This case report describes the Revascularization of a Permanent Immature Mandibular Premolar with Pulp Necrosis and apical periodontitis. Access opening was done & the canal was disinfected with copious irrigation using 2.5% NaOCl and triple antibiotic paste (Ciprofloxacin, Metronidazole, and Minocycline) as intracanal medicament. After the disinfection protocol is complete, it is followed by revascularization procedure. The apex was mechanically irritated to initiate bleeding into the canal to produce a blood clot to the level just below the level of cementoenamel junction. Mineral trioxide aggregate was placed over the blood clot followed by bonded resin restoration above it. After one year follow up; the patient was asymptomatic, no sinus tract was evident. Apical periodontitis was resolved, and there was radiographic evidence of continuing thickness of dentinal walls.
Apical periodontitis, Mineral trioxide aggregate, Open apex, Revascularization, Triple antibiotic paste (TAP)
Case Report
A 12-year-old child patient was referred to the Department of Conservative Dentistry & Endodontics for the evaluation of left Mandibular 2nd premolar. The patient had a history of swelling on the left mandibular region one month back, for which he received medication. The swelling got regressed on taking medication but continued to have discomfort on chewing.
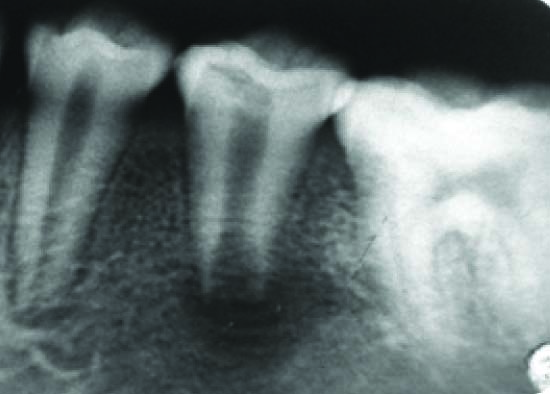
On clinical examination, tooth appeared intact without caries. Radiographically the tooth had an incompletely formed root with open apex associated with a large Periapical radiolucency [Table/Fig-1]. Periodontal probing was within normal limits. Diagnostic testing was inconclusive on cold and electric pulp testing & was slightly symptomatic to percussion.
Preoperative radiograph of tooth-45 showing an open apex with a large periapical radiolucency
An attempt to regeneration of pulp was made because of the open apex & thin dentinal walls are susceptible for future fracture. The technique followed was similar to the one proposed by Banchs & Trope in 2004 with few modifications in irrigation regimen [1].
Procedure
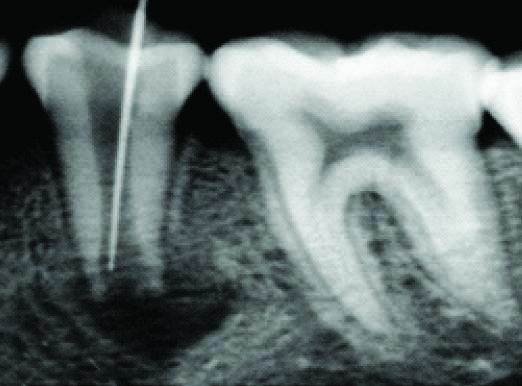
First visit: An access cavity was made under rubber dam, purulent hemorrhagic drainage obtained and the necrotic nature of the pulp confirmed. A K-file is introduced into the canal to establish working length [Table/Fig-2]. Root canal was irrigated with 20 ml of 2.5% NaOCl for 10 min, 2 mm short of the apex, and the NaOCl is slowly expressed from the syringe to prevent its introduction into the periapical tissues. Initial NaOCl irrigation is followed by irrigation with 5 ml sterile saline and final rinse with 10 ml 2% CHX. The canal was dried with paper points, and Triple Antibiotic Paste (Ciprofloxacin, Metronidazole and Minocycline) was placed inside the canal. The medicament is made by mixing equal doses of the three antibiotics with sterile saline to a paste-like consistency. Access cavity was sealed with temporary restorative material (Cavit).
Determining working length with a K-file.,
Second visit (four weeks later): Patient was asymptomatic, reporting no pain postoperatively. The temporary restoration was removed and the medication was removed gently from the canal using 20 ml of 2.5% NaOCl followed by same irrigation protocol followed in the 1st appointment. The canal appeared clean and dry, with no signs of inflammatory exudates.
A sterile size #30 K-file was used to irritate the tissue gently to create some bleeding into the canal. Bleeding should be controlled so that it does not extend beyond a point approximately 3 mm apical to the CEJ. The bleeding was left for 15 min so that the blood clot was formed. MTA was carefully placed over the blood clot, followed by a wet cotton pellet and IRM [Table/Fig-3].
Radiograph taken 4 weeks after the placement of triple antibiotic paste. Radiographic signs of healing are evident
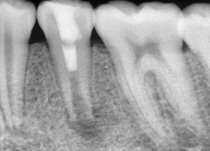
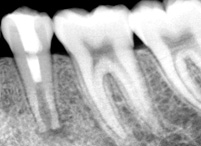
Third visit (1day later): Cotton pellet was removed over the set MTA & IRM was replaced with a bonded resin restoration to seal the access [Table/Fig-4].
Radiograph showing MTA & bonded resin restoration over it
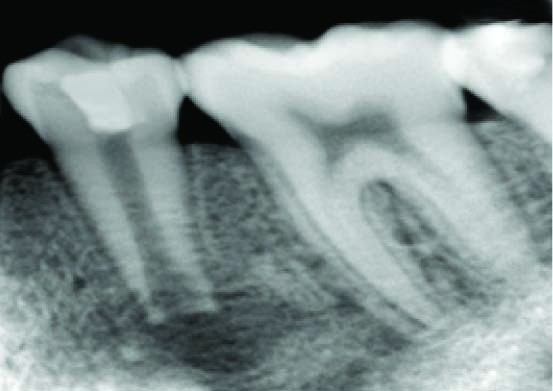
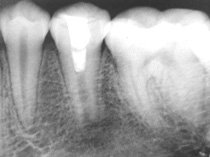
Recall visits: After three months-the patient was asymptomatic, with no signs of the sinus tract. The radiograph showed resolution of the radiolucency. After six months, the patient continued to be asymptomatic, with no signs of the sinus tract and an indication of continued development of the apex of the tooth [Table/Fig-5]. After one year, closure of the apex and thickening of the dentinal walls was observed. A mineralized bridge appeared to develop beneath the MTA [Table/Fig-6].
Six-month recall radiograph. Periapical radiolucency has completely disappeared & signs of apical closure and continued root development can be seen
One year recall radiograph, closure of the apex and thickening of the dentinal walls was observed. A mineralized bridge appeared to develop beneath the MTA
Discussion
The treatment of pulpal necrosis in an immature tooth with an open apex presents a unique challenge to the dentist. The consequences of loss of pulp vitality in a immature tooth include a poor crown-root ratio, a root with very thin walls, an increased risk of fracture, and an open apex [2].
Previously, clinicians treated these teeth with Traditional Apexification procedures or the use of apical barriers [3]. Traditional Apexification using long-term calcium hydroxide has proven to be successful, but it needs multiple appointments over a period of months & susceptibility to cervical fracture is increased [4,5]. The artificial apical barrier technique using MTA has proven to be predictable and successful [6]. When compared with traditional apexification procedures, this technique requires less appointments [7]. The disadvantage of both the techniques is that there is no thickening of the root wall or continued development of the root.
In 1960, Nygaard-Ostby attempted Revascularization procedure in a necrotic, infected tooth with apical periodontitis. However, the results were limited because of limitations in materials and instruments available at that time [8]. Iwaya et al., described a revascularization procedure for treating a necrotic immature mandibular second premolar with a chronic apical abscess. After 30 months they noted thickening of the root canal walls by mineralized tissue and continued root development [9].
Banchs and Trope in 2004 described a new treatment procedure for the management of a necrotic immature mandibular second premolar with an open apex called “Revascularization” [1]. The authors used sodium hypochlorite & Chlorhexidine as irrigating solutions and a combination of three antibiotics (Ciprofloxacin, Metronidazole and Minocycline) for disinfecting the canals as described by Hoshino et al., [10]. After two years, they found that root walls are thickened (and stronger) and the apex has formed normally.
The success of non-surgical endodontic treatment method is based on appropriate cleaning, shaping, asepsis, and filling of the root canal [11]. Revascularization in luxated or avulsed teeth with open apices is a possibility & almost predictable under ideal conditions and with chemical decontamination of the root surface [12,13].
It is important to understand the biologic features permitting revascularization in young avulsed teeth. The immature avulsed tooth has an open apex, short root, and intact but necrotic pulp tissue. It was apparent the larger the foramen, the greater is the opportunity for ingrowth of a new blood supply and the reestablishment of new tissue [14,15].
It has been experimentally shown that the apical portion of a pulp might remain vital and proliferate coronally after reimplantation, replacing the necrotized coronal portion of the pulp [16].
Banchs and Trope in 2004, described a revascularization procedure for the treatment of a necrotic immature mandibular second premolar with an open apex and a large apical lesion, indicating that it might be possible to replicate the unique circumstances of an avulsed tooth to revascularize the pulp in infected necrotic immature roots [1]. After them, many successful case reposts have been published by various authors using revascularization approach & most of them were performed on incisors and premolars of children 8–14 y of age [17–22].
In the case presented here, mechanical instrumentation cannot be performed in these teeth because of the open apex and thin dentinal walls. So, the removal of necrotic tissue from the root canal is accomplished by gently irrigating the root canal with NaOCl because of its tissue dissolving ability & potent antimicrobial activity. CHX is used as a final rinse because of its antimicrobial activity and its substantivity [22]. When irrigating with NaOCl, It is extremely important to ensure that the irrigating needle is loose in the canal and that the NaOCl irrigation is performed very slowly. The needle should be introduced into the root canal to a point 2 mm short of the apical foramen [1,16,23]. We used a triple antibiotic paste proposed by Hoshino et al., [10] for disinfection of the canal. TAP was proved to be biocompatible & can help promote functional development of the pulp–dentin complex [24]. Blood clot was created in the canal after disinfection. This approach has been supported by many researchers [1,20,21]. This blood clot acts as a matrix for the growth of new tissue into the pulp space. Researchers have assumed that stable blood clot serve as a scaffold & provide factors that stimulate their cell growth and differentiation of these cells into odontoblast-like cells [18,23].
Bacteria-tight seal is created coronally to inhibit bacterial invasion into the pulp space. Double seal with MTA to a level below the CEJ covered by a bonded resin coronal restoration was created to achieve good sealing [1,21].
In teeth with open apices, it is possible that some pulp tissue may have survived apically, even though most of the pulp is devitalized and heavily infected. Some authors suggested that regeneration can occur from vital pulp cells remaining at the apical end of the root canal, the multipotent dental pulp stem cells, stem cells in the periodontal ligament and stem cells from apical papilla [25].
This case has been followed for 1year and can be considered as success because the walls are thickened and the development of apex is seen with absence of clinical symptoms.
Conclusion
Success of the endodontic treatment relies upon the elimination of bacteria from the root canal. From the existing literature, it is clear that TAP can be effectively used for sterilization of canals and healing of periapical pathology. It is worth attempting revascularization, because the advantage of this procedure lies in the possibility of further root development and reinforcement of dentinal walls by deposition of hard tissue, thus strengthening the root against fracture. Few limitations of revascularization are long-term clinical results are as yet not available and whether the newly regenerated tissue is truly pulp or only pulp-like is also uncertain.
[1]. Banchs F, Trope M, Revascularization of immature permanent teeth with apical periodontitis: new treatment protocolJ Endod 2004 30:196-200. [Google Scholar]
[2]. Cotti E, Mereu M, Lusso D, Regenerative Treatment of an Immature, Traumatized Tooth With Apical Periodontitis: Report of a CaseJ Endod 2008 34:611-16. [Google Scholar]
[3]. Yates JA, Barrier formation time in non-vital teeth with open apicesInt Endod J 1988 21:313-19. [Google Scholar]
[4]. Andreasen JO, Farik B, Munksgaard EC, Long-term calcium hydroxide as a root canal dressing may increase risk of root fractureDent Traumatol 2002 18:134-37. [Google Scholar]
[5]. Doyon GE, Dumsha T, von Fraunhofer JA, Fracture resistance of human root dentin exposed to intracanal calcium hydroxideJ Endod 2005 3:895-97. [Google Scholar]
[6]. Witherspoon DE, Small JC, Regan JD, Retrospective analysis of open apex teeth obturated with mineral trioxide aggregateJ Endod 2008 34:1171-76. [Google Scholar]
[7]. Simon S, Rilliard F, Berdal A, The use of mineral trioxide aggregate in one-visit apexification treatment: a prospective studyInt Endod J 2007 40:186-97. [Google Scholar]
[8]. Ostby BN, The role of the blood clot in endodontic therapy: an experimental histologic studyActa Odontol Scand 1961 19:324-53. [Google Scholar]
[9]. Iwaya SI, Ikawa M, Kubota M, Revascularization of an immature permanent tooth with apical periodontitis and sinus tractDent Traumatol 2001 17:185-87. [Google Scholar]
[10]. Hoshino E, Kurihara-Ando N, Sato I, In-vitro antibacterial susceptibility of bacteria taken from infected root dentine to a mixture of ciprofloxacin, metronidazole and minocyclineInt Endod J 1996 29:125-30. [Google Scholar]
[11]. Taneja S, Kumari M, Prakash H, Non-surgical healing of large periradicular lesions using a triple antibiotic paste: A case seriesContemporary Clinical Dentistry 2010 1:31-35. [Google Scholar]
[12]. Kling M, Cvek M, Mejàre I, Rate and predictability of pulp revascularization in therapeutically reimplanted permanent incisorsEndod Dent Traumatol 1986 2:83-89. [Google Scholar]
[13]. Johnson WT, Goodrich JL, James GA, Replantation of avulsed teeth with immature root developmentOral Surg Oral Med Oral Pathol 1985 60:420-27. [Google Scholar]
[14]. Kling M, Cvek M, Mejare I, Rate and predictability of pulp revascularization in therapeutically reimplanted permanent incisorsEndod Dent Traumatol 1986 2:83-89. [Google Scholar]
[15]. Skoglund A, Tronstad L, Pulpal changes in replanted and autotransplanted immature teeth of dogsJ Endod 1981 7:309-16. [Google Scholar]
[16]. Iwaya SI, Ikawa M, Kubota M, Revascularization of an immature permanent tooth with apical periodontitis and sinus tractDent Traumatol 2001 17:185-87. [Google Scholar]
[17]. Shah N, Logani A, Bhaskar U, Aggarwal V, Efficacy of revascularization to induce apexification/apexogensis in infected, nonvital, immature teeth: a pilot clinical studyJ Endod 2008 34:919-25. [Google Scholar]
[18]. Huang GT, Sonoyama W, Liu Y, The hidden treasure in apical papilla: the potential role in pulp/dentin regeneration and bioroot engineeringJ Endod 2008 34:645-51. [Google Scholar]
[19]. Chen MY, Chen KL, Chen CA, Responses of immature permanent teeth with infected necrotic pulp tissue and apical periodontitis/abscess to revascularization proceduresInt Endod J 2012 45:294-305. [Google Scholar]
[20]. Reynolds K, Johnson JD, Cohenca N, Pulp revascularization of necrotic bilateral bicuspids using a modified novel technique to eliminate potential coronal discolouration: a case reportInt Endod J 2009 42:84-92. [Google Scholar]
[21]. Jung IY, Lee SJ, Hargreaves KM, Biologically based treatment of immature permanent teeth with pulpal necrosis: a case seriesJ Endod 2008 34:876-87. [Google Scholar]
[22]. Chen MY, Chen KL, Chen CA, Responses of immature permanent teeth with infected necrotic pulp tissue and apical periodontitis/abscess to revascularization proceduresInt Endod J 2012 45:294-305. [Google Scholar]
[23]. Neha K, Kansal R, Garg P, Management of immature teeth by dentin-pulp regeneration: a recent approachMed Oral Patol Oral Cir Bucal 2011 16:e997-1004. [Google Scholar]
[24]. Bose R, Nummikoski P, Hargreaves K, A retrospective evaluation of radiographic outcomes in immature teeth with necrotic root canal systems treated with regenerative endodontic proceduresJ Endod 2009 35:1343-49. [Google Scholar]
[25]. Gronthos S, Brahim J, Li W, Fisher LW, Cherman N, Boyde A, Stem cell properties of human dental pulp stem cellsJ Dent Res 2002 81:531-35. [Google Scholar]