Seroprevalence of Toxoplasma IgG Antibodies in HIV Positive Patients in and Around Khammam, Telangana State
Basavaraju Anuradha1, Chilupuri Preethi2
1 Professor & HOD, Department of Microbiology, Mamata Medical College, Khammam, Telangana, Andhra Pradesh, India.
2 Post Graduate Student, Department of Microbiology, Mamata Medical College, Khammam, Telangana, Andhra Pradesh, India.
NAME, ADDRESS, E-MAIL ID OF THE CORRESPONDING AUTHOR: Dr. Basavaraju Anuradha, H. No. 11- 4-74,Nehru Nagar, Khammam - 507002, Andhra Pradesh, India. Phone : 9848097479, E-mail : Basavaraju_a@yahoo.com
Dear Sir,
Toxoplasma gondii, one of the most common parasites of humans infecting approximately one third of world’s population. With the advent of HIV pandemic, toxoplasmosis has been reported as the commonest opportunistic infection in HIV/AIDS patients in developed countries [1,2] and most common cause of focal brain lesions, coma and death. Transmission is mainly by ingestion of tissue cysts in raw and undercooked meat, exposure of oocysts in contaminated vegetables or contact with faeces of pets. The incidence of Toxoplasma gondii in patients depends mainly on the existence of latent anti-toxoplasma antibodies in affected population [3,4]. Because of the risk of damage to Central Nervous System and high morbidity in the patients, it is important to find out the prevalence of anti-toxoplasma antibodies in HIV/AIDS patients. Serological evidence of infection virtually always precedes the development of Toxoplasma disease. It is estimated by presence of IgG antibodies.
A cross-sectional study was conducted from August 2013 to October 2013 on 92 HIV positive patients attending ICTC centre, Khammam with the approval of institutional ethics committee. Samples were collected after written informed consent. Patients of all age groups and both sexes, with CD4 counts less than 500, were included.
IgG antibodies were estimated by using Serion ELISA classic Toxoplasma gondii IgG kit supplied by Lilac medical care Ltd, Germany. Sensitivity and specificity of the test are 98.2% and 99.4% respectively.
The results are interpreted as per manufacturer’s instructions. Out of 92 HIV positive patients 32 were positive for anti-toxoplasma antibodies. Toxoplasma IgG antibodies were present in 11 males out of 38 and 21 females out of 54. The sex distribution can be seen in the [Table/Fig-1].
Sex wise distribution of toxoplasma antibodies
| Gender | positive | negative | Total | Percentage |
|---|
| Male | 11 | 27 | 38 | 28.95% |
| Female | 21 | 33 | 54 | 38.89% |
| Total | 32 | 60 | 92 | |
Age range of the patients was between 20-50 years with mean age of 33.75 for anti-toxoplasma IgG antibodies positivity. The age wise distribution of IgG antibodies is given in the [Table/Fig-2].
Age wise distribution of toxoplasma antibodies
| Gender | positive | negative | Total | Percentage |
|---|
| <20 | 0 | 3 | 3 | 0 |
| 21-30 | 7 | 24 | 31 | 22.58% |
| 31-40 | 20 | 21 | 41 | 48.78% |
| 41-50 | 4 | 10 | 14 | 28.57% |
| >50 | 1 | 2 | 3 | 33.33% |
| Total | 32 | 60 | 92 | |
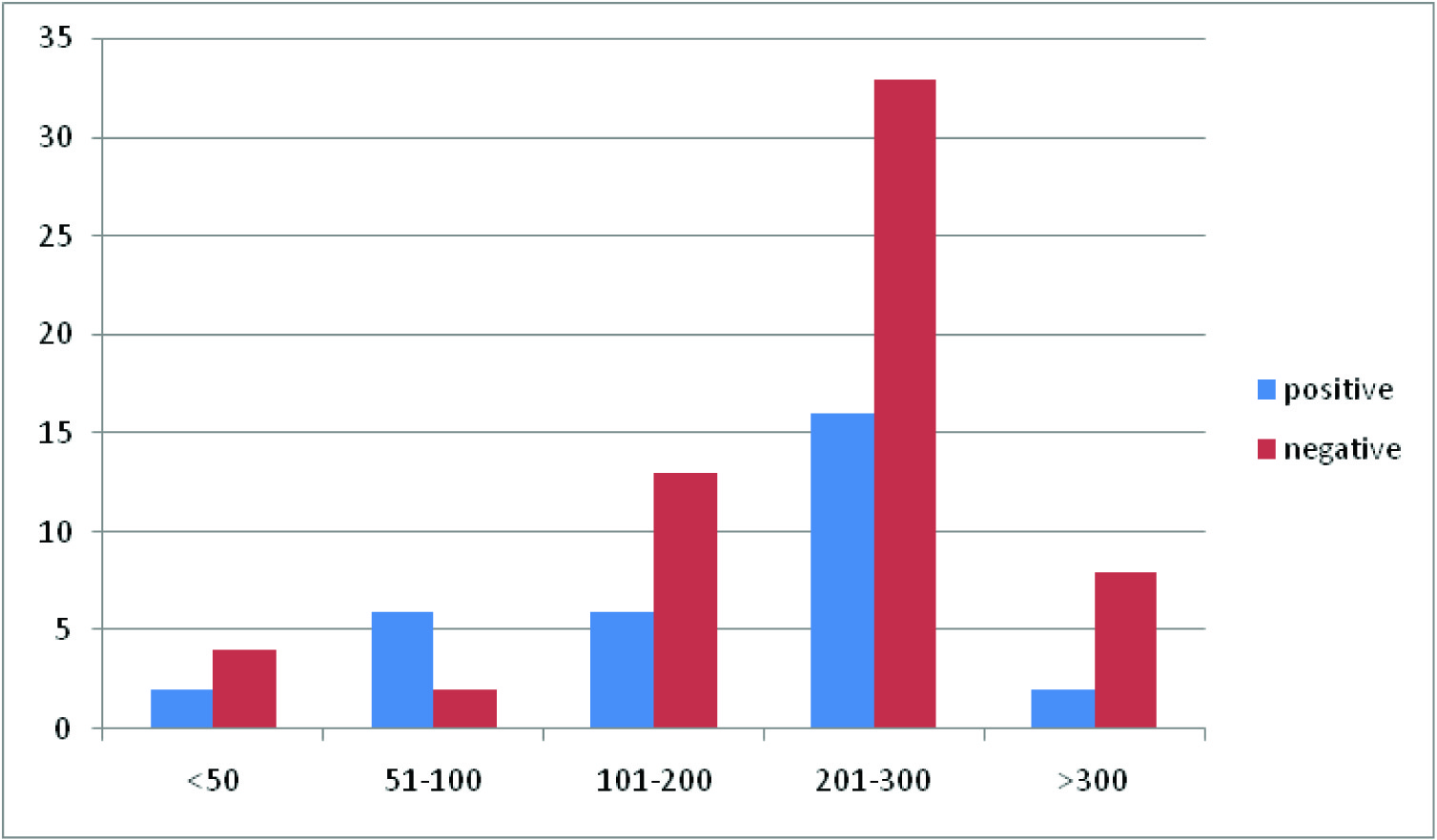
CD4 counts ranging up to 500 with mean CD4 count of 200.96 cells/mm3. CD4 counts were categorised into 5 groups. CD4 count <50 cells/mm3 , 51-100 cells/mm3, 101-200 cells/mm3 , 201-300 cells/mm3 and >300 cells/mm3 . The seroprevalence of Toxoplasma IgG antibodies in relation to CD4 counts is given in the [Table/Fig-3].
Toxo IgG antibodies in relation to CD4 Counts
Our study reveals that seroprevalence of Toxoplasmosis is 34.78% among HIV patients. The prevalence of Toxoplasmosis in different geographic areas is variable 75.4% in Nigeria [5], 60% from AIDS patients in Cote d’Ivoire [6], 58.4% in Tunisia [7], 28.5% in HIV woman in Benin [8], 53.6% in Guania, 40.2% in Senegal [9], 34.1% from pregnant woman in Sudan [10]. In one study by Sucilathangam G et al., showed seropositivity of toxoplasmosis in HIV positive patients was found to be 15 % based on IgG ELISA and it was found to be highly sensitive (90%) and specific (100%) in detecting toxoplasmosis [11]. The variation in prevalence rates could be due to difference within the geographical locations, infection is more common in warm climates and at lower altitudes than in cold and mountainous regions [12].
The seroprevalence was 48.78% in age group of 31-40 years. This is correlating with reports by Meisheri et al., which showed that highest prevalence at 3rd and 4th decade of life [13]. However, Nisspatorn et al., reported highest prevalence rate within 2nd and 3rd decade of life [12]. The increase in prevalence rate with increase in age may be explained by increase risk of exposure with infection with increase in age.
Seroprevalence of Toxoplasmosis in our study was more in females (38.89%) than in males (28.95%) indicating that females are at higher risk of infection. This could be due to various reasons such as more association with pet animals, handling of raw meat more frequently than men. In one study by Liu Q et al., from China found that taking care of pet animals and consuming raw meat are two main risk factors in relation to Toxoplasma gondii infection [14].
There was an association between CD4 counts and prevalence of Toxoplasmosis. In patients with CD4 counts between 51-100 cells/mm3 without any neurological symptoms toxoplama IgG antibodies are present in 75% cases. Vincent O et al., reported that 79.4% of HIV positive people without neurological symptoms had CD4 counts <100 cells/mm3 [15]. But, in one study by Eliaszewiez et al., in France showed that 79% of patients with neurological symptoms had CD4 counts <150 cells/mm3 [16]. These findings are contrary to findings in our study which may further confirm the early onset of neurological complications among HIV patients may be unrelated to Toxoplasma infection.
Toxoplasma gondii prevalence is more common in 3rd and 4th decade of life. Immunosupressed people with CD4 counts <100 cells/mm3 are more commonly affected. Serological testing has become the routine method of diagnosis of Toxoplasmosis especially in resource poor countries where it is the most available and affordable means for detecting the presence of antitoxoplasma antibodies. Hence, It is advisable to screen for Toxoplasma IgG antibodies in all HIV positive people to detect the latent infection as this may reduce the risk of Toxoplasma encephalitis.
[1]. Winstanley P, Drug treatment of toxoplasmic encephalitis in acquired immunodeficiency syndromePost Grad Med Jr 1995 71:404-08. [Google Scholar]
[2]. Mccabe R, Chirirgi V, Issues in ToxoplasmosisInfect Dis Clin North Am 1993 7(3):587-604. [Google Scholar]
[3]. Grant IH, Gold JW, Rosenblum M, Niedzwiecki D, Armstrong D, Toxoplasma gondii serology in HIV-infected patients: the development of centralnervous system toxoplasmosis in AIDSAIDS 1990 4:519-521. [Google Scholar]
[4]. Holliman RE, Serological study of the prevalence oftoxoplasmosis in asymptomatic patients infected withhuman immunodeficiency virusEpidemiol Infect 1990 105:415-18. [Google Scholar]
[5]. Onadeko MO, Joynson DH, Payne RA, Francis J, The prevalence of Toxoplasma antibodies in pregnant Nigerian women and the occurrence of stillbirth and congenital malformationAfr. J. Med. Sci 1996 25:331-34. [Google Scholar]
[6]. Adou-Bryn KD, Ouhon J, Nemer J, Yapo CG, Assoumou A, Serological survey of acquired toxoplasmosis in women of childbearing age in Yopougon (Abidjan, Cote d’Ivoire)Bull. Soc. Pathol. Exot 2004 97:345-48. [Google Scholar]
[7]. Bouratbine A, Siala E, Chahed MK, Aoun K, Ben Ismail R, Seroepidemiologic profile of toxoplasmosis in Northern TunisiaParasite Immunol 2001 8:61-66. [Google Scholar]
[8]. Rodier MH, Berthonneau J, Bourgoin A, Giraudeau G, Agius G, Burucoa C, Kekpazo A, Jacquemin J. L, Seroprevalences of toxoplasma, malaria, rubella, cytomegalovirus, HIV and treponemal infections among pregnant women in Cotonou. RepubBenin. Acta Trop 1995 59:271-77. [Google Scholar]
[9]. Assob Jules C.N, Njunda Anna L, Nsagha Dickson S, Kamga Henri L, Weledji Patrick E, Che V. B, Toxoplasma antibodies amongst HIV/AIDS patients attending the university teaching hospital Yaounde, in CameroonAFR. J. CLN. EXPER. MICROBIOL 2011 12(3):1119-123. [Google Scholar]
[10]. Faye O, Leye A, Dieng Y, Richard-Lenoble D, Diallo S, Toxoplasmosis in Dakar. Seroepidemiologic sampling of 353 women of reproductive age. Bull. Soc. Pathol. Exot. 1998; 91:249–250 11. Elnahas A., Gerais A. S, Elbashir M.I, Eldien E. S., Adam I. Toxoplasmosis in pregnant Sudanese womenSaudi. Med. J 2003 24:868-70. [Google Scholar]
[11]. Sucilathangam G, Palaniappan N,*, Sreekumar C,**, Anna T, Serological survey of toxoplasmosis in a district in Tamil Nadu: Hospital-based studyIndian J Med Res 2013 137(3):560-63. [Google Scholar]
[12]. Nissapatorn V, Lee CKC, Cho SM, Toxoplasmosis in HIV/AIDS patients in MalaysiaSoutheast Asian J Trop Med Public Health 2003 34(2):80-85. [Google Scholar]
[13]. Meisheri YV, Mehta S, Patel U, A prospective study of seroprevalence of Toxoplasmosis in general population, and in HIV/AIDS patients in Bombay, IndiaJ Postgrad Med 1997 43:93-97. [Google Scholar]
[14]. Liu Q, Wei F, Gao S, Jiang L, Lian H, Yuan B, Toxoplasma gondii infection in pregnant women in ChinaTrans R Soc Trop Med Hyg 2009 103:162-66. [Google Scholar]
[15]. Osunkalu Vincent O, Akanmu SA, Ofomah NJ, Onyiaorah IV, Adediran AA, Akinde RO, Seroprevalence of Toxoplasma gondii IgG antibody in HIV-infected patients at the Lagos University Teaching HospitalHIV/AIDS - Research and Palliative Care 2011 3:101-05. [Google Scholar]
[16]. Eliaszewicz M, Lecomte I, De Sa M, Relation between decreasing series CD4 lymphocyte count and outcome of toxoplasmosis in AIDS patients: a basis for primary prophylaxisInt Conf AIDS 1990 6(242):20-23. [Google Scholar]