Disability has often been described as a physiological deficit. More specifically, a person with a disability has been defined “as anyone who has or had an impairment causing a long term adverse effect upon his or her ability to perform daily activities typical for the person’s stage of development and cultural environment” [1]. Disability affects a wide segment of population of all ages and social classes [2]. According to World Health Organization, an estimated 650 million people live with disabilities around the world [3] and census 2001 has revealed that over 21 million people in India are suffering from one or the other kind of disability. This is equivalent to 2.1% of the country’s population [4]. Children and adolescents with disabilities appear to have poorer oral health than their non-disabled counterparts [5]. Individuals with disabilities or illnesses receive less oral care than the normal population [6].
Dental caries is the most prevalent disease among mentally retarded children worldwide and dental treatment is the greatest unattended health need of the disabled [7]. The oral health of the disabled individuals may be influenced by age, severity of impairment and living conditions. This group of individuals may also not understand and assume responsibility or cooperate with preventive oral health practices. Those who are very young and those who are living in various institutional homes are dependent on parents, siblings or caregivers for general care including oral hygiene. Many caregivers do not have the requisite knowledge to recognize the importance of oral hygiene and proper diet. They may be more susceptible to dental caries if they reside at home and are pampered with cariogenic snacks and other unhealthy eating habits. Some studies have reported a high caries experience in handicapped children, while other studies describe comparable or even lower disease levels [8,9].
An internet based search on the oral health status revealed lack of data on the dentition status and treatment needs of disabled individuals in Central India. Reports are often restricted to examination of a small number of individuals, one specific type of handicapped or one specific type of institute. Hence, the present study was undertaken with the aim to gather baseline data and to determine the dentition status, treatment needs and risk predictors for dental caries among different disabled individuals at four institutions in Indore city, Madhya Pradesh, Central India.
Materials and Methods
A descriptive cross-sectional study was conducted from July to September 2013, at all four institutions for the disabled in Indore city, Madhya Pradesh, Central India. The final sample consisted of 330 subjects (Visually Impaired (VI)-76, Hearing Impaired (HI) - 155, Cerebral Palsy patients (CP) - 36 and Mentally Retarded (MR)- 63. Individuals who were either absent on the day of examination, or not willing to co-operate, or systemically ill were excluded from the study. The participants fell in the age group of 3-22 y. Most of them were from a low socioeconomic stratum and were living under the guidance of care givers.
Ethical Clearance and Consent
The study was reviewed by the institutional ethical committee of ‘Aurobindo College of Dentistry’ and clearance for the same was obtained. Institutional consent was taken from the Head of the Disability Institute, as the subjects were not in a position to understand the consent form.
Data Collection
In this study, the first part of the required data was collected and recorded using printed proforma which consisted of the name of the institution, the age and the gender of the participants, the special group that they belong to, the questionnaire related to their oral hygiene practices (mode of brushing, materials used, and frequency of cleaning) and their previous visit to the dentist. The questionnaire was pre-tested prior to its distribution and the intra reliability of the examiner was assessed by using the Weighted Kappa statistics, which was 90% for deft and 91% for DMFT. The second part consisted of dentition status and treatment needs of the children which were assessed by the WHO Oral Health Assessment form 1997 [10]. The proforma was filled by the trained recorder by interviewing the care givers, conveniently during fieldwork. Clinical examinations were carried out at the institute’s medical room or classroom by a single examiner with the aid of a mouth mirror and CPI probe, under adequate natural light (Type III examination).
Data Analysis
Statistical Package for Social Sciences (SPSS 20.0, Inc., and Chicago, IL) was used for statistical analysis of data. The ANOVA test followed by Tukey post hoc analysis was performed for the statistical evaluation of differences in mean whereas proportions were compared by Chi-square test. Backward conditional logistic regression was performed to identify the risk predictors for dental caries. P value <0.05 was considered as statistically significant.
Results
The mean age for the study population was 13.9±4.71 y. There was a difference in the distribution of subjects according to age group, with only 10.9% of the subjects falling in the age group of 2-7 y, 52.5% subjects were female and 47.5% subjects were male. The majority of the study subjects belonged to Hearing impairment (46.9%) disability group [Table/Fig-1].
Baseline characteristics of disabled subjects (n=330)
| Baseline character | Number of subjects (n) | % of subjects |
|---|
| Age Group(years) | 3-7 | 36 | 10.9 |
| 8-12 | 89 | 26.9 |
| 13-17 | 121 | 36.6 |
| 18-22 | 84 | 25.4 |
| Gender | Female | 173 | 52.5 |
| Male | 157 | 47.5 |
| Type of disability | Visual impairment | 76 | 23 |
| Hearing impairment | 155 | 46.9 |
| Mentally retarded | 63 | 19 |
| Cerebral palsy | 36 | 10.9 |
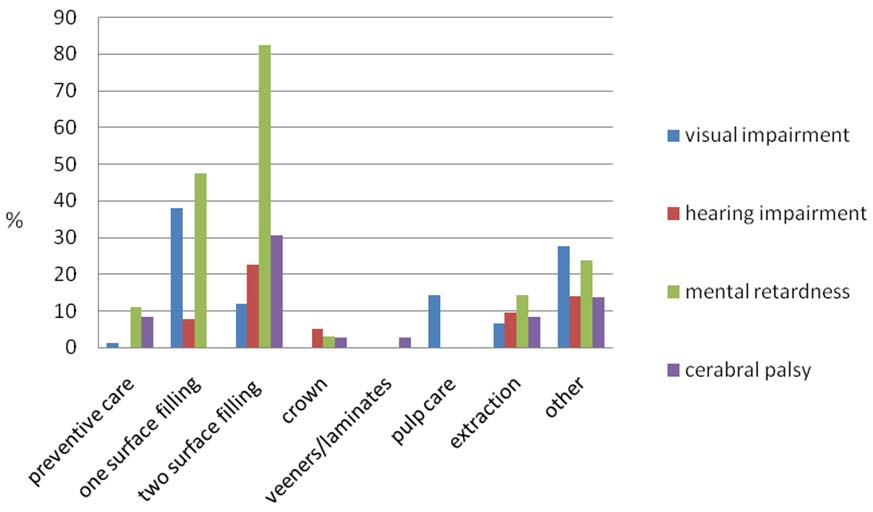
The mean DMFT for all the age groups was 1.26 ±1.80 and the mean deft was 0.59 ± 1.67 [Table/Fig-2]. Analysis of variance tests for DMFT/deft indicates significant differences between the four groups for DMFT and deft. Tukey post-hoc test revealed significant differences among individuals with cerebral palsy, visual impairment, mental retardation and hearing impairment respectively [Table/Fig-3]. It was found that the greatest treatment need is required for the mentally retarded individuals and those suffering from cerebral palsy and the type of greatest treatment need being two surfaces filling,(82.5% of the cases) followed by one surface restoration(47.6% of the cases) [Table/Fig- 4]. Backward conditional logistic regression analysis was performed to identify risk predictors for dental caries. A significant difference was observed between different disability types and age categories (p value<0.05).Individuals who were mentally retarded (OR=1.36) and in the age group of 13-17 y (OR=1.91) were more likely to develop dental caries [Table/Fig- 5].
Caries experience among disability groups
| Disability | DMFT | deft |
|---|
| Mean | S.D | Mean | S.D |
|---|
| Visual impairment(VI) | 0.97 | 1.46 | 0.46 | 1.19 |
| Hearing impairment (HI) | 1.10 | 1.58 | 0.85 | 1.76 |
| Mentally retarded (MR) | 2.06 | 2.36 | 0.16 | 0.75 |
| Cerebral palsy (CR) | 1.22 | 1.89 | 0.53 | 2.84 |
| Total | 1.26 | 1.80 | 0.59 | 1.67 |
ANOVA comparison of caries experience DMFT/deft) among disability groups
| Variables | Comparison group | Sum of Squares | df | Mean Square | P value |
|---|
| DMFT | Between groups | 50.73 | 3 | 16.91 | 0.00(S) |
| Within groups | 1022.26 | 326 | 3.14 | - |
| deft | Between groups | 22.8 | 3 | 7.63 | 0.04(S) |
| Within groups | 902.52 | 326 | 2.77 | - |
Treatment needs among dirrerenc eisability groups
Conditional Backward Logistic Regression analysis for the study population with dental caries present in the dentition as dependent factor.
| Variables | Categories | Odds ratio | CI(Confidence interval) | p-value |
|---|
| Age group | 2-7 years | 0.68 | 0.37-1.22 | 0.03* |
| 8-12 years | 1.48 | 0.86-2.55 |
| 13-17years | 1.91 | 1.08-3.40 |
| 18-22years | 1x | - |
| Type of disability | VI | 0.64 | 0.32-1.28 | <0.001* |
| HI | 0.46 | 0.20-1.06 |
| MR | 1.36 | 0.72-2.56 |
| CP | 1x | - |
Variables entered on step 1:Age, type of disability, gender, method of teeth cleaning, material used for cleaning, frequency of brushing, time of cleaning, duration of brushing and visit to dentist. Variables removed on step 2: method of teeth cleaning. Variables removed on step 3: gender. Variables removed on step 4: time of teeth cleaning. Variables removed on step 5: duration of brushing. Variables removed on step 6: visit to dentist. Variables removed on step 7: frequency of brushing. Variables removed on step 8: material used for teeth cleaning 1x: reference category
*: p<0.05(statistically significant)
Discussion
In the present study, the mean age of the sample was 13.9±4.71y and the caries experience in permanent dentition was 46.4% with mean DMFT 1.26±1.80 and 14.5% in deciduous dentition with mean deft 0.59±1.67. If comparisons are made on a national platform, the caries experience of these institutionalized children is lesser than the National average for normal children as reported in the survey conducted by Govt. of India in 2003-04. It has been estimated by the National oral health survey in 2003-2004 that the prevalence of dental caries in five year olds is 51.9% and 12 years old is 63.1% [7]. Low caries prevalence could be due to the fact that the institutionalised children were having supervised meals that are regularly checked and are mostly free from sugar.
When intergroup comparisons were made, the mean DMFT was found to be 2.06±2.36 among mentally retarded children which is in close agreement with the previous study conducted by Manish Jain et al., [3], where mean DMFT was 2.01±2.26. This may be because of individuals’ poor socio-economic status, poor oral hygiene, and practical difficulties during treatment session and underestimation of treatment needs [3]. Henequen [11] stated that dental caries is the most prevalent disease amongst mentally retarded children. The important reasons for this could be in adequate recall systems, practical difficulties during treatment sessions, socio-economic status of the individuals, underestimation of treatment need or pain [12]. In the present study, the mean caries experience for the mentally retarded group subjects was somewhere higher than the National average. Gizani [13] did a study on mentally challenged children and found the mean DMFT to be 2.7; this was higher than our study. This mean difference existed in spite of the children receiving timely dental care and preventive interventions being applied to them.
Hearing impairment subjects had the second highest caries prevalence (45.8% of the cases). This could possibly be due to barriers in communication for proper health education & poor oral hygiene habits. The prevalence is in close agreement with the study conducted by Suma et al., [5], who reported 42% of the cases with caries prevalence. The results are however contradictory to the finding of study done by Jain et al., [3] and Aruna [14] where in their study they found a prevalence of 93.33% of the cases and 93.09% of the cases respectively. This may be due to geographical and cross-cultural variations.
In the present study the visual impairment subjects had a caries experience of 40.8%. Prashanth GM et al., [9] conducted a study to assess dental caries experience among 6-18 y old blind children of residential school, Bangalore, Karnataka, India. The study concluded that 68% of the study subjects were having dental caries which is very high. They concluded that these groups of disabled children were highly neglected. In the present study, the mean DMFT and deft were 0.97 and 0.46 respectively. Reddy et al., [12] did a study on institionalized handicapped children which included both hearing impaired and visually impaired groups. They concluded that the mean DMFT among the hearing impaired group was 1.4±1.95 and for the visually impaired group was 0.94±1.45.These results are comparable to our study. In the present study there was a statistically significant difference between all 4 disabilities groups for mean DMFT/deft (p=0.00/0.04).The highest DMFT was recorded in the individuals of the mentally impaired group. It is valuable to know that the majority of the individuals in the present study were using tooth brush with tooth paste daily as part of their oral health regime. Most of the subjects brushed once daily-in the morning. There is good oral hygiene awareness as the institutionalized children are periodically monitored by various organizations.
The treatment need was high among the mentally retarded subjects as compared to other groups. Two-surface filling was the most frequent treatment need for the population studied. The reason may be that the mentally retarded children are the most difficult ones to handle and treat. Among the subjects with visual impairment, preventive care & pulp care were required by 14.5% of the cases, which is in close agreement with the Indian study conducted by Manish Jain et al., [2] which indicated preventive care & pulp care requirements for subjects to be 11.9% and 19.4% respectively. Unfortunately, the methods generally used to maintain oral hygiene i.e., visual perception of caries, removal and tooth brushing to remove plaque are of no use for the visually impaired children. Also, it was concluded by Sarheed [15] that the main difference between normal and visually impaired children were that normal children could remove plaque more easily than visually impaired children. The difficulty in removing bacterial plaque is the main factor responsible for development of caries, and continual motivation to correct oral hygiene procedures is fundamental in order to keep a good oral hygiene in blind patients [16]. It is interesting to note that the caries prevalence is highest in mentally retarded children. This is attributed by most of the authors to the difficulty in manual dexterity for the children, however Shaw et al., [8] reported that manual dexterity is not related to oral hygiene. Among all disability groups, the mentally retarded individuals (87.3% of the cases) used toothbrush to clean their teeth. These findings were similar to the study conducted by Nural & Bekiroglu et al., [4] and Adivaso [17] which concluded that if knowledge of oral health of special children are improved, it will bring a better oral health to these children.
Backward conditional logistic regression analysis results showed that there was a significant difference in the type of disability and age categories. Individuals who were mentally retarded and individuals with cerebral palsy were more likely to have dental caries. Individuals in the age group of 13-17 y were more likely to have dental caries. Similar findings were reported by Jain et al., [3] where they found higher caries prevalence in this age group. Prashant [18] stated that for special children a little extra care by the parent or caregiver regarding oral hygiene could produce drastic results in reduction of dental caries.
Conclusion
The findings of the present study showed that on the whole the caries experience was low but the treatment need was high among the study population. The institutionalized disability groups had good oral hygiene awareness. However, the frequency of dental visit was less among all the disability groups. Therefore, a prevention-based intervention & oral health promotion programme, facilitating access and regular use of oral health service is recommended for these special disabled institutionalized children of Indore city and India as a whole. Further research can be done where preventive interventions have been done and have produced some results, which will give us an idea about how these special children are responding to various preventive methods and regimes.
Variables entered on step 1:Age, type of disability, gender, method of teeth cleaning, material used for cleaning, frequency of brushing, time of cleaning, duration of brushing and visit to dentist. Variables removed on step 2: method of teeth cleaning. Variables removed on step 3: gender. Variables removed on step 4: time of teeth cleaning. Variables removed on step 5: duration of brushing. Variables removed on step 6: visit to dentist. Variables removed on step 7: frequency of brushing. Variables removed on step 8: material used for teeth cleaning 1x: reference category*: p<0.05(statistically significant)