Objective: The present study was conducted to analyze the current prescription pattern and cost analysis of antihypertensive drugs in hypertensive patients in a tertiary care hospital.
Materials and Methods: A retrospective cross-sectional study was conducted in tertiary care hospital, Bangalore for three months and utilized 300 prescriptions for the analysis. The data analysed from the prescription included patients demographics, stage of hypertension according to JNC VII guidelines, type of drug therapy, class of anti-hypertensive, and cost effectiveness of therapy. Drug acquisition costs was calculated, using the cost of the cheapest available drug and the most commonly prescribed dosage, for each drug on a daily and annual basis. Total annual drug expenditure on buying required doses of all antihypertensive prescribed in the study population for a year was calculated.
Results: Monotherapy (48.94%) was leading trends of antihypertensive therapy followed by fixed dose combination (35.04%) and polytherapy (16.01%). The most frequent antihypertensive class to be prescribed were CCBs (38.59%) followed by beta blockers (24.07%). The ranking in terms of cost utilized per year from the highest to the lowest found in this study was: alpha blockers> ACE-inhibitors> ARBs> CCBs> beta blockers > diuretics. The diuretics were most cost-effective (Cost per day: 5.89 ± 2.87; Cost per year: 2129.02 ± 1080.49) in relation to the other antihypertensive prescribed.
Introduction
Hypertension has been reported to be the strongest modifiable global risk factor for cardiovascular morbidity, mortality as well as health burdens [1,2]. Epidemiological studies conducted in many parts of the world have consistently identified an important and independent link between hypertension and various disorders, especially coronary heart disease, stroke, congestive heart failure and impaired renal function [3].
Hypertension is currently the leading risk resulting in considerable death and disability worldwide and accounted for 9.4 million deaths and 7% of disability adjusted life years in 2010 [4]. In India, the situation is more alarming as hypertension attributes for nearly 10% of all deaths [5]. Prevalence of hypertension in India is reported to vary from 4-15% in urban and 2-8% in rural population [6]. It is estimated that the worldwide prevalence of hypertension would increase from 26.4% in 2000 to 29.2% in 2025 [7]. Epidemiological studies also demonstrate that prevalence of hypertension is increasing rapidly among Indian urban and rural populations [8].
Antihypertensive pharmacotherapy effectively reduces hypertension-related morbidity and mortality [9]. Over the past decade a range of clinical guidelines on antihypertensive treatment have been published with contributions from multiple clinical trials and studies [10,11]. The Joint National Committee (JNC) in 2003 published a series of guidelines recommend the appropriate antihypertensive therapy based on the best available evidence. The guidelines recommend Thiazide diuretics to be prescribed alone or as part of combination therapy for most hypertensive patients without compelling indications [11]. However, most recent published data showed an increasing use of the more expensive Calcium Channel Blockers (CCBs) and Angiotensin Converting Enzyme Inhibitors (ACEIs) despite the lack of evidence to support that they are superior to diuretics and beta blockers in reducing morbidity and mortality of cardiovascular diseases [12]. Despite broad dissemination of the JNC guidelines, prescribing practices have long remained discrepant with recommendations [13].
The cost of medications has always been a barrier in effective treatment. The increasing prevalence of hypertension and the continually rising expense of its treatment influence the prescribing patterns among physicians and compliance to the treatment by the patients.
The objective of the present study was to analyse the prescription pattern of antihypertensive drugs and adherence to JNC VII guidelines as well as to study the cost incurred during the treatment. Cost of the drug was obtained from current index of medical specialties (CIMS) [14].
Materials and Methods
This was a retrospective cross-sectional study conducted on patients attending the out-patient department of General Medicine of a Tertiary Care Hospital, Bangalore. The duration of the study was over three months from September to November 2013. Total 300 prescriptions were collected and data was analysed using SPSS version 20. Patients aged ≥ 18 y and diagnosed with hypertension were included in this study. We excluded patients with serious co morbid illness like congestive heart failure, chronic kidney disease, stroke, dementia, cognitive/ sensory deficits and also pregnant, lactating mothers.
The information collected from each prescription included the name, gender, age, recorded blood pressure (both systolic and diastolic), name of drugs (generic as well as brand name), dosage, frequency, type of therapy (monotherapy, polytherapy and fixed dose combination) and cost of the drugs. For brand-name and combination antihypertensive agents, each generic name (active ingredient) component of the agent was counted separately. Subsequently, each generic name was categorized into its major antihypertensive drug class. The drug costs were obtained from CIMS and universally applied to clinical facilities regardless of their size. Cost of drugs was obtained from the Current Index of Medical Specialties (CIMS) [14]. Drug acquisition costs was calculated, using the cost of the cheapest available drug and the most commonly prescribed dosage, for each drug on a daily and annual basis. Total annual drug expenditure (money spent on buying required doses of all antihypertensive prescribed in the study population for a year) was calculated. Drug expenditure due to a single drug was expressed as a percentage of total drug expenditure [15].
The JNC VII guideline was used to classify the stages of hypertension among the patients. Patients who were on antihypertensive medication with only one active ingredient were defined as receiving monotherapy; those taking two active ingredients in a combination pill were defined as receiving fixed dose combination (FDC) therapy and those who had been prescribed with two or more active ingredients were considered to be on polytherapy. The study protocol was approved by the Institutional Review Board and Ethics Committee of the hospital.
Statistical Analysis
Data collected from patients prescriptions were transferred to data entry format for evaluation. Continuous variables are presented as mean values ± standard deviation (SD) and categorical variables are presented as percentages. Cost analysis was done using ANOVA.
Results
The data were expressed as mean ± standard deviation. 300 prescriptions were included in the analysis. The demographics of the patients are given in [Table/Fig-1]. The patients were grouped according to the stages of hypertension as per the JNC VII guidelines. Based on the blood pressure recorded at the time of visit to the OPD, 8.66% of patients were found to have normal blood pressure, 25% were pre-hypertensives, 36.33% were at Stage 1 and 30% were at Stage 2 hypertension. The percentage corresponding to number of hypertensive patients, who received the type of medication is shown in [Table/Fig-1].
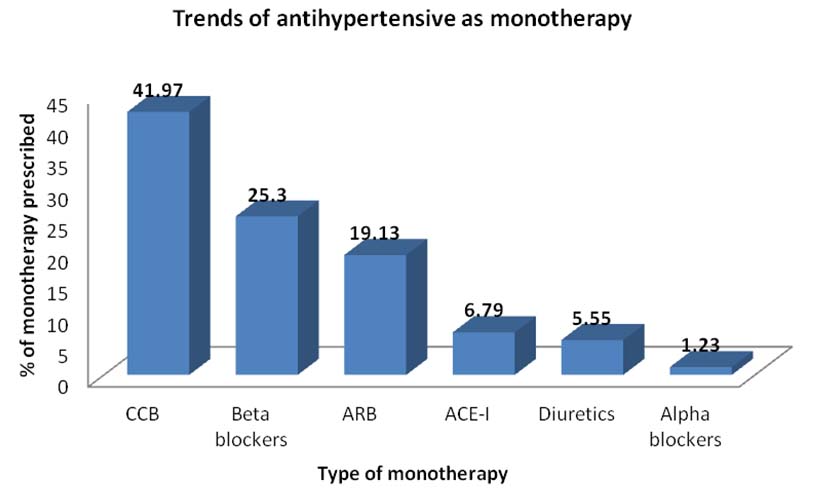
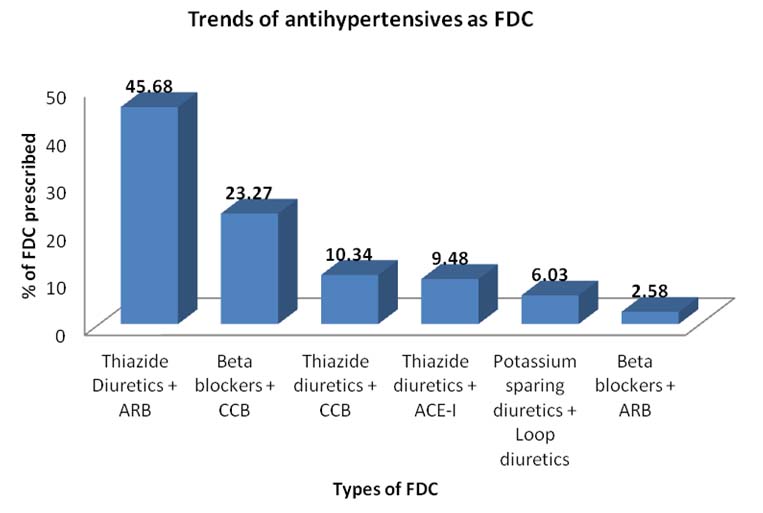
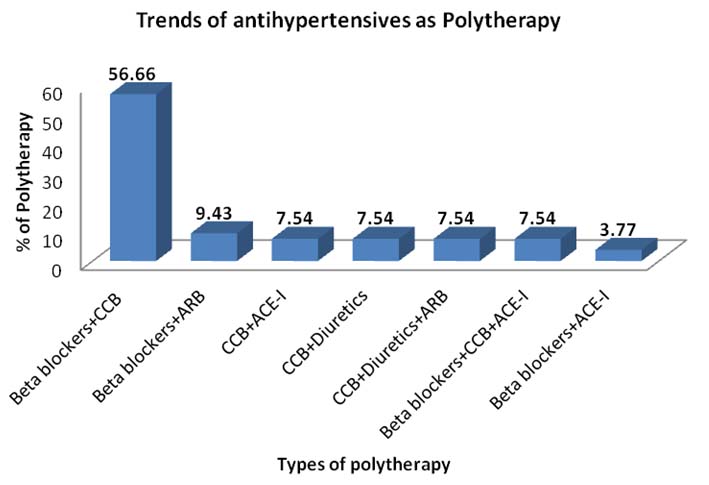
The trends of antihypertensive medication prescribed as monotherapy are shown in [Table/Fig-2]. Total of 116 prescriptions were found to have FDCs, trends of antihypertensive combination is been depicted in [Table/Fig-3]. In polytherapy [Table/Fig-4] beta blockers with CCBs were mostly prescribed (56.66%) followed by beta blockers with ARBs (9.43%).
The frequencies of the six antihypertensive drug classes prescribed by physicians are described in [Table/Fig-5]. Among the different classes of antihypertensives Amlodipine (37.3%) was the most prescribed drug followed by Atenolol (19.43%), and Telmisartan (8.03%).
Cost-effectiveness of the pharmacological agents: The ranking in terms of cost per year from the highest to the lowest found in this study was: alpha blockers> ACE-I> ARBs > CCBs > beta blockers > diuretics. Drug utilization and costs of different antihypertensive agents incurred per day as well as per year are represented in [Table/Fig-6]. Thus, the diuretics were most cost-effective (Cost per day: 5.89 ± 2.87; Cost per y: 2129.02 ± 1080.49) in relation to the other antihypertensive prescribed.
Cost-effectiveness of Different Therapy: In the comparison for antihypertensive therapy, lower costs were incurred with monotherapy followed by FDC while polytherapy proved to be the most expensive. Cost analysis of different therapy prescribed is also represented in [Table/Fig-6]. One-way ANOVA analysis on yearly expenditure on medication suggested the difference in cost of medication prescribed within a type of therapy was not significant at the p<0.05 level for all three mode of therapy {dF = (2, 297) = 0.32964; p =0.7194)}.
Discussion
Appropriate antihypertensive drug therapy is important as the prevalence of hypertension has risen dramatically in last three decades [16]. Any deviation from evidence-based guidelines in hypertension treatment contributes to the high cost of medications and creates difficulties in providing affordable prescription drugs [17].
In our study, the prevalence of hypertension was seen more in males compared to females (1.2:1), which corresponds to the findings of Gupta R et al.,[18] and Guang Hui Dong et al.,[19].
Out of six classes of drugs prescribed as monotherapy in our study, CCBs were found to be prescribed most frequently followed by beta blockers and ARBs, though diuretics are the first line of medication for the management of hypertension according to the JNC VII guideline. Diuretics were prescribed more often as FDC in our study which is comparable to studies conducted in several countries including India and USA [20,21].
JNC VII guidelines advocate initiating therapy with two drugs, either as individual doses or in fixed-dose combinations, when either the SBP is >20 mmHg or DBP is >10 mmHg above the recommended goal of <140/90 mmHg [22]. The fixed combination of beta blockers and CCBs was the second most prescribed in this study because of its efficiency and cost effectiveness [23]. Use of FDC has an advantage over polytherapy as it enhances compliance to the treatment regimen. It has also been suggested that FDC are often less expensive than multiple dosage regimen or high dose monotherapy [24].
Prescription with polytherapy reflected the major use of beta blockers and CCBs (56%) which was in line with multiple other studies conducted previously [15,25-27]. The result of cost evaluation showed that diuretics had the lowest cost per day (CPD) -INR (5.89 ± 2.87) and cost per year (CPY) -INR (2129.02 ± 1080.49) followed by other classes; these results were comparable with other studies which evaluated the cost effectiveness of the available antihypertensives [28-30]. Analysis of the comparative cost effectiveness of the therapies showed that monotherapy was least costly followed by FDC and polytherapy. This finding was supported by results of other studies which observed that patients on three or four drug regimens had significantly higher treatment costs [31].
In a developing country like India, one of the smart ways to reduce the prescription costs is to use the generics. Even though the Medical Council of India have insisted on prescribing the generic drugs as far as possible, doctors are reluctant to write prescriptions containing only generic or unbranded chemical name of drugs. All too often, the physicians and the patients prefer the expansive brand name drugs because they believe that the generic equivalent is inferior. The present study was undertaken after the implementation of drug price control order act (DPCO) 2013.According to the DPCO 2013, medication price are calculated taking simple average of all brands which have more than one percent market share [32]. Out of 652 drugs under price control, we found that only seven antihypertensives prescribed by our hospital physicians were included in the DPCO list 2013. These included atenolol, metoprolol, amlodipine, nifedipine, hydrochlorothiazide, losartan and enalapril. Previous randomized controlled trials have proven that these agents prevent recurrent myocardial infarction, stroke and decrease the overall cardiovascular mortality. Therefore by including these medications in the revised price list of DPCO 2013, they are more affordable for the patients. Medication cost are the highest proportion of the overall cost of managing hypertension. We can now hope that these price changes would improve the patient compliance and their adherence to the treatment regimen.
Our study had few limitations. Firstly, the main challenge with cross sectional study design in general. We could not assess the patients adherence to the treatment. Patients with severe co morbid illness like congestive heart disease, chronic kidney disease were not included in this study. Having these limitations, treatment pattern of anti hypertensive drugs were relatively uniform.
Characteristics of the studied patients
| Total No. of Prescriptions 300 |
| Gender | N | % |
| Male | 164 | 54.66 |
| Female | 136 | 45.33 |
| Age Mean ± SD |
| Male | 58.06±12.94 |
| Female | 62.09±14.27 |
| Total | 59.89 ± 13.68 |
| Systolic Blood Pressure (SBP) – mm Hg Mean ± SD |
| Male | 148.23±25.03 |
| Female | 146.45±23.52 |
| Total | 140 ± 16.32 |
| Diastolic Blood Pressure (DBP) - mm Hg Mean ± SD |
| Male | 86.48±18.19 |
| Female | 86.18±13.15 |
| Total | 104.4 ± 8.93 |
| Stage of Hypertension (JNC VII guidelines) | N | % |
| Normal | 26 | 8.66 |
| Prehypertension | 75 | 25 |
| Stage 1 | 109 | 36.33 |
| Stage 2 | 90 | 30 |
| Type of therapy | N | % |
| Monotherapy | 162 | 48.94 |
| Polytherapy | 53 | 16.01 |
| Fixed Dose combination | 116 | 35.04 |
N= Frequency; %= Percentage
Percentage of antihypertensive medication as monotherapy
Percentage of antihypertensive medication as FDC
Percentage of antihypertensive medication as polytherapy
Types of antihypertensive medications prescribed overall
| Type of Antihypertensive prescribed | N | % |
| Beta blockers | | 24.07 |
| Atenolol | 75 | 19.43 |
| Metoprolol | 14 | 3.62 |
| Bisoprolol | 3 | 0.77 |
| Carvedilol | 1 | 0.25 |
| CCB | | 38.59 |
| Amlodipine | 144 | 37.3 |
| Nifedipine | 5 | 1.29 |
| Diuretics | | 13.2 |
| Hydrochlorothiazide | 19 | 4.92 |
| Furosemide | 29 | 7.51 |
| Spironolactone | 3 | 0.77 |
| ARB | | 17.35 |
| Losartan | 26 | 6.73 |
| Olmesartan | 10 | 2.59 |
| Telmisartan | 31 | 8.03 |
| ACE-I | | 6.21 |
| Ramipril | 18 | 4.66 |
| Enalapril | 6 | 1.55 |
| Alpha -blockers | | 0.51 |
| Prazosin | 2 | 0.51 |
| Total | 386 | |
Drug acquisition (daily and annual) costs of the different antihypertensive drugs prescribed in the outpatient clinic.,
| Class | N | CPD (mean ± SD) | CPY (mean ± SD) |
| Diuretics | 93 | 5.89 ± 2.87 | 2129.02 ± 1080.49 |
| Beta blockers | 149 | 6.01 ± 2.80 | 2184.23 ± 1069.49 |
| CCB | 51 | 9.02 ± 4.27 | 3293.32 ± 1603.22 |
| ARB | 67 | 10.23 ± 4.21 | 3748.54 ± 1552.29 |
| ACE-I | 24 | 9.33 ± 5.62 | 3780.41 ± 2501.14 |
| α blockers | 2 | 13.08 ± 3.23 | 4776.05 ± 1179.48 |
| Type of therapy | N | CPD (mean ± SD) | CPY (mean ± SD) |
| Monotherapy | 162 | 6.30± 3.71 | 2362.69 ± 1521.67 |
| Polytherapy | 53 | 6.87 ± 2.37 | 2525.72 ± 853.33 |
| FDC | 116 | 7.16 ± 3.70 | 2576.48± 1399.47 |
CPD= Cost per Day; CPY= Cost Per Year. (df=2; p=0.7194) (Both CPD and CPY in Indian Rupees),
Conclusion
Our retrospective cross-sectional study analysed the prescription pattern of antihypertensive drugs and found that the prescribing pattern was not totally consistent with the JNC VII guidelines for the treatment of hypertension. Monotherapy was consistently more recommended in the early stages of hypertension to achieve target goal of blood pressure and calcium channel blockers were the drugs of choice for hypertensive patients as a single drug therapy and overall utilization.
The cost analysis showed monotherapy to be more economical .The under utilization of diuretics in monotherapy is the most important drawback of the present prescribing pattern as they are available at lower cost. But in combination therapy diuretics are being utilized in combination with angiotensin receptor blocker (45.68 %) and the pattern supports JNC VII guidelines. Higher percentage of patients (56.66%) was found to be on polytherapy. The DPCO 2013 has overcome the problem of fixation of prices of drugs.
N= Frequency; %= Percentage
CPD= Cost per Day; CPY= Cost Per Year. (df=2; p=0.7194) (Both CPD and CPY in Indian Rupees),
[1]. PM Kearney, M Whelton, K Reynolds, P Muntner, PK Whelton, J He, Global burden of hypertension: analysis of worldwide data.Lancet 2005 365:217-23. [Google Scholar]
[2]. RB Singh, IL Suh, VP Singh, S Chaithiraphan, P Laothavorn, SY RG, Hypertension and stroke in Asia: Prevalence, control and strategies in developing countries for prevention.J Hum Hypertens. 2000 14:749-63. [Google Scholar]
[3]. PR Kokiwar, SS Gupta, PM Durge, Prevalence of hypertension in a rural community of central India.J Assoc Physicians India. 2012 60:26-29. [Google Scholar]
[4]. SS Lim, T Vos, AD Flaxman, G Danaei, K Shibuya, H Adair- Rohani, A comparative risk assessment of burden of disease and injury attributable to 67 risk factors and risk factor clusters in 21 regions, 1990-2010: a systematic analysis for the Global Burden of Disease Study 2010.Lancet. 2013 380:2224-60. [Google Scholar]
[5]. V Patel, S Chatterji, D Chisholm, S Ebrahim, G Gopalakrishna, C Mathers, Chronic diseases and injuries in India.Lancet 2011 377:413-28. [Google Scholar]
[6]. T Sandozi, VK Emani, Survey of prescription pattern of anti-hypertensivedrugs in hypertensives & hypertension associated diabetics.International Journal of Pharma and Bio Sciences. 2010 1(4):P23-26. [Google Scholar]
[7]. PM Kearney, M Whelton, K Reynolds, P Muntner, PK Whelton, J He, Global burden hypertension: analysis of worldwide data.Lancet 2005 365:217-23. [Google Scholar]
[8]. R Gupta, VP Gupta, Hypertension epidemiology in India: lessons from Jaipur Heart Watch.Current science. 2009 97(3):349-55. [Google Scholar]
[9]. Q Gu, R Paulose-Ram, C Dillon, V Burt, Antihypertensive medication use among US adults with hypertension. Circulation 2006 113:213-21. [Google Scholar]
[10]. European Society of Hypertension-European Society of Cardiology guidelines for the management of arterial hypertension.J Hypertens. 2003 21(6):1011-53. [Google Scholar]
[11]. AV Chobanian, GL Bakris, HR Black, WC Cushman, LA Green, JL Izzo, Seventh report of the Joint National Committee on Prevention, Detection, Evaluation, and Treatment of High Blood Pressure.Hypertension 2003 42:1206-52. [Google Scholar]
[12]. PH Liu, JD Wang, Antihypertensive medication prescription patterns and time trends for newly diagnosed uncomplicated hypertension patients in Taiwan.BMC Health Serv Res. 2008 8:133 [Google Scholar]
[13]. JD Guo, GG Liu, DB Christensen, AZ Fu, How well have practices followed guidelines in prescribing antihypertensive drugs: the role of health insurance. Value Health. 2003 6(1):18-28. [Google Scholar]
[14]. Current Index of Medical Specialities(update-1).CMPM Medical India Private Limited. September-DecemberLancet. 2013 [Google Scholar]
[15]. R Jhaj, NK Goel, CS Gautam, Prescribing Patterns and Cost of Antihypertensive Drugs in an Internal Medicine Clinic.Indian.Heart J. 2001 53:323-27. [Google Scholar]
[16]. R Gupta, Trends in hypertension epidemiology in India.J Hum Hypertens. 2004 18:73-78. [Google Scholar]
[17]. MA Fischer, J Avorn, Economic implications of evidence-based prescribing for hypertension: can better care cost less?JAMA 2004 291:1850-56. [Google Scholar]
[18]. R Gupta, H Prakash, VP Gupta, KD Gupta, Prevalence and determinants of coronary heart disease in a rural population of India. J Clin Epidemiol. 1997 50:203-09. [Google Scholar]
[19]. GH Dong, ZQ Sun, XZ Zhang, JJ Li, LQ Zheng, J Li, Prevalence, awareness,treatment and control of hypertension in a rural Liaoning Province, China. Indian J Med Res. 2008 128:122-27. [Google Scholar]
[20]. Q Gu, R Paulose-Ram, C Dillon, V Burt, ntihypertensive medication use among US adults with hypertension.Circulation. 2006 113(2):213-21. [Google Scholar]
[21]. AV Chobanian, GL Bakris, HR Black, Seventh report of the Joint National Committee on Prevention, Detection, Evaluation, and Treatment of High Blood Pressure.Hypertension 2003 42:1206-52. [Google Scholar]
[22]. HR Black, WJ Elliott, G Grandits, Principal results of the Controlled Onset Verapamil Investigation of Cardiovascular End Points (CONVINCE) trial. J Am Med Assoc. 2003 289:2073-82. [Google Scholar]
[23]. A Carre, Pharmacologic importance of the combination atenolol/nifedipine in hypertensive patients.Drugs. 1998 56(2):23-30. [Google Scholar]
[24]. JJ Caro, JL Speckman, M Salas, Effect of initial drug choice on persistence with antihypertensive therapy: the importance of actual practice data.Can Med Assoc J. 1999 160:41-46. [Google Scholar]
[25]. PK Lee, RK Li, JC Chan, S Chang, SC Lee, B Tomlinson, A prescription survey in a hospital hypertension outpatient clinic.Br J Clin Pharmacol. 1997 44:577-82. [Google Scholar]
[26]. S Malhotra, RS Karan, P Pandhi, S Jain, Pattern of use and pharmacoeconomic impact of antihypertensive drugs in a north Indian referral hospital.Eur J Clin Pharmacol. 2001 57:535-40. [Google Scholar]
[27]. F Khurshid, M Aqil, MS Alam, P Kapur, KK Pillai, Antihypertensive medication prescribing patterns in a university teaching hospital in south Delhi.IJPSR 2012 3(7):2057-63. [Google Scholar]
[28]. R Dias da Costa, R Fuchs, R Olinto, R Gigante, VP Menezes, Cost effectiveness of hypertension treatment: a population-based study. Sao Paulo Med J. 2002 120:100-04. [Google Scholar]
[29]. GC Moreira, JP Cipullo, JF Martin, LA Ciorlia, MR Godoy, CB Cesarino, Evaluation of the awareness, control and cost-effectiveness of hypertension treatment in a Brazilian city: populational study.J Hypertens. 2009 27(9):1900-07. [Google Scholar]
[30]. Q Alefan, MIM Ibrahim, TA Razak, A Ayub, Cost-effectiveness of antihypertensive treatment in Malaysia.Malaysian Journal of Pharmaceutical Sciences. 2009 7(2):137-52. [Google Scholar]
[31]. OS Ilesanmi, OK Ige, AO Adebiyi, The managed hypertensive: the costs of blood pressure control in a Nigerian town.Pan Afr Med J. 2012 12:96 [Google Scholar]
[32]. V Kumar, NV Gupta, KA Kumar, A comparison between old and latest systems in DPCO.International Journal of Pharmacy and Pharmaceutical Sciences 2014 6(2):19-20. [Google Scholar]