Bilateral Absence of Musculocutaneous Nerve: A Case Report
Aniruddha Sarkar1, Anubha Saha2
1Associate Professor, Department of Anatomy, Midnapore Medical College, Midnapore, West Bengal, India.
2Assistant Professor, Department of Anatomy, Institute of Post-Graduate Medical Education & Research, Kolkata, West Bengal, India.
NAME, ADDRESS, E-MAIL ID OF THE CORRESPONDING AUTHOR: Dr. Aniruddha Sarkar, 48, Sreenagar Main Road, Kolkata, West Bengal-700094, India.
E-mail: drani77@gmail.com
Detailed knowledge of course and distribution of nerves in the axilla and arm is very important in the management of nerve injuries particularly in case of their variations. Bilateral absence of the musculocutaneous nerve was found during routine dissection in a male cadaver. The dissected part was cleared to see the distribution of the muscles of the arm. The muscles of the flexor compartment were supplied by the median nerve, instead of the musculocutaneous nerve. The present case report of this anatomical variation of the nerves should help in management of nerve injuries in the axilla or the arm.
Musculocutaneous nerve, Median Nerve, Variation
Case Report
During routine dissection of the arm for the undergraduate students absence of musculocutaneous nerve was noted bilaterally. All the flexor muscles of the arm were supplied by the median nerve except the coracobrachialis of left side supplied by a twig from the lateral cord of the brachial plexus.
Nerve to the coracobrachialis of left side arises 6 centimeter (cm) distal to the outer border of the first rib from the lateral cord of brachial plexus after the usual emergence of the lateral pectoral nerve [Table/Fig-1] and further 6 cm away nerve for biceps brachii appears from lateral root of median nerve (i.e. 12 cm from outer border of first rib) [Table/Fig-2]. Left median nerve is formed by the union of the two roots14 cm from outer border of first rib [Table/Fig-2]. The brachialis muscle is supplied by another branch of left median nerve about 18 cm away from outer border of the first rib [Table/Fig-2]. After supplying brachialis muscle the nerve has crossed the elbow joint deep to the bicipital-aponeurosis [Table/Fig-2] to pierce the deep fascia lateral to the biceps brachii tendon and emerged out just as the lateral cutaneous nerve of the forearm.
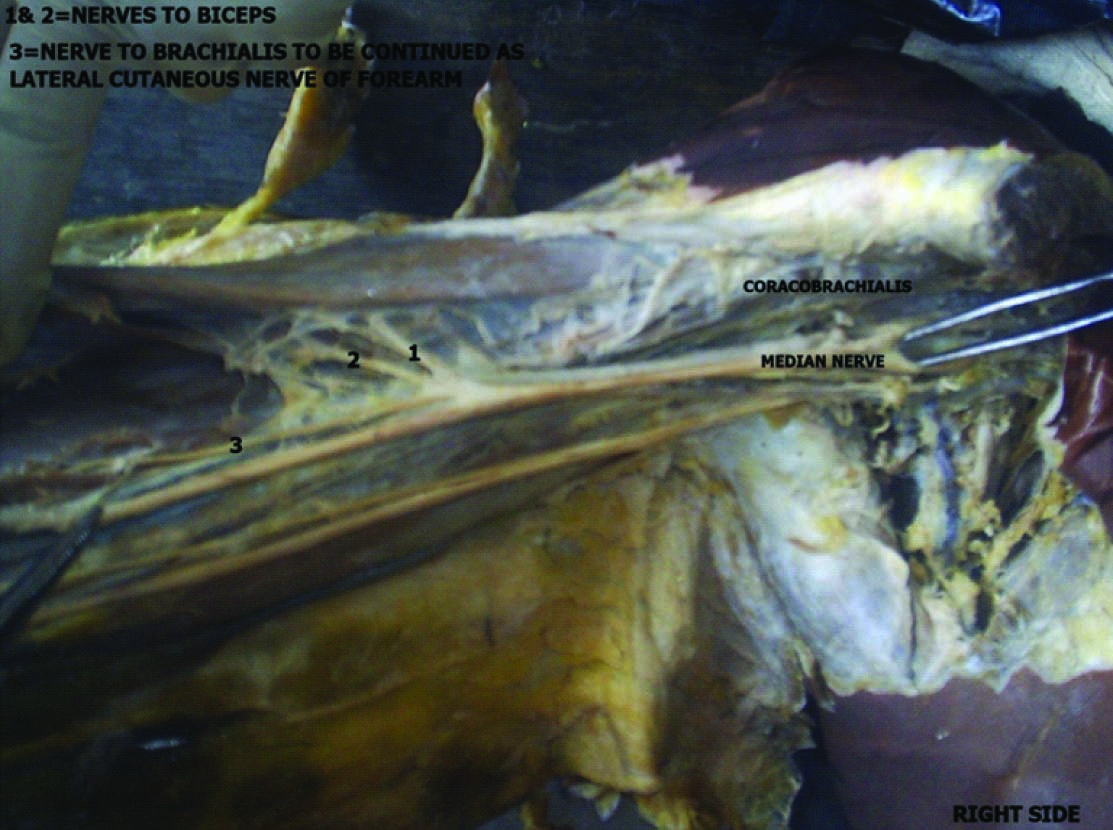
In right side, nerve to coracobrachialis is given from the lateral root of the median nerve 4 cm distal to the outer border of the first rib. Then 15 cm away from the outer border of the first rib three branches appeared from the median nerve in arm, two branches for the biceps brachii and one branch to the brachialis. Brachialis is supplied by a twig passing through the muscle and then the nerve became lateral cutaneous nerve of the forearm as in the opposite side[Table/Fig-3].
Union of two roots of median nerve is at lower level on left side than the right.
Discussion
Musculocuataneous (MC) nerve variation is very much common and several studies have been done to see the variations.In the study of Gumusburun & Adiguzel bilateral absence of musculocutaneous nerve have been shown in which the lateral cord of brachial plexus consisted of anterior divisions of upper and middle trunks and two branches appeared to supply the coracobrachialis muscle; the lateral root of the median nerve included the fibres of the musculocutaneous nerve [1]. Complete absence of musculocutaneous nerve have been reported by Bhojak NR et al., [2] in 4% of cases and Jamuna M [3] observed it in 6% of their cases. But the musculocutaneous nerve rejoins the median nerve in 2% of cases in both the studies. Complete absence of the musculocutaneous nerve is a very rare anomaly and it is reported by few authors like Sud et al., [4], Sharmila Bhanu et al., [5]and Ravishankar et al., [6].
Variations in the course and branches of the musculocutaneous nerve have been noted in works of Bergman et al., [7]. Multiple communications between the musculocutaneous nerve and the median nerve have been observed by Chouhan et al., [8]. In the present case report the lateral cord and the median nerve are supplying the muscles of the anterior compartment of arm bilaterally. In the study of Chakrabarti S also bilateral absence of musculocuataneous nerve have been shown where the median nerve is supplying all the flexor muscles of both the arm, after supplying the coracobrachialis and biceps a common branch have been given for the brachialis and lateral cutaneous nerve of forearm [9]. In the present study, only left coracobrachialis is supplied by a twig from lateral cord but in study of Sharmila Bhanu and Devi Sankar coracobrachialis of both arm is supplied by lateral cord [4]. In the present case report, after giving supply to brachialis the branch of the median nerve is continuous as lateral cutaneous nerve of forearm similar to other studies. In absence of musculocutaneous nerve the fibres are passing through the median nerve which is also supported by Ojaswini Malukar and Ajay Rathva [10]. Meenakshi sundaram J has reported a case of unilateral absence of MC nerve where the author has explained it due to the abnormal formation of the axillary artery [11]. Nasr AY has reported in his study that in 3.3% cases of absence of MC nerve all the flexor arm muscles are supplied by the median nerve corroborative with the present study [12].
Here the first branch of the median nerve is most probably representing the MC nerve in the left side. The other front muscles of left arm are supplied by the branches arising from the median nerve at different levels. In the right side the nerve to coracobrachialis is arising slightly above than the left side and it can be compared withthe MC nerve as per the location so that it can be said that the fibres of MC nerve are passing through the median nerve. Supply to other front muscles of right arm is totally different from the left side. Thenerve passing through the brachialis continued as lateral cutaneous nerve of forearm after piercing the deep fascia and so functionally representing the MC nerve. Most probably developmentally MCnerve is not so much important in the presence of median nervewhich can take the charge to supply the front muscles of arm.
The possible explanation of the absence of the musculocutaneous nerve, as in this case might be the failure of aggregation of all the ventral branches arising from the lateral cord of the brachial plexus to form the musculocutaneous nerve which normally supplies all the muscles of the anterior compartment of the arm. Instead of formation of musculocutaneous nerve all the segmental branches enter through the lateral root and pass through the median nerve. Along with the growth of the limb bud muscles, the nerves to supplythem also emerge from the lateral border of the median nerve as if the branches given off by the median nerve [13].
Clinical implications could be that the injury of the median nerve here will produce muscle weakness or paralysis of the flexor muscles of the arm which is unusual. Because lateral root of the median nerve and the musculocutaneous nerve are appearing from the same cord of the brachial plexus, i.e. lateral cord carrying the fibers C5,C6 and C7 roots. Normally in case of damage at the single root or multiple roots at C5,C6, C7 there is damage of all the flexor muscles of arm including a major damage of flexor muscles of forearm. But, in case of injury of both median and musculocutaneous nerves below the roots, paralysis/paresis of flexor group of muscles of both arm and fore-arm can occur simultaneously. In the presentcase report as there are no separate musculocutaneous nerves in both the upper limbs, whether the damage is at the root or at the cord level, paralysis or paresis should occur toall flexor muscles inboth the arm and fore-arm due to median nerve involvement.
From clinical, embryological and anatomical point of view the present case report is very much significant. The proper knowledge of such very rare anomaly will help to conclude the diagnosis and to carry out investigations accordingly.
The cause of such rare anomaly needs further investigations and studies. The probable explanation has been expressed embryologically for the presented case report. It may help for further research and would invite much more views regarding such anomalies.
Such type of neural anomaly might enrich our knowledge to remain conscious in surgical repair of nerves in brachial plexus injury or in other trauma to prevent unwanted outcomes.
Figure illustrating the anomalous lateral cord branching on left side After branch for coracobrachialis from lateral cord (1), nerve for biceps brachii comes out from lateral root of Median nerve (3), after which both the roots of Median nerve unite (2)
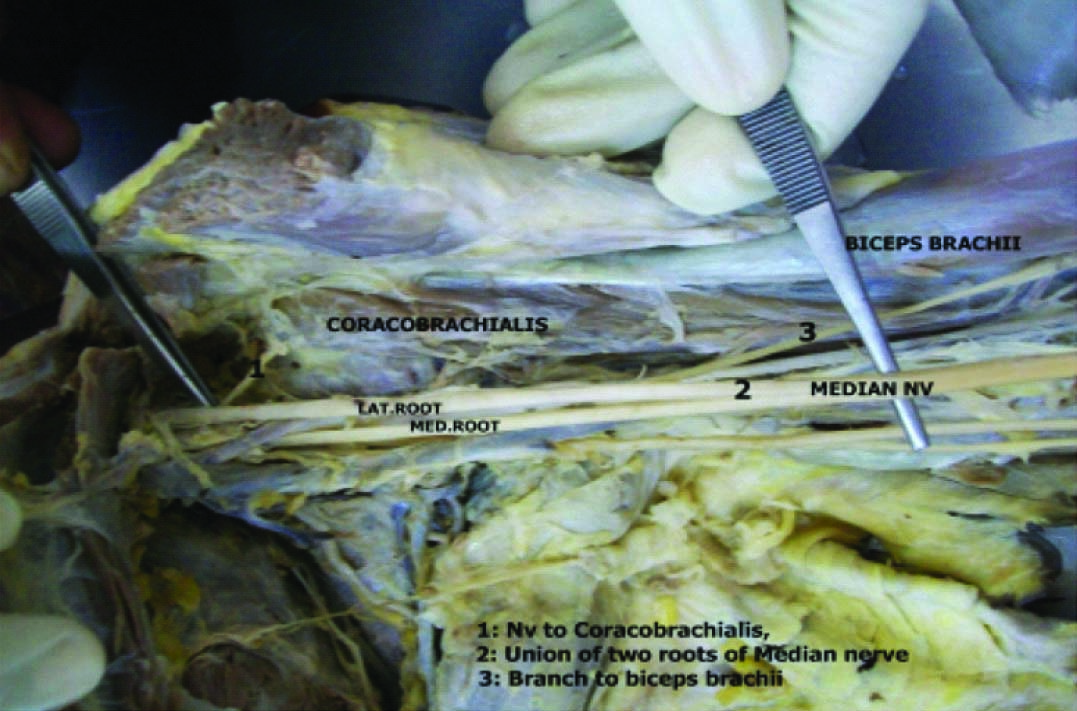
Figure demonstrating the anomalous branches of Median nerve on left side. Nerve to biceps brachii comes from its lateral root (1) and at the lower arm another branch comes out to supply the brachialis, after which it gets continued as Lateral cutaneous nerve of forearm (2)

Figure showing branch to coracobrachialis from median nerve on right side and branches to biceps (1&2) and branch to brachialis (3) from median nerve which continued as lateral cutaneous nerve of forearm
[1]. E Gumusburun, E Adiguzel, A variation of the brachial plexus characterized by the absence of the musculotaneous nerve-a case report.Surg Radiol Anat. 2000 22:63-65. [Google Scholar]
[2]. NR Bhojak, JP Patel, JN Desai, SH Ram, Anatomical variation in musculocutaneousnerve- A cadaveric study.NJIRM 2014 5(1):92-95. [Google Scholar]
[3]. M Jamuna, G Amudha, A cadaveric study on the anatomic variations of the musculocutaneous nerve in the infraclavicular part of the brachial plexus. J Clin Diagn Res (JCDR). 2011 5(6):1144-47. [Google Scholar]
[4]. M Sud, A Sharma, Absence of Musculocutaneous nerve and innervation of Choracobrachialis, Biceps brachii and Brachialis from the Median nerve.J Anat Soc India. 2000 49(2):176-77. [Google Scholar]
[5]. P Sharmila Bhanu, K Devi Sankar, Bilateral absence of musculocutaneous nerve with unusual branching pattern of lateral cord and median nerve of brachial plexus. Anat Cell Biol. 2012 45:207-10. [Google Scholar]
[6]. MV Ravishankar, PS Jevoor, L Shaha, Bilateral absence of musculocutaneous nerve.J Sci Soc. 2012 39(1):34-36. [Google Scholar]
[7]. RA Bergman, SA Thompson, AK Afiffi, FA Saadesh, Compendium of human anatomic variation.Urban & Schwarzeberg Munich. 1988 :139-43. [Google Scholar]
[8]. R Chauhan, TS Roy, Communication between the Median and Musculocutaneous nerve -a case report.J Anat Soc India. 2002 51(1):72-75. [Google Scholar]
[9]. S Chakrabarti, RK Subramanian, Absence of musculotaneous nerve bilaterally with variant motor innervations of flexors of arm.Published Online 2013 [Google Scholar]
[10]. O Malukar, A Rathva, A study of 100 cases of Brachial plexus.Nat J Comm Med. 2011 :166-70. [Google Scholar]
[11]. J Meenakshi Sundaram, A single common cordin the infraclavicular part of the brachial plexus.IJHSR 2012 2(2):108-11. [Google Scholar]
[12]. AY Nasr, Morphology and clinical significance of the distribution of the median nerve within the arm of human cadavers.Neurosciences 2012 17(4):336-44. [Google Scholar]
[13]. Limb Musculature. In: Sadler TW, editor. Langman’s Medical Embryology. 2004 9th EditionPhiladelphiaLippincott Williams & Wilkins.:203-06. [Google Scholar]