One of the most distressing and dramatic causes of xerostomia is radiotherapy for the cure of maxillofacial and neck carcinomas. Patient with radiotherapy induced xerostomia presents with challenges in prosthodontic management and in unique radiation caries control. This clinical report illustrates step by step execution of complex treatment planning that lead to successful outcome in 34-year-old man, who had been treated with Radical Neck Dissection (RND) and therapeutic radiotherapy for squamous cell carcinoma of tongue and due to radiation caries, was presented with chief complaint of difficulty in mastication. Rehabilitation was carried out with metal-ceramic fixed restorations and cast removable prostheses after extensive endodontic intervention. This article also discusses the maintenance strategies for radiation caries patient requiring complete occlusal reconstruction, who certainly presents with special needs in post-treatment management.
Complete occlusal rehabilitation, Radiation caries, Squamous cell carcinoma of tongue, Treatment sequencing
Case Report
A 34-year-old man reported with the chief complaint of difficulty in mastication. The integrated approach towards complete occlusal reconstruction consists of four phases: (1) patient evaluation (2) comprehensive treatment planning (3) systemic reconstruction and (4) postoperative maintenance [1].
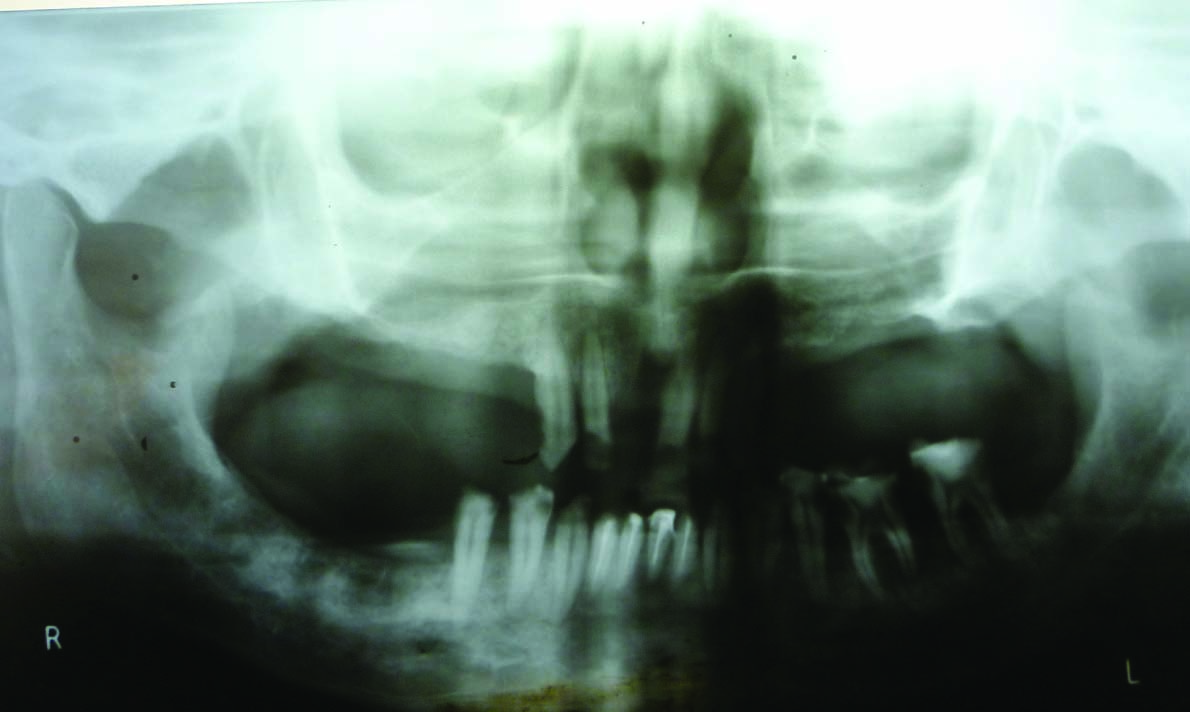
1. Patient evaluation: The first phase can be subdivided into history taking and clinical examination. A 27-year-old male patient was referred by local physician to Head & Neck, Plastic and Reconstructive surgery Department, TATA Memorial Hospital, Mumbai, India for his chief complaint of ulcer on tongue for three months and swelling in neck for two months. On examination then, 3×3 cm lesion on right lateral border of tongue and ankyloglossia were observed. Patient was diagnosed histo-pathologically as squamous cell carcinoma and treated with hemiglossectomy of right side of tongue and RND eight years from now [Table/Fig-1a]. Post-operative radio therapy with 60Co to a total dose of 5600 centigray (cGy) was also included in the treatment regimen. It was started two months after surgery and lasted for 43 d. Oral prophylaxis and extractions of left first to third maxillary molars were carried out before radiotherapy in the dental department of the same hospital. No radiation shield or stent was used while radiation therapy being given. On clinical examination for dental rehabilitation, it was observed that patient had surgical scar on the right side of the neck with facial asymmetry [Table/Fig-1b]. Exodontias were advised after intra oral examination revealed un-restorable maxillary right central incisor, maxillary left premolars, maxillary right posteriors as well as mandibular right molars. Thus, what remained was maxillary anteriors with missing right central incisor and class II mandibular arch with remaining decayed dentition from left second molar to contralateral second premolar. The saliva was mucus and of very less quantity. The patient was diagnosed as radiation caries with severe xerostomia and loss of vertical dimension (VD) of occlusion [Table/Fig-2a,b]. Diagnostic impressions were taken for two sets of diagnostic casts. One set of casts was maintained as a pretreatment record. Centric and protrusive jaw relationship records were obtained with record bases and occlusal rims to mount the diagnostic casts on semi-adjustable articulator (Hanau Wide vue, Whipmix Corporation, Louisville, KY) using face-bow (spring bow, WhipMix Corporation, Louisville, KY). Loss of VD was determined around 5mm by viewing the profile of the patient in maximum inter-cuspation and evaluation of the freeway space at the physiologic rest position. The assessment of the position of the maxillary central incisor relative to the upper lip was made with the patient’s upper lip at rest. The ideal gingival levels were determined by establishing the correct width-to-length ratio of the maxillary anterior teeth, by determining the desired amount of gingival display and by establishing symmetry between right and left sides of the maxillary dental arch [2]. Incisal pin on the articulator was raised to utilize the available space in diagnostic wax-up.

Preoperative front view note the facial asymmetry

Preoperative Intra-oral front view,

Pre-operative panoramic radiograph
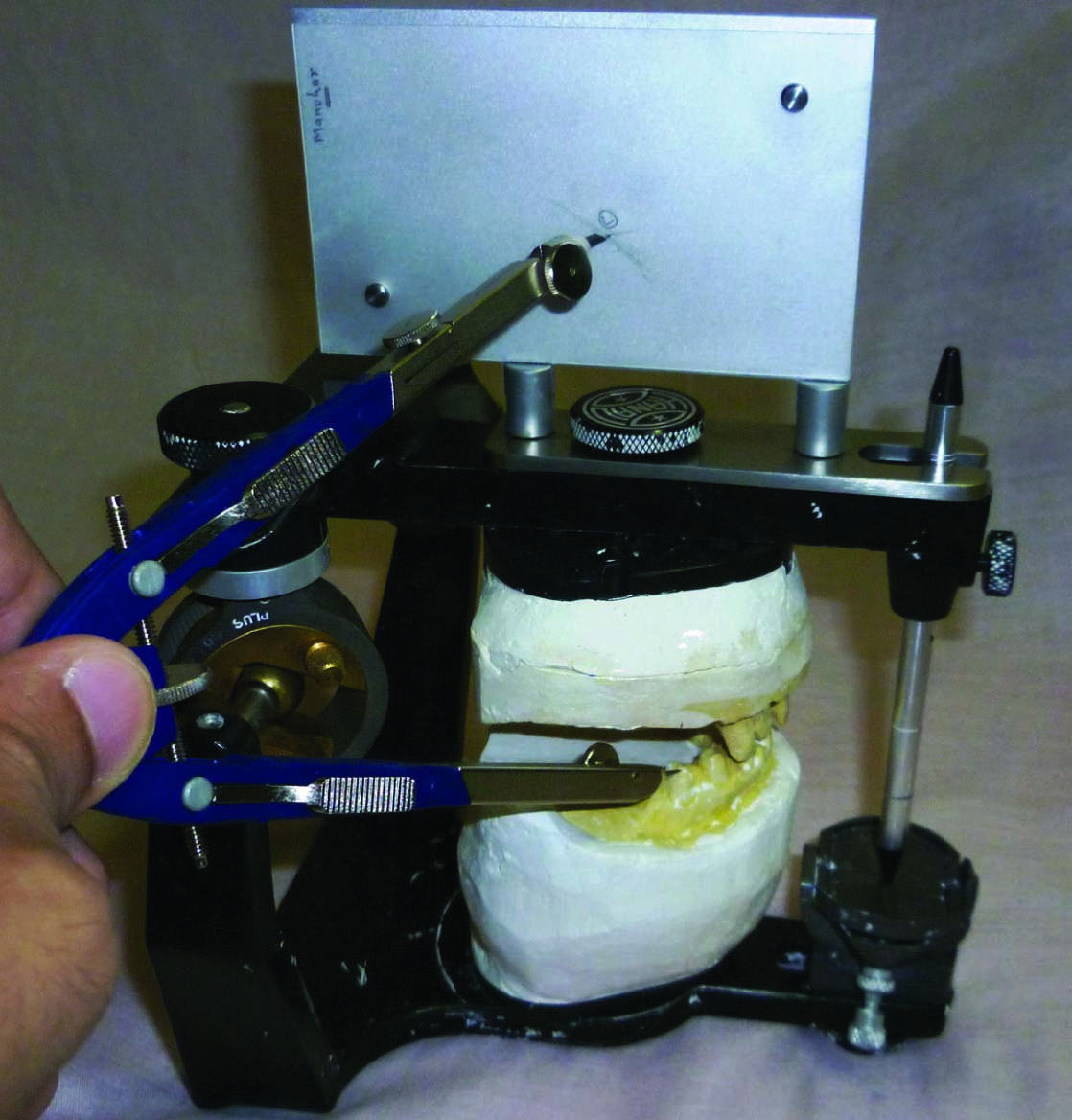
2. Comprehensive Treatment Planning: All the assessments and evaluations of maxillary incisors and gingival levels facilitated in correct positioning of the incisal edges and cervical portion of the maxillary anteriors during diagnostic wax-up. Mandibular anterior teeth were first modified to have ideal morphology. Maxillary anterior teeth were then altered to optimum aesthetics. Posterior occlusal plane was determined with broad rick occlusal plane analyser [Table/Fig-3] and modified in accordance with anterior guidance to have balanced occlusion in excursions [1]. Acrylic preformed denture teeth were arranged in maxillary and mandibular posterior edentulous areas. Various prosthetic treatment options were explained to the patient in the second visit. Due to economic constraints, complete mouth rehabilitation with fixed metal-ceramic restorations and tooth and tissue supported cast removable prostheses was suggested.
Broadrick occlusal plane analyser
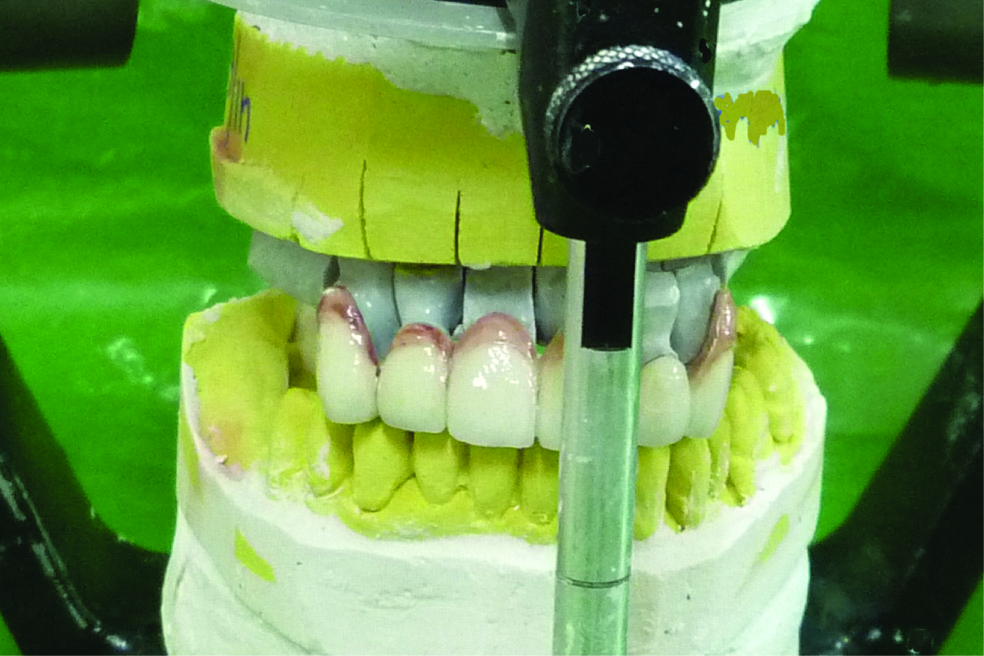
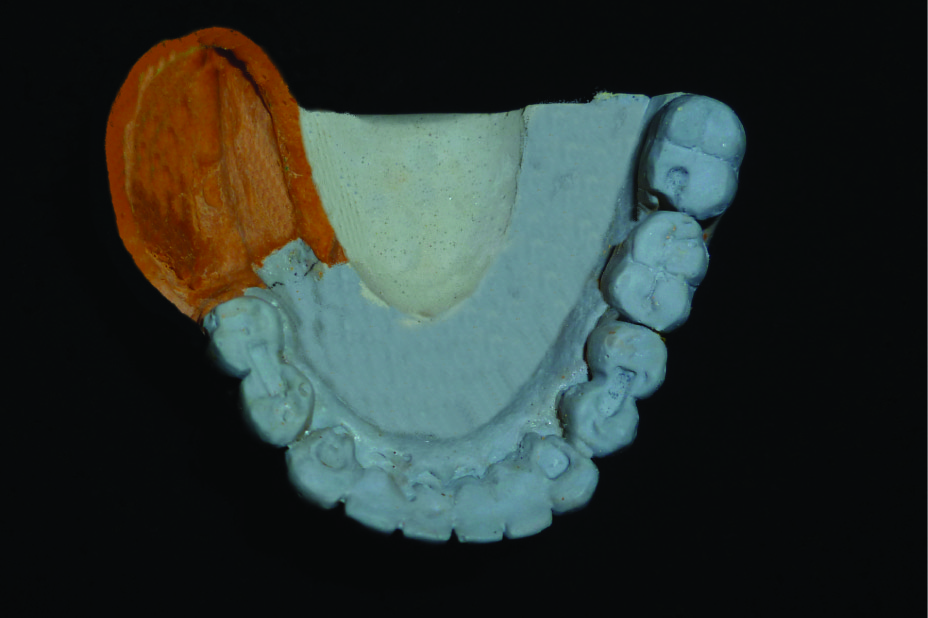
3. Systemic Reconstruction: Reconstruction phase can be subdivided into four phases: (1) mouth preparation prior to definitive tooth preparation (2) tooth preparation and fabrication of provisional restorations (3) final restorations fabrication and provisional cementation; and (4) final cementation. Endodontic treatment was carried out for all the remaining dentition. Cast posts and cores were done for mandibular anteriors. Pre-fabricated post and core was done for maxillary right lateral incisor [Table/Fig-4a,b]. Vacuum formed tooth preparation guides were fabricated from the casts obtained from diagnostic wax-up. Maxillary and mandibular arch tooth preparations were completed on successive days [Table/Fig-5a,b] and checked for adequacy with tooth preparation guides. Silicon putty moulds were used to fabricate acrylic provisional restorations to reproduce the occlusal scheme which was developed during diagnostic wax-up stage. Acrylic provisional restorations were cemented with eugenol free temporary cement. Provisional restorations also involved removable partial denture. Patient was allowed to wear provisional restorations for eight weeks to confirm the aesthetics, function and comfort of the newly developed occlusal scheme. Maxillary and mandibular final impressions were made with addition silicon material (Express XT, 3M ESPE, St Paul, MN). Anterior provisional restorations were removed and Lucia jig was constructed at the VD of occlusion established during diagnostic wax up. Another record was obtained with record bases and rims and only anterior provisional restorations in place. An index made on the cast of the corrected and approved provisional restorations of the mandibular anterior was used to communicate exact details to the technician [3]. The anterior guidance as determined and tested was duplicated by use of the customized anterior guide table. The metal copings for the crowns and fixed partial denture (FPD) with occlusal rests on predetermined areas for cast partial denture (CPD) were completed and fit for the same was verified intraorally. Metal ceramic restorations were completed [Table/Fig-6] and cemented with temporary cement. Once the final restorations were found satisfactory in objectives such as aesthetics, function, ease of oral hygiene, definitive cementation was carried out [Table/Fig-7]. Maxillary and mandibular arch impressions were taken to construct CPD framework. On subsequent appointment, when framework was ready, altered cast technique was followed to compensate tissue compressibility [Table/Fig-8a,b]. Teeth arrangement was completed on semi-adjustable articulator and checked for bilaterally balanced occlusion. After wax try-in [Table/Fig-9a,b], partial dentures were processed and delivered.
Cast posts direct pattern fabrication

Prefabricated post and core with 12 and cemented cast posts and cores in mandibular anteriors

Mandibular arch tooth preparations

Maxillary arch preparations

Maxillary finished FDP with mandibular definitive prostheses cast on Hanau wide-vue
Cemented maxillary and mandibular FDPs




4. Postoperative maintenance: Following the treatment [Table/Fig-10a,b], patient was instructed to maintain good oral hygiene – brush twice daily with soft toothbrush and use dental floss regularly. Patient was prescribed oral rinse with chlorhexidine 1.2% mouth rinse (Hexidine, Ipca, Mumbai, MS) twice daily. Sodium fluoride 1.1% (Previ Dent 1.1% Brush-On Gel; Colgate Oral Pharmaceuticals, New York, NY) was prescribed to use with brushing at bed time preferably to allow prolonged exposure of fluoride to teeth [4]. Patient was informed for the use of Vaseline on lips to prevent irritation and to spray salivary substitute (optimoist; Colgate Oral Pharmaceuticals, New York, NY) 4-5 times a day. Patient visited once or twice with sore spots complaint after CPD delivery. Occlusion refinement and relief of the tissue surface of the prosthesis by using pressure indicating paste resolved the problem. Patient was informed for the every 6 months recall schedule. On recall visits, patient was satisfied with the improved aesthetics and function with the prostheses. Patient was found to be following oral hygiene instructions optimally.
Postoperative Intra-oral front view


Discussion
Carcinoma, surgery and subsequent radiotherapy have profound effects on quality of life of the patient. Dentist has a significant role to play – from the early detection of the precancerous changes to complete oral rehabilitation following completion of the cancer therapy. The patient who receives radiotherapy usually need complete occlusal reconstruction due to different degrees of partial edentulism and radiation caries involving the remaining dentition.
This article illustrates a step by step approach to the complete occlusal rehabilitation of a partially edentulous patient with a history of radical neck dissection (RND) and radiotherapy.
The common treatment of neoplasm in and about the oral cavity is by X-ray radiation. The inadvertent radiation of adjacent structures results in variable forms of damage, depending on the radio sensitivity of different types of living cells. Carcinoma of the tongue (COT) comprises between 25 and 50 per cent of all intraoral cancers [5]. A definite aetiology does not appear to exist as per our present state of knowledge. The typical lesion developed in this case was on the lateral border of the posterior tongue.
Judicious combination of surgery and X-ray has become the treatment protocol for the patient with COT. Many radiotherapists prefer the use of radium needles and radon seeds to X-ray radiation because with these devices limit the radiation to the tumour, sparing adjacent normal tissue.
Xerostomia is one of the earliest and most universal of complaints of patients receiving therapeutic radiation about the head and neck. Post-radiation glandular atrophy is partly due to a reduction in the vascularity of the gland and partly to the direct effect of the X-rays on the highly specialized and sensitive secretary epithelial cells [6]. The serous glands are more radiosensitive than mucous glands.
Erupted teeth are often affected by destruction of tooth substance, resembling dental caries and sometimes called ‘radiation caries’, which often begins at the cervical area of the teeth. Besides the lack of lubrication associated with the decreased salivary flow, other complications include a significant decrease of the bactericidal action and self-cleansing properties of saliva are the primary causes of the condition.
The most significant factor affecting prognosis of these patients is the presence or absence of cervical metastases. The necessity for early diagnosis thus becomes obvious, and the role of the dentist in identifying cancerous changes is, certainly, of paramount importance. Dentist can play a significant role both before and after radiotherapy. After radiation therapy, dental practitioners should strive to rule out infections in the oral cavity due to the compromised host defence mechanism [7]. Different prosthetic treatment options should be made available to the patient.
The median time interval reported in the literature between extraction and irradiation is 15 to 30 d [8]. In patients, as is this, in whom ipsilateral radiation is indicated, acrylic resin stents are fabricated with or without shielding alloy. Stents with shielding alloy such as lead are used while treating well lateralized tumours of the oral cavity, lip, parotid gland and cheek [9]. Treatment option executed to rehabilitate this patient is considered inferior in comparison to implant supported prostheses in xerostomic patient, removable partial denture may cause minor soft tissue irritation. To keep the fixed partial denture abutments caries free, meticulous oral hygiene and regular use of topical fluoride is essential. Despite that, caries remains to be the significant risk for dentition. Sufficient number of implants to provide support, retention and stability for fixed prostheses can be used to avoid intimate soft tissue contact as in removable partial denture. certainly, implants do not degrade by cariogenic bacteria [10]. A recent review [11] discussed five variables that should be considered for implant placement in irradiated bone: site of implant placement, time interval between radiation and implant placement, effect of hyperbaric oxygen therapy (HBO) on implant survival, radiation dose and timing of radiation therapy (before or after radiation therapy). Implant survival for pre and post-implantation radiation were 89% and 92% respectively. Implant survival in maxilla and mandible were 79% and 93% respectively. The study fails to identify cut-off time interval for implant placement after radiation therapy and any trend for increased implant survival rate with increased time interval. Radiation dose above 5500 cGy significantly reduced the implant survival. Though no significant difference in implant survival with or without HBO, it may be used as an adjunct prior to implant placement whenever possible. Alikhashi et al.,[4] recently reported full mouth rehabilitation in radiation caries patient due to naso-pharyngeal carcinoma. The author used similar approach except that endosseous implants were used to restore posterior mandible. Systemic step by step approach to occlusal rehabilitation can be grouped into several distinct phases for successful outcome. It was initially planned to use permanent soft liners as tissue surface of the CPDs. On recall visits, patient was found to be tolerating acrylic tissue surface without discomfort. Post-treatment management advised to patient is optimal and it must be followed extremely diligently to ensure success with this treatment option [10]. Oral hygiene instructions and daily fluoride application are very important in this compromised patient.
Conclusion
To plan in advance according to patient’s perceived dental needs for predictable treatment outcome with diagnostic wax-up and to execute that blue print in systemic manner resulted in successful restorative treatment with satisfied case.
[1]. Stewart B, Restoration of the severely worn dentition using a systematized approach for a predictable prognosisInt J Perio Rest Dent 1998 18:47-57. [Google Scholar]
[2]. Spear F, Kokich V, A multidisciplinary approach to esthetic dentistryDent Clin N Am 2007 51:487-505. [Google Scholar]
[3]. Dawson PE, Functional occlusion from TMJ to smile design 2007 ed 2St LouisMosby [Google Scholar]
[4]. Alikhasi M, Kazemi M, Nokar S, Khojasteh A, Sheikhzadeh S, Step-by-step full mouth rehabilitation of a nasopharyngeal carcinoma patient with tooth and implant-supported prostheses: A clinical reportContemp Clin Dent 2011 2:256-60. [Google Scholar]
[5]. Rajendran R, Shivapathasundharam B, Shafer’s Textbook of Oral Pathology 2009 ed 6Elsevier [Google Scholar]
[6]. Cassolato SF, Turnbull RS, XerostomiaClinical aspects and treatment. Gerodontology 2003 20:64-67. [Google Scholar]
[7]. Brennan MT, Woo SB, Lockhart PB, Dental treatment planning and management in the patient who has cancerDent Clin North Am 2008 52:19-37. [Google Scholar]
[8]. Koga DH, Salvajoli JV, Alves FA, Dental extractions and radiotherapy in head and neck oncology. Review of the literatureOral Diseases 2008 14:40-44. [Google Scholar]
[9]. Khan Z, Abdel-Azim T, A direct technique to fabricate an intraoral shield for unilateral head and neck radiationJ Prosthet Dent 2014 112:689-91. [Google Scholar]
[10]. Eckert SE, Desjardins RP, Keller EE, Tolman DE, Endosseos implants in an irradiated tissue bedJ Prosthet Dent 1996 76:45-49. [Google Scholar]
[11]. Nooh N, Dental Implant survival in irradiated oral cancer patients: A systematic review of the literatureInt J of Oral Maxillofac Implants 2013 28:1233-42. [Google Scholar]