Altered Lung Function Test in Asymptomatic Women Using Biomass Fuel for Cooking
Jeneth Berlin Raj T1
1 Assistant Professor, Department of Physiology, Mahatma Gandhi Medical College and Research Institute, Karpaga Vinayaga Institute of Medical Sciences, Tamil Nadu, India.
NAME, ADDRESS, E-MAIL ID OF THE CORRESPONDING AUTHOR: Dr. Jeneth Berlin Raj. T, Bharathidasan Street, Indira Nagar Extension, Gorimedu, Pondicherry- 605006, India.
Phone: 9994737997/8925457292, E-mail : berlin_jbr@yahoo.com
Background: One third of the world’s population use biomass fuel like wood, dung or charcoal for cooking. The smoke from these organic materials increases the incidence of respiratory illness including chronic obstructive pulmonary disease and lung cancer.
Aim: To evaluate forced expiratory lung volumes in asymptomatic women previously exposed to biomass fuel smoke.
Materials and Methods: The study was done in 74 healthy asymptomatic women divided into two age matched groups of 37 each. Pulmonary function tests (PFT) were assessed by computerised spirometry and statistical comparisons done on women using biomass fuel (study group) and women using other sources of fuel (LPG/ electric stove) for cooking (control group).
Results: The PFT results showed significant reduction in forced expiratory lung volumes like Forced Vital Capacity (FVC), Forced Expiratory Volume in 1st sec (FEV1), Forced Expiratory Flow between 25-75% (FEF 25-75%) and Forced Expiratory Volume percentage (FEV1%) in biomass fuel users as compared to those not exposed to biomass fuel smoke.
Conclusion: The results of this study suggest that biomass fuel smoke may produce definite impairment in lung function, especially with regard to the smaller airways.
Biomass fuel users, Computer spirometry, Forced expiratory lung volumes, Impaired lung function test
Introduction
In developing countries like India, about three-quarters of the Indian households use unprocessed fuel like firewood, dung cakes, crop residues (straw, grass, and shrubs), coal and kerosene for domestic cooking. The percentage of households using biomass stove in rural and urban area constitute to 90% and 32% respectively. In rural India, firewood is used as biomass fuel in 62% of households, 14% cook with dung cake and 13% use other biomass source. In urban India, 22% of households use firewood, 8% use kerosene and 70% of households use cleaner fuels like LPG or electric stoves [1].
According to recent statistics from World health Organisation (WHO) in 2012, solid fuels like firewood are used for domestic uses by 65% of the Indian population [2]. Because of customary involvement in cooking, women are more exposed to biomass fuel than men [3]. In developing countries, girls start cooking at the age of 15 and spend an average of 4-6 h daily for cooking. Therefore during their lifetime, females are exposed to biomass smoke for 30-40 y, equivalent to 60,000 hours of exposure, inhaling 25 million litres of polluted indoor air [4].
Biomass fuel combustion produces suspended particulate matter of respirable size (PM < 10μ) like carbon monoxide, nitrous oxide, sulphur oxides (principally from coal), formaldehyde and polycyclic organic matter including carcinogens such as benzopyrene [5]. Particles with diameter smaller than 10μ particularly those smaller than 2.5μm (PM < 2.5 μ) can penetrate deep into the lungs and appear to have the greatest potential for damaging health status. Studies have shown remarkable consistency in the relationship between change in daily ambient suspended particulate levels and subsequent changes in mortality [6].
Long term exposure to biomass fuel combustion smoke is associated with many respiratory diseases like acute respiratory infection (mostly in children under 5 years), chronic obstructive pulmonary disease, asthma, lung cancer, pulmonary tuberculosis, pneumoconiosis and interstitial lung disease [7]. It is against this backdrop that this study was initiated to understand the effect of biomass fuel smoke on lung function in asymptomatic women.
Materials and Methods
This study was done in 74 healthy asymptomatic females in two groups of 37 each working in a tertiary care teaching hospital in Tamil Nadu, South India. The study group consisted of 37 class D workers (Ayammas) between the age group of 25- 44 years who were using biomass fuel (mainly firewood) for cooking. The control group consisted of 37 age, height, weight and BMI matched female staff members using either LPG or electric stove i.e. they were not exposed to biomass fuel smoke. Both the groups were cooking for a minimum period of 3 years. The study group subjects had a history of exposure to biomass fuel smoke for a minimum of 3 hours daily. The subjects were given clear explanation about the aim, methodology and possible implications prior to the commencement of the study. Written informed consent was obtained from all subjects. A preliminary screening was done to exclude gross pulmonary diseases, anatomical deformity of the chest or spine and any infectious aetiology like TB that may affect respiratory functions. Subjects with any of these conditions were excluded from the study. The selected subjects were interviewed with a standard respiratory questionnaire based on American Thoracic Society (ATS) and European Respiratory Society (ERS) guidelines [8].
Pulmonary function tests were carried out using computerized spirometer (MEDIKRO WINDOWS SPIROMETER / MODEL – M 9831-1-8-0.4). Satisfactory demonstrations were given to the subjects regarding the procedure for recording the forced expiratory lung volumes like Forced Vital Capacity (FVC), Forced Expiratory Volume in 1st sec (FEV1), Forced Expiratory Flow 25-75% (FEF 25-75%), Peak Expiratory Flow Rate (PEFR) and Forced Expiratory Volume % (FEV1%) prior to the test. The subjects were allowed to relax and familiarize with the procedure. After attaching the nose clip, the subjects were asked to take a deep inspiration and blow into the mouthpiece as rapidly, forcefully and completely as possible while keeping their lips tightly sealed around the mouthpiece to prevent escape of any air through the sides of the mouthpiece. A minimum of three forced expiratory maneuvers were performed and the best of three readings was selected for statistical analysis [9]. The standard guidelines of ATS and ETS were strictly followed throughout the procedure.
Results
The effect of biomass fuel smoke exposure on forced expiratory lung volumes was assessed in healthy asymptomatic biomass fuel using females and the data was compared with healthy females matched for age, height, weight and BMI [Table/Fig-1].
Anthropometric measurements of study and control groups Both groups were comparable as p-value for inter-group comparisons was > 0.05
| Variable | Study Group (N=37) (Mean ± SD) | Control Group (N=37) (Mean ± SD) |
|---|
| Age (yrs) | 34.27 ± 5.45 | 34.27 ± 5.45 |
| Height (cm) | 155.68 ± 6.08 | 155.49 ± 6.24 |
| Weight (kg) | 49.08 ± 5.83 | 48.78 ± 7.49 |
| BMI | 20.3 ± 2.28 | 20.17 ± 2.79 |
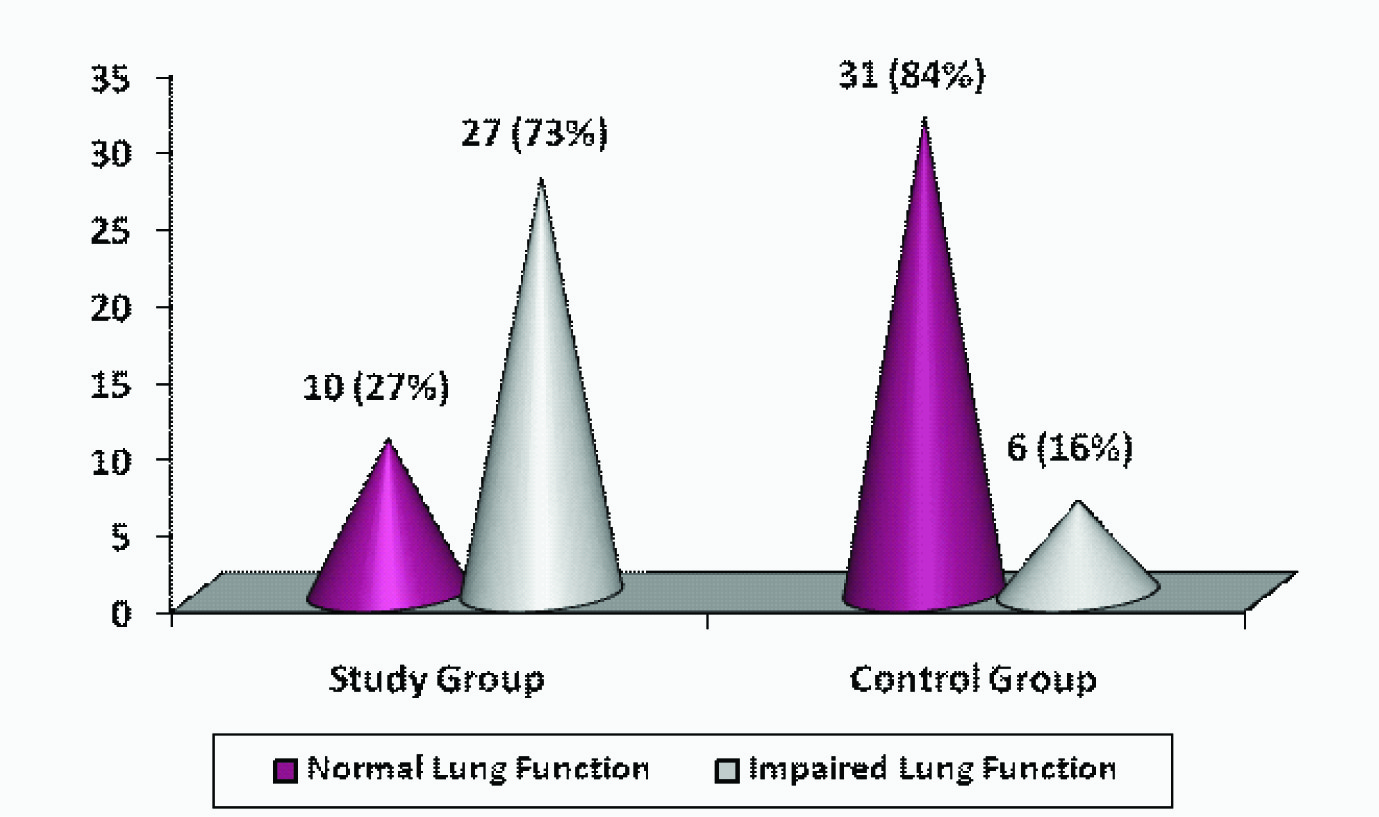
Upon comparison of pulmonary function in both groups it was observed that almost 3/4th of the women using biomass fuel had impaired lung function test [Table/Fig-2]. The relative risk (RR) of getting impairment in lung function is 4.5 times more in the biomass users as compared to the controls not exposed to biomass fuel. The 95% confidence interval for RR was 2.05 to 9.78 which is significant.
PFT results for both groups based on FEV1 test value according to ATS/ERS recommendation 2005
Discussion
Chronic exposure to biomass fuel smoke is associated with macrophage infiltration in intra alveolar space, bronchial wall and sputum indicating active inflammatory process. Histopathological lung changes observed were septal enlargement, fibrosis, bronchitis, glandular hyperplasia and goblet cell metaplasia [10]. All these changes lead to airway obstruction resulting in gradual deterioration of lung function.
FVC, FEV1, FEV1% values are better indicators for measuring generalised airway obstruction. These parameters are also used to differentiate obstructive lung diseases from restrictive lung diseases. In the present study, all these parameters were lower in biomass fuel users when compared to controls not exposed to biomass fuel combustion smoke [Table/Fig-3]. This result suggest that biomass fuel definitely produces airway obstruction which may be due to the inflammatory reaction in pulmonary airways caused by suspended particles in biomass fuel smoke. Similar decrease in FVC, FEV1, FEV1% was observed in a study by Regalado et al., in rural Mexican women [11]. Reduction of all the forced expiratory lung function parameters indicates an obstructive type of lung disease.
Forced expiratory lung volumes in study and control group
| Lung function parameters | Study Group (n=37) | Control Group (n=37) | Student t-test |
|---|
| Ref.Value (Mean ± SD) | Test.Value (Mean ± SD) | % Ref. (Mean ± SD) | Ref.Value (Mean ± SD) | Test.Value (Mean ± SD) | % Ref. (Mean ± SD) |
|---|
| FVC (litres) | 2.4±0.24 | 1.96±0.34 | 81.6±10.5 | 2.39±0.24 | 2.22±0.42 | 92.38±12.2 | 0.007 |
| FEV1 (litres) | 1.96±0.18 | 1.61±0.3 | 81.9±11.7 | 1.94±0.18 | 1.8±0.31 | 92.9±10.86 | 0.006 |
| FEF 25 – 75 % (l/sec) | 3.49±0.25 | 3.29±0.27 | 94.15±4.5 | 3.45±0.25 | 3.4±0.46 | 98.54±9.56 | 0.01* |
| PEFR (l/sec) | 6.44±0.41 | 6.53±0.46 | 101.3±3.3 | 6.39±0.39 | 6.34±0.57 | 99.2±6.43 | 0.12 |
| FEV1% | 81.72±1.11 | 83.36±1.8 | 102.01±2.05 | 81.52 ±1.42 | 86.23 ±5.36 | 105.76 ±6.07 | 0.003 |
Note: - FEF 25 – 75 % Reference value – p-value*
When compared with control group, all the forced expiratory lung volume parameters except PEFR were significantly lesser in study group subjects indicating the silent ill effect of biomass fuel smoke
FEF 25-75% is one of the most sensitive indicators to determine the patency of small airways with diameter less than 2mm. The FEF 25-75% test value in this study was significantly reduced in study group when compared to control group indicating the presence of smaller airway obstruction. Suspended particles of biomass fuel combustion < 2.5 μm can penetrate deeply into the lungs and affect the smaller airways as well as the lung parenchyma. This is the reason for decreased FEF 25-75% value in biomass fuel users. Our finding is in agreement with the previous study by Revathi et al., [12].
Peak expiratory flow rate is determined to assess the caliber of larger airway and to distinguish between reversible and irreversible lung disease. In the present study, the reduction in test value of PEFR was not statistically significant. This can be explained on the postulate that biomass fuel mostly affects the smaller airways and that the lesions may be reversible.
Conclusion
Significant reduction in FEF 27-75% and not PEFR in this study suggests that suspended particles emitted during biomass fuel combustion predominantly affects the smaller airways.
Early detection of smaller airway damage by FEF 25-75% is at risk population can be used as a potential diagnostic tool in clinical scenario as the progress of the disease can be arrested or even reversed if the person is withdrawn from the pollutant.
Further studies are required to substantiate such reversal of smaller airway disease and to study the improvement in lung function when such subjects are withdrawn from the pollutant.
Note: - FEF 25 – 75 % Reference value – p-value*
When compared with control group, all the forced expiratory lung volume parameters except PEFR were significantly lesser in study group subjects indicating the silent ill effect of biomass fuel smoke
[1]. International Institute of population Sciences (IIPS)National family health survey (MCH and family planning): India 2005-2006 2007 Bombay. InInternational Institute of Population Sciences [Google Scholar]
[2]. World Health Organization. The World health statistics:2012. Available from http://www.who.int/whois/whostat/2012/en/- (Accessed September 24, 2012) [Google Scholar]
[3]. Behear D, Dash S, Malik S, Blood carboxy haemoglobin levels following acute exposure to smoke of biomass fuelIndian Journal of Medical Research. 1998 88:522-42. [Google Scholar]
[4]. Salvi S, Barnes PJ, Is exposure to biomass smoke the biggest risk factor for COPD globally?Chest 2010 138:3-6. [Google Scholar]
[5]. Ezzati M, Kammen DM, The health impacts of exposure to indoor air pollution from solid fuels in developing countries: knowledge, gaps and data needsEnviron Health Perspect 2002 110:1057-68. [Google Scholar]
[6]. Smith KR, Indoor air pollution in developing countries: growing evidence of its role in the global disease burdenIn: Indoor Air, 96: Proceedings of 7th International conference on indoor air climate. Ikedak, Iwata T, eds 1996 Tokyo, JapanInstitute of public health:33 [Google Scholar]
[7]. Prasad R, Singh A, Garg R, Giridhar B, Hosmane Biomass fuel exposure and respiratory diseases in IndiaBioscience Trends. 2012 6(5):219-28. [Google Scholar]
[8]. Brausasco V, Viegi Crapo R, Series ATS/ERS task force: Standardisation of lung function testingEur Respir J 2005 26:948-68. [Google Scholar]
[9]. Raj JB, Loganayaki R, Rajakumar D, Effect of cigarette smoking on forced expiratory lung volumes in asymptomatic smokersInt J Cur Res Rev. 2013 5(10):38-42. [Google Scholar]
[10]. Mena MA, Woll F, Cok J, Ferrufino JC, Accinelli RA, Histopathological lung changes in children due to biomass fuelAm J Respir Crit Care Med. 2012 185:687-88. [Google Scholar]
[11]. Regalado J, Prez-Padilla R, Sansores R, The effect of biomass burning on respiratory symptoms and lung function in rural Mexican womenAm J Respir Crit Care Med 2006 174(8):901-05. [Google Scholar]
[12]. Revathi M, Kutty TK, Annamalai N, Pulmonary function in rural women exposed to biomass feulJ Pulmon Resp 2012 2(7):133 [Google Scholar]