al., [22], who showed that 15 ml of either 0.12% or 0.2% chlorhexidine mouthwash was significantly clinically better than placebo mouthwash when used alongside toothbrushing. The high efficacy could be explained by its immediate bactericidal action during the time of application followed by a prolonged bacteriostatic action due to adsorption on the tooth surface [23]. The 0.12% concentration was selected based on the previous study [22] which indicated a lower concentration of CHX was just as effective in reducing gingivitis as 0.20% concentration.
Rinsing is easier than either brushing or flossing and takes less time, therefore requiring a shorter attention span. Patients also tend to be more concerned with “fresh breath” than with plaque and gingivitis levels, and patient compliance with rinsing may be superior to patient compliance with adequate brushing and flossing (or other interdental cleaning).
In all the measured clinical parameters, buccal surfaces were more cleaned as compared to the lingual and palatal surface. A possible explanation could be that with tooth brushing, the facial surfaces were more accessible and easily cleansed whereas lingual and palatal surfaces were easily skipped.
Mouthrinse being in close proximity to the lingual/ palatal surfaces exerted a more profound antibacterial action on the plaque on this side and the natural cleansing action of the tongue and saliva occurred more on the lingual/ palatal surface.
In this study, the mean values of plaque pattern revealed that plaque formed was more on the mandibular arch than on the maxillary arch. This may be attributed to the ease of accessibility of the facial surface of the maxillary arch with a toothbrush. The accessibility of the lingual surface of the mandibular arch could have been limited on account of limited access or obstruction by the tongue. Moreover, the stagnation of saliva on the floor of the mouth and the lower vestibule due to gravity lead to more plaque formation on the lower arch.
The present study also depicts mandibular lingual surfaces had more plaque than the comparable maxillary palatal surface. Many of these differences appear to be a consequence of tooth contour and position which is subject to friction by food and the tongue.
Introducing a bacterial rinse into the regimen (including where chemotherapeutic pastes are used) may provide additional benefits for patients, especially interdentally in harder to reach areas. The patient who brush well and floss daily may still benefit from adjunctive rinsing to help prevent the development and initial maturation phase of fresh plaque, thereby reducing the presence of acid-producing cariogenic bacteria associated with early plaque formation. In choosing a chemotherapeutic mouthrinse, considerations include the health status of the patient, whether the rinse is intended for short term or long term use, efficacy, propensity for staining, lack of microbial resistance, taste, and clinician and patient preferences.
The study subjects were only instructed to follow the regimen but monitoring it was beyond the control of the examiner. Consequently, there might be some irregularity in the way the subjects follow their respective regimen. Moreover, the study was done on the dental students who are more aware of oral health care. Therefore, generalising the result is difficult. So, a larger prospect of study can be planned using subjects from general population to get a more definite result.
Conclusion
The level of plaque accumulation and gingival inflammation efficacy provided by 0.12% CHX-MR was much better than that of the DF when used as an adjunct to toothbrushing. The inclusion of dental floss into normal toothbrushing did not reduce the clinical parameters during some stages in the study. Thus, by understanding the properties and limitations of the CHX molecule, the dental profession can ensure that the efficacy of the agent is maximized, allowing chlorhexidine to rightly remain as the gold standard when used in combination with normal toothbrushing.
* not significant, p<0.001 is statistically significan