Short and Hypertrophic Ligament of Treitz: A Rare Cause of Superior Mesentric Artery Syndrome
Suhani1, Lalit Aggarwal2, Shadan Ali3, Ashish Jhaketiya4, Shaji Thomas5
1 Senior Resident, Department of General Surgery, Lady Hardinge Medical College, New Delhi, India.
2 Assistant Professor, Department of General Surgery, Lady Hardinge Medical College, New Delhi, India.
3 Assistant Professor, Department of General Surgery, Lady Hardinge Medical College, New Delhi, India.
4 Former Senior Resident, Department of General Surgery, Lady Hardinge Medical College, New Delhi, India.
5 Director Professor and Surgical Unit Head, Department of General Surgery, Lady Hardinge Medical College, New Delhi, India.
NAME, ADDRESS, E-MAIL ID OF THE CORRESPONDING AUTHOR: Dr. Suhani, Senior Resident, Department of General Surgery, LHmc and SSkh, Shaheed Bhagat Singh Marg, New Delhi- 110001, India.
Phone: 9810534358,
E-mail: drsuhani@gmail.com
Superior mesenteric artery syndrome (SMAS) is a rare form of upper intestinal obstruction in which the third part of the duodenum is compressed between the superior mesenteric artery and the aorta, secondary to any condition decreasing the angle between these two arteries. We recently cared for a young male who came with features of proximal small bowel obstruction. On investigation, there was extrinsic duodenal obstruction. Exploratory laparotomy was done which revealed a short and hypertrophic ligament of treitz leading to compression of 3rd part of duodenum. Release of the ligament with doudenojejunostomy was done. Postoperatively, patient recovered well. This case report highlights the occurrence and importance of hypertrophic and contracted ligament of treitz as a rare cause of SMAS.
Duodenal Obstruction, Aorto Mesenteric Angle, Duodenojejunostomy, Intestinal Obstruction
Case Report
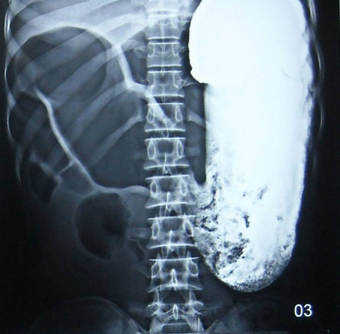
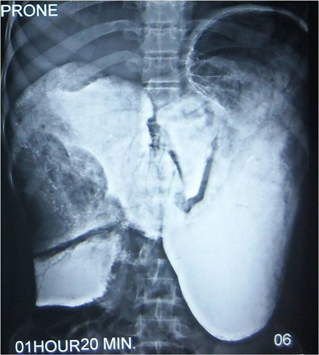
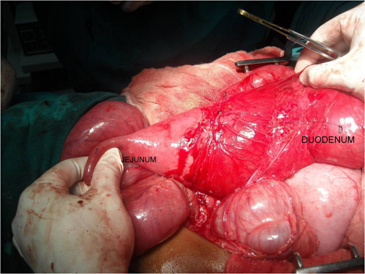
A 20-year-old thin built male was admitted with six months history of epigastric fullness, recurrent abdominal pain associated with vomiting which were improved with lying prone. He had a history of multiple admissions for suspected intestinal obstruction, wherein he was managed conservatively. On general examination, there was pallor, tachycardia and pedal oedema and BMI of 10.8 kg/m2. On abdominal examination, there were visible peristalsis in upper abdomen and hyper peristaltic bowel sounds. However, there was no sign of peritonitis. The patient was further investigated and put on parentral nutrition and expectant management meanwhile. Haematological investigations revealed anaemia, hypoalbuminemia and hypokalemia. Ultrasonographic evaluation of the abdomen depicted duodenum to be grossly dilated with collapsed small bowel loops. Upper GI endoscopy showed dilated stomach and duodenum with no obvious intraluminal pathology. On barium meal study, stomach and duodenum up to its 3rd part were grossly dilated with abrupt cutoff in 3rd part [Table/Fig-1a]. There was no passage of contrast on films taken after one and half hour [Table/Fig-1b]. A provisional diagnosis of superior mesenteric artery syndrome was made and patient was taken up for exploratory laparotomy. Intraoperative findings confirmed dilated stomach and duodenum with a narrow aorto-mesenteric angle due to short and hypertrophic ligament of Treitz [Table/Fig-2]. Short and hypertrophic ligament of Treitz was divided and duodenojejunostomy was done. In postoperative period, parentral nutrition was continued for a week and the patient had an uneventful recovery.
Dilated stomach and duodenum on barium meal
Non passage of barium on delayed (90 minutes) images.
Intra operative image showing grossly dilated stomach and duodenum
Discussion
SMA syndrome was first described by Von Rokitanski in 1861 [1]. The incidence of this condition varies from 0.013-0.3% in barium series of upper GI tract. In human beings, due to the erect posture, the superior mesenteric artery leaves the aorta at an acute downward angle. It is through this vascular angle, between the aorta and the SMA that the third part of the duodenum passes and is thus vulnerable to becoming pinched in between the SMA anteriorly and the aorta and vertebral column posteriorly [2]. The aorto-mesenteric angle and aorto-mesenteric distance are reduced in SMA syndrome with values of 6 – 15 degree ( normal 28-65 degree) and 2-8 mm (normal 10-34mm) respectively [3]. The common causes include exaggerated lumbar lordosis, external compression by a body cast used for treatment of vertebral fracture or lumbar lordosis [3]. However, a rare aetiology is a short and hypertrophic ligament of treitz, which brings the duodenum into the vascular angle between the SMA and the aorta [4].
Patients usually present acutely with features of duodenal obstruction, with symptoms getting relieved on lying prone. Plain abdominal X-ray demonstrates gastric dilatation. Endoscopic examination usually does not indicate the diagnosis. On barium meal, a positive diagnosis of SMAS can be made in the presence of duodenal dilatation, retention of barium within the duodenum, vertical linear extrinsic pressure in the third portion of the duodenum and a positive Hayes manoeuvre [5]. Computed tomography (CT) has the advantage of demonstrating the characteristic duodenal distension and the close proximity of superior mesenteric vessels with aorta [6].
Surgery is the preferred modality of treatment. Various surgical procedures have been described. Isolated division of the hypertrophic ligament has a high failure rate. Preferred treatment options include gastrojejunostomy or duodenojejunostomy [7].
Our case represents a rare case of proximal small bowel obstruction due to short and hypertrophic ligament of treitz leading to a narrow aorto mesenteric angle. Division of this ligament and duodenojejunostomy lead to marked improvement of the symptoms as well as nutritional status of the patient. On follow-up, patient is asymptomatic for three years with normalization of BMI and nutritional parameters.
Conclusion
SMA syndrome is an uncommon cause of duodenal obstruction that should be considered once luminal pathologies have been ruled out by endoscopy. Short and hypertrophic ligament of Treitz is one of the rare causes of SMAS. Surgery offers a safe and complete cure for the same.
[1]. Rokitansky CV, Lehrbuch der patologische Anatomie, 3rd edn, vol 3 1861 3(3)ViennaBraumuller:187 [Google Scholar]
[2]. Akin ST, Skandalakis JE, Gray SW, The anatomic basis of vascular compression of the duodenumSurg Clin North Am 1974 54:1361-70. [Google Scholar]
[3]. Rudinsky SL, Matteucci MJ, Emergency department presentation of superior mesenteric artery syndrome: two cases in marine corps recruitsJ Emerg Med 2012 42:155-58. [Google Scholar]
[4]. Akin JT, Vascular compression of the duodenumSurgery 1976 79:512-22. [Google Scholar]
[5]. Lukes PJ, Rolny P, Nilsson AE, Diagnostic value of hypotonic duodenography in superior mesenteric artery syndromeActa Chir Scand 1978 144:39-43. [Google Scholar]
[6]. Applegate GR, Cohen AJ, Dynamic CT in superior mesenteric artery syndromeJ Comput Assist Tomogr 1988 12:976-80. [Google Scholar]
[7]. Pasumurthy LS, Ahlbrandt DE, Srour JW, Abdominal pain in a 20-year-old womanCleve Clin J Med 2010 771:45-50. [Google Scholar]