Isolated Non-Necrotising Granulomatous Vasculitis of the Gall Bladder- A Rare Entity
Priavadhana Rajan Prasaad1, Shubhranshu Shekhar2, S. Anu Priyadharshini3
1 Assistant Professor, Department of Pathology, Sree Balaji Medical College, Chennai, Tamil Nadu, India.
2 Assistant Professor, Department of Pathology, Sree Balaji Medical College, Chennai, Tamil Nadu, India.
3 Junior Resident, Department of Pathology, Sree Balaji Medical College, Chennai, Tamil Nadu, India.
NAME, ADDRESS, E-MAIL ID OF THE CORRESPONDING AUTHOR: Dr. Priavadhana Rajan Prasaad, No. 70, LIG, NH-1, Thayumanavar street, Maraimalai Nagar, Chennai-603 209, India. Phone : 9677685015, E-mail : vadanamuru@gmail.com, rajankpondy@yahoo.com
Gall bladder diseases are a significant cause of morbidity and mortality worldwide. Gall bladder diseases comprise a wide spectrum of disease entities including non specific inflammatory diseases, acute and chronic cholecystitis, follicular cholecystitis, granulomatous cholecystitis, metaplasic and dysplastic diseases of the gall bladder mucosa, gall bladder polyps and carcinomas. Here, we describe an unusual and a rare case of granulomatous vasculitis of the gall bladder incidentally diagnosed in a 38-year-old female, in a routine cholecystectomy specimen. Granulomatous vasculitis has been reported as a part of localised vasculitis of the gastrointestinal tract in the literature. The case is presented here for the rarity of the diagnosis of an isolated non-necrotising granulomatous vasculitis of the gall bladder.
Follicular cholecystitis, Granulomatous vasculitis, Gallstones
Case Report
A 38-year-old female presented to the surgery department of our hospital with symptoms of cholecystitis and was managed conservatively. She had similar complaints after six months and underwent cholecystectomy. The specimen was received in the Department of Pathology and routine histopathological examination was done.
Gross Findings: The gall bladder specimen was measuring 6.5cm in length and the wall was smooth and thickened. Cut surface revealed a thickened gall bladder wall with a granular and brown pigmented mucosal surface. No gall stones were identified. No other gross abnormality noted [Table/Fig-1].
Gross photomicrograph of cholecystectomy specimen- cut surface showing granular brown pigmentation with thickened wall

Microscopy
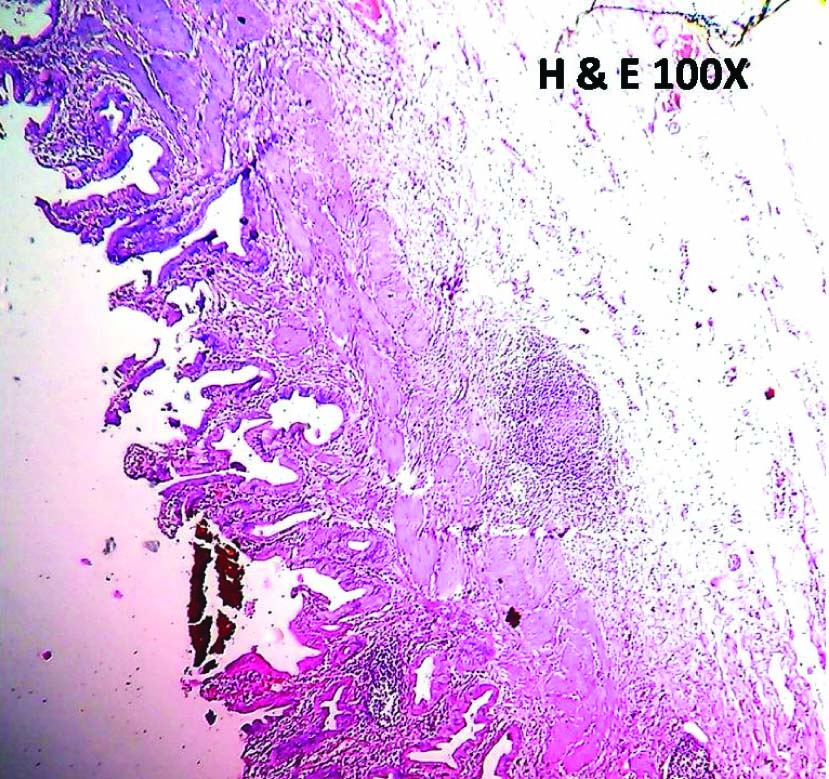
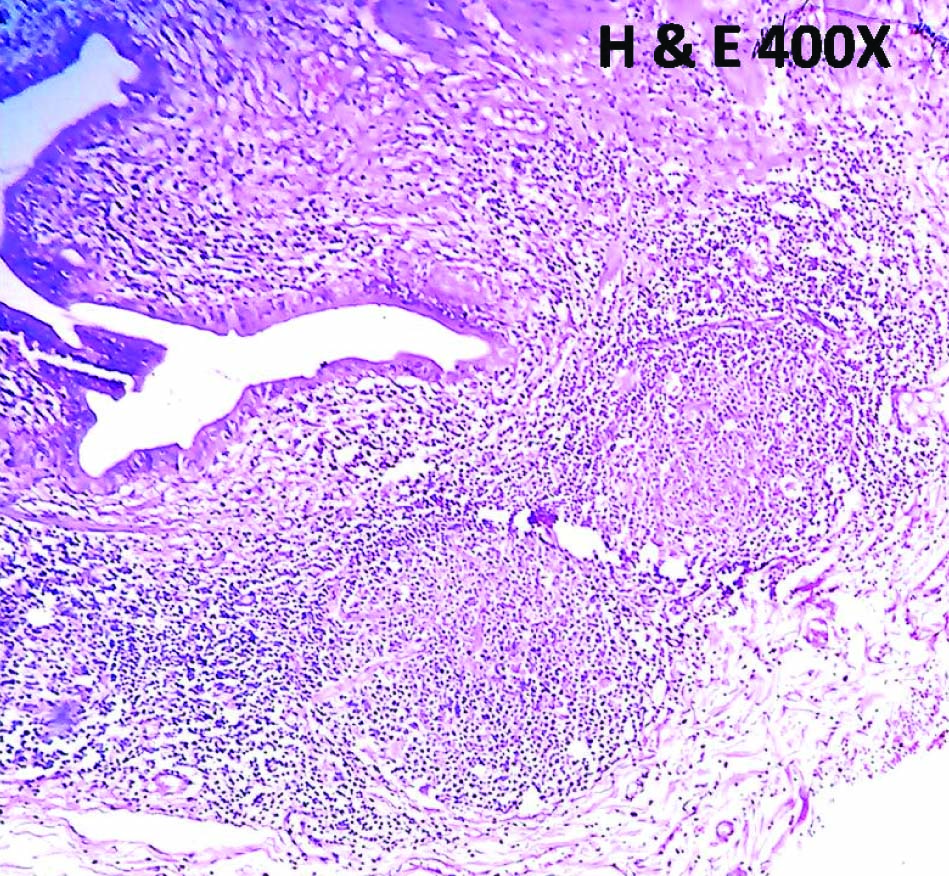
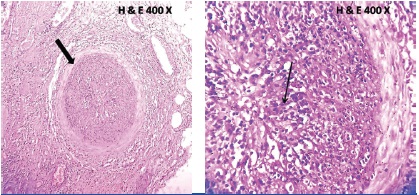
Sections from the gall bladder specimen showed features of chronic cholecystitis with Rokitansky-Aschoff sinuses and chronic inflammatory infiltrate composed of lymphocytes, macrophages and few eosinophils in the lamina propria along with lymphoid follicles [Table/Fig-2]. In addition, the muscular surface showed two isolated reactive lymphoid follicles with germinal centres [Table/Fig-3] and a small non-necrotising granuloma with epitheloid cell aggregates and lymphocytes. Along with this, also seen was a full thickness non-necrotising granuloma involving a small sized vessel in the serosal surface [Table/Fig-4,5]. There were no necrosis or giant cells within the granuloma. With these features, a diagnosis of non-necrotising granulomatous vasculitis of the gall bladder was considered. Further histochemical stains were done using Ziehl-Neelsen stain for tuberculosis and Periodic Acid Schiff stain for fungal aetiology and both were negative indicating the absence of any specific organism.
Low power view showing gall bladder mucosa with Rokitansky-Aschoff sinuses and lamina propria showing chronic inflammatory infiltrate –chronic cholecystitis
Low power view of lymphoid follicles with germinal centres in the muscular and serosal layer
Low power and high power view of non-necrotising granuloma in the small sized vessel with epitheloid cells and lymphocytes surrounded by dilated blood filled capillaries
The patient was followed up and evaluated for systemic vasculitis and serological screening with ANA, dsDNA, endomysial antibodies, p-ANCA and c-ANCA were done. All serological markers were negative. Radiological screening of the biliary tract and liver did not reveal any underlying abnormality.
Hence, a systemic component of vasculitis was ruled out and a diagnosis of isolated non-necrotising granulomatous vasculitis of the gall bladder was reported.
Discussion
Isolated non-necrotising granulomatous vasculitis of gall bladder (NNGV) is a very rare entity with only a few cases published in literature. Lasser et al., [1] reported a case of necrotising granulomatous vasculitis of gall bladder presenting as acute cholecystitis. Despite extensive investigations no systemic immunological disorder was identified in this case.
NNGV is an entity which comes under the spectrum of localised vasculitis of the gastrointestinal tract (LVGT). Localised vasculitis of the gall bladder was reported as a part of the LVGT. LVGT is an uncommon form of vasculitis that can be associated with significant morbidity and mortality. Burke AP et al., [2] showed that 19 out of 33 diagnosed cases (58%) of polyarteritis nodosa had localised manifestations of vasculitis in the gall bladder and small intestines only. The significance of NNGV and LVGT lies in diagnosing the underlying systemic immunologic conditions frequently associated with vasculitis of any organ. Gall bladder abnormalities are frequently a part of systemic immunological disorders especially primary sclerosing cholangitis.
Genaro Vazquez Elizondo et al., [3] showed in their study on 286 patients that cholecystitis is more frequently associated with sclerosing cholangitis with significant extrahepatic involvement than in cases with intrahepatic involvement. They have also concluded that cholecystectomy should be considered in patients with sclerosing cholangitis. Kumar B et al., [4] have reported two cases of necrotising granulomatous vasculitis of the gall bladder associated with systemic polyarteritis nodosa. They have also concluded that localised involvement of the gallbladder in Polyarteritis nodosa is a rare incidental finding, the serological work-up for autoantibodies may be negative and the disease is likely to remain self-limited.
Lymphoid follicles are not an infrequent finding in the resected gall bladder specimens. Chronic follicular cholecystitis (CFC) is an entity which has lymphoid follicles distributed throughout the wall of gall bladder. Chronic follicular cystitis has an incidence of 2%, all cases associated with salmonellosis. Tomori H et al., [5] studied 1341 patients of which 11.8% of the patients showed lymphoid follicles in the lamina propria of the gall bladder which later turned out to be diagnosed as low grade maltomas. Albores-Saavedra et al., [6] studied five cases of chronic cholecystitis with focal lymphoid hyperplasia (CCLH) which later were diagnosed as low grade lymphomas. In our study, two distinct lymphoid follicles with germinal centre formation were seen in the muscular layer. Further immunohistochemical confirmation to rule out a monoclonal proliferation of lymphoid cells is necessary in all cases of follicular cholecystitis.
Granulomas in the gall bladder are an infrequent finding in histopathological examination. In a study conducted on 1100 patients in Northern region of India, Mohan H et al., [7] have reported granulomas in resected specimens of gall bladder in which 2.3% cases were showing features of xanthogranulomatous cholecystitis, 2.3% showed follicular cholecystitis and 0.9% cases showed ceroid granulomas.
Siddiqui et al.,[8] have studied the importance of histopathological examination of all resected gall bladder specimens and concluded that systematic examination of the gall bladder specimens is mandatory as the underlying systemic immunological disorders can be diagnosed based on histopathological evidences.
Conclusion
The case is presented here for the rarity of the diagnosis of an isolated non-necrotising granuloma of the gall bladder and to emphasize that systematic histopathological evaluation of the cholecystectomy specimens may pave way for the diagnosis of systemic immunological and haematological disorders like primary sclerosing cholangitis/classic polyarteritis nodosa and low grade lymphomas.
[1]. Lasser A, Ghofrany S, Necrotising granulomatous vasculitis (allergic granulomatosis) of the gall bladderGastroenterology 1976 71:660-62. [Google Scholar]
[2]. Burke AP, Sobin LH, Virmani R, Localized vasculitis of the gastrointestinal tractAm J Surg Pathol 1995 19(3):338-49. [Google Scholar]
[3]. Genaro VE, Jimena MB, Nahum MS, Gallbladder disease in patients with primary sclerosing cholangitisAnnals of Hepatology 2008 7(2):182-83. [Google Scholar]
[4]. Kumar B, Krishnani N, Misra R, Pandy R, Isolated necrotising vasculitis of gall bladder:a report of two cases and review of literatureIndian J of Pathol Microbiol 2003 46(3):429-31. [Google Scholar]
[5]. Tomori H, Nagahama M, Miyazato H, Shiraishi M, Muto Y, Toda T, Mucosa associated lymphoid tissue (MALT) of the gall bladder:a clinicopathological correlationInt Surg 1999 84(2):144-50. [Google Scholar]
[6]. Albores SJ, Gould E, Manivel RC, Angeles AA, Henson DE, Chronic cholecystitis with lymphoid hyperplasiaRev Invest Clin 1989 41(2):159-64. [Google Scholar]
[7]. Mohan H, Punia RPS, Dhawan SB, Atal S, Sekhon MS, Morphological spectrum of gallstone disease in 1100 cholecystectomies in North IndiaIndian J Surg 2005 67:140-42. [Google Scholar]
[8]. Siddiqui FG, Memon AA, Abro AH, Sasoli NA, Ahmad L, Routine histopathology of gallbladder after elective cholecystectomy for gall stones: waste of resources or a justified act?BMC Surg 2013 13:26 [Google Scholar]