Evaluation of Proximal Femoral Geometry in Plain Anterior-Posterior Radiograph in Eastern-Indian Population
Sanchita Roy1, Rajib Kundu2, Shyamalendu Medda3, Avanish Gupta4, Baljit Kaur Nanrah5
1 Assistant Professor, Department of Anatomy, IPGME & R, Kolkata, India.
2 Associate Professor, Department of Anatomy, IPGME & R, Kolkata, India.
3 Demonstrator, Department of Anatomy, IPGME & R, Kolkata, India.
4 Assistant Professor, Department of Anatomy, IPGME & R, Kolkata, India.
5 Assistant Professor, Department of Anatomy, IPGME & R, Kolkata, India.
NAME, ADDRESS, E-MAIL ID OF THE CORRESPONDING AUTHOR: Dr. Sanchita Roy, 207A/2 Moitri Abasan, Garfa Main Road, Kolkata-78, India. Phone : 9831767953, E-mail : doctor_sanchita@yahoo.co.in
Background: The morphologic features of the proximal femur are used in preoperative planning prior to total hip arthroplasty. The standard commercially available marketed prostheses sometimes may not be the best fit to all subjects because of the large anatomic variation among different population. Orthopaedic surgeons always stress the need for a proper implant-patient match in hip joint replacements to avoid post-operative complication of mismatch which may affect the ultimate outcome of the operation.
Aim: The present study was undertaken to measure the important parameters of upper end of femur in elderly Eastern Indian population which will help the prosthetist to manufacture ideal implant for the local population. This will also help the orthopaedic surgeons while positioning the implants during total hip replacement (THR) procedure in this population.
Materials and Methods: Measurements were made on both sides, left and right from anterior-posterior radiograph of 102 subject (>50yrs, 42 male and 60 females) using AGFA software. Three parameters femoral head diameter (FHD), neck-shaft angle (NSA) and horizontal off-set (HO) were measured.
Results: SPSS software used for data analysis. Gender- wise no significant differences were found in NSA and FHD, but HO was significantly lower in female than that of male (p<.05).The values on both sides didn’t differ significantly.
Conclusion: Improved knowledge of the morphology of the proximal femora will assist the surgeon in restoring the geometry of the proximal femur during total hip arthroplasty and the data could be used as a guideline to design a more suitable implant for Eastern Indian population.
Anatomy, Neck-shaft angle, Proximal femur, Offset, Total hip arthroplasty
Introduction
Presently in the developing countries like India the frequencies of total hip replacement (THR) have been increased to a great extent. The morphological features of the proximal femur, relied on radiographs or computed tomography, are used in preoperative planning prior to total hip arthroplasty because it is vital to match the dimension of the implant with those of the femur. Otherwise, inappropriate sized or incorrectly placed prosthesis might cause aseptic loosening and improper load distribution causing huge discomfort to the patient thus ultimately affecting long term success of the operation [1,2].
Most of the standard prostheses available in the market are manufactured based on the data available from the Western population. Mainly three parameters femoral head diameter, horizontal offset and neck shaft angle are considered for the manufacture of the prosthesis. Many studies evaluating proximal femoral geometry based on dry bone, radiographs or computed tomography, showed substantial variations in these parameters among populations of different geographic regions [3,4]. Nelson & Megyesi studied sex and ethnic differences in bone architecture and therefore established the need for developing gender-specific implants [5]. In their study Chaubber & Singh showed higher value of various parameters on left side than that of right, as whether a person is right handed or left handed, more people use left lower limb for more weight bearing [6]. A population based study by Nurzenski et al., showed that life style factors also influence geometric indices of bone strength in the proximal femur [7]. So, to minimise post operative complications the implants should be designed by taking into account the parameters of the local population. Preoperative radiographic assessment however is complicated by the inability of some patients with advanced osteoarthritis to internally rotate their hips for standard positioning. The offset measured from their radiographs therefore could deviate from their true femoral offset. This present study evaluated the important morphological features of upper end of femur mainly femoral head diameter, neck shaft angle and horizontal offset from anterior-posterior radiograph maintaining the standard positioning of the individual without having gross abnormalities in the hip joint.
The aims of this study were to
Provide data which can give idea to engineers and surgeons in the development and placement of implants during THR in local population; thus help them to exert better performance in their respective specialities.
Evaluate any variations of these measurements attributable to side and gender.
Materials and Methods
Determination of the geometrical measurement of upper end of femur was the main target. For this study skiagrams of pelvis (including both hip joints & proximal femurs [Table/Fig-1a] of male and female population aged more than 50 y, were collected from the radiology department of IPGME&R, Kolkata during the period of 2011, Dec to 2013, Dec. Xrays of the hip joint (without any gross abnormality involving the joint) of patients, who came to the radiology department as a part of their treatment for different reasons, were taken for this study. A.P views were taken maintaining standard radiographic positioning using same radiographic machine (of ELECTROMEDICAL Company). One hundred and two skiagrams which grossly appeared normal were measured. AGFA digital software was used for measurement and all the measurements were taken by the single observer under guidance of an experienced radiologist and radiographer [Table/Fig-1a,b].
Skiagram of both hip joint (AP view) showing proximal femur

Schematic presentation showing measurements of the parameters
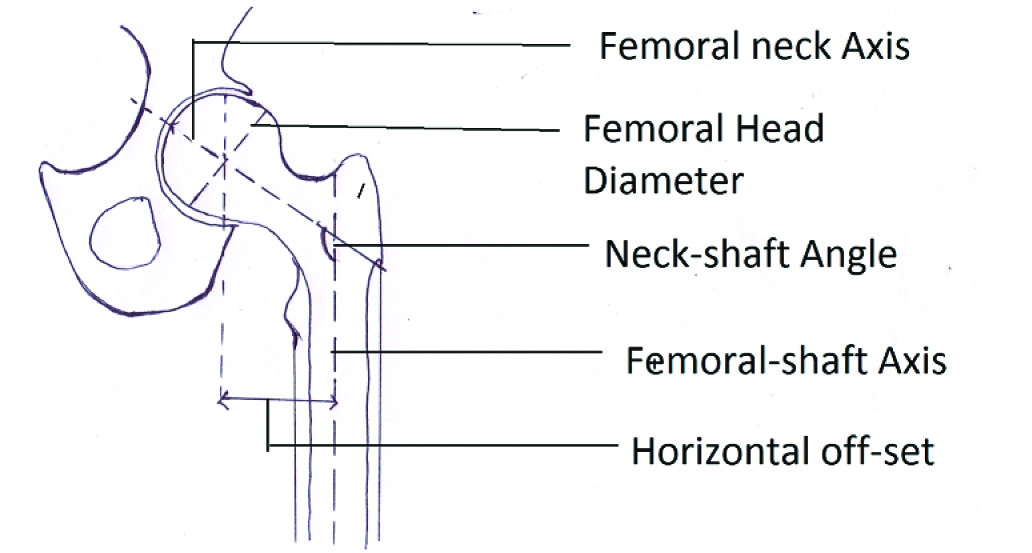
Parameters measured were [Table/Fig-1b]
Femoral Neck Shaft Angle (NSA) - created by the intersection of two lines, proximal femoral shaft axis and the line joining two points (i) the centre of femoral head and (ii) the centre of the femoral neck (neck axis).
Femoral head diameter (FHD) - diameter of a perfect circle drawn around the femoral head.
Horizontal offset (HO) - perpendicular distance from the centre of femoral head to the axis of the femoral shaft.
All measurements were statistically analysed using SPSS software to compare between genders and femoral sides and summarized in [Table/Fig-2,3].
Summary of the measured parameters of both sides in both sexes., *CI – Confidence Interval; LB–Lower Bound; UB‡ – Upper Bound
| Parameters | | Male (n=42) | Female (n=60) |
|---|
| 95% CI* of mean | Mean±SD | p- value | 95% CI* of mean | Mean+/-SD | p- value |
| Neck-shaft angle(o) | Left | LB-129.75 | 130.99±3.77 | 0.9 | LB-129.37 | 130.2±2.56 | 0.52 |
| UB‡-132.14 | UB‡-131.03 |
| Right | LB-129.76 | 130.89±3.61 | LB-129.61 | 129.93±3.82 |
| UB-132.0 | UB-131.0 |
| Femoral head diameter (cm) | Left | LB-4.51 | 4.67±0.52 | 0.67 | LB-4.34 | 4.46±0.41 | 0.74 |
| UB-4.83 | UB-4.61 |
| Right | LB-4.48 | 4.63±0.46 | LB-4.29 | 4.42±0.46 |
| UB-4.77 | UB-4.59 |
| Horizontal offset (cm) | Left | LB-3.71 | 3.86±0.47 | 0.89 | LB-3.33 | 3.5±0.55 | 0.12 |
| LB-4.0 | UB-3.68 |
| Right | LB-3.71 | 3.85±0.47 | LB-3.48 | 3.6±0.67 |
| UB-3.99 | UB-3.79 |
Comparison of the parameters between genders including both sides
| Parameters | Mean in male | Mean in female | P value |
|---|
| Neck-shaft angle(o) | 131.0 | 130.37 | 0.21 |
| Femoral head diameter (cm) | 4.6 | 4.45 | 0.21 |
| Horizontal offset(cm) | 3.85 | 3.57 | 0.0009 |
The goodness-of-fit test was used to verify the normality assumption for each group of data and found to be normally distributed. There was no significant differences between the left and right sided parameters (p>.05 in all the cases). Statistical analyses comparing parameters between males and females were performed using unpaired t-tests, the level of significance was set at p<.05. By the analysis of data it was observed that average NSA and FHD in female was 130.370 & 4.45cm respectively which was less than that of in male, 1310 & 4.6cm respectively, but the differences were not statistically significant. Women had less HO than men (3.57cm Vs 3.85 cm) which was statistically significant (p<.001) [Table/Fig-3].
Discussion
The biomechanical goals of total hip arthroplasty are to create a stable anatomical articulation with an optimum range of movement, to restore normal biomechanics for muscular efficiency and to equalize limb length. The present study was undertaken to compare the differences in dimensions between femurs of West Bengal population and those of population from other regions in order to solve the problem of a possible geometric mismatch between a selected implant and the dimensions of the hip joint of the study population concerned.
Neck-shaft angle is an important parameter of upper femur geometry which is used for designing as well as placing the femoral implant during total hip replacement operation. According to Standring et al., the average NSA in adults as 1250 [8]. In our study average NSA in male and female was 1310 & 130.370 respectively. The measurement of NSA & HO by radiographs however is affected by femoral neck version, hip rotation and femoral bowing [1,9]. Unlike many studies we measured the neck-shaft angle based on the axis of proximal femur. This will replicate the actual NSA when performing THA, as the stem of the femoral component was designed to restore the anatomy of only proximal femoral region. There was a change toward varus angulations of the NSA (an inward deviation of the distal femoral segment) if the measurement was performed using the long axis of the femoral shaft instead of using the axis of the proximal femur [10]. Anthropologist Kate BR [11] worked on 1000 dry femora and the average angle was found to be 128.40. He observed difference in the angle between the various races of India. He found the Formosans to have lowest average NSA (125.60) & Andamanians the highest angle (1340) [12]. Saikia reported the average NSA in the North Indian population as 1390.The comparison of NSA with other studies shown in [Table/Fig-4].The difference in our study may be due to consideration of proximal neck shaft axis. If the long axis is considered for manufacture of implant the prosthesis will unnecessarily remove the medial cortex of the femoral diaphysis thus causing unstable anatomical articulation affecting the normal biomechanics of hip joint [9].
Comparison of parameters with other study
| Parameters | B.R RAWAL et al., [17] N=98(on Indian population) | Rubin et al., [14] N=32(on swiss pop) | Husmann et al., [18] N=310(on French pop) | Mahaisvariya et al., [19] N=108(on Thai pop) | R.C Siwach et al., [20] (on European pop.) | Present Study N=204 (on Eastern Indian pop.) |
|---|
| Neck-shaft angle(0) | 124.42±5.49 | 122.9±7.6 | 129.2±7.8 | - | - | 130.57±3.0 |
| Femoral head diameter(mm) | 45.41±3.66 | 43.4±2.6 | | 43.98±3.47 | 43.53±3.4 | 45.30±4.7 |
| Horizontal offset(mm) | 40.23±4.85 | 47±7.2 | 40.5±7.5 | - | 38±5.52 | 36.93±5.2 |
Femoral head diameter is another important parameter which is to be considered during prosthesis manufacture. In the present study mean head diameter is 4.6cm and 4.45cm in male and females respectively (p<.05). In this parameter also no significant differences were found among left or right side. The findings of this study are compared with other studies in [Table/Fig-3].
Femoral horizontal offset restoration is also essential to improve function and longevity of hip arthroplasty. Charnley [13] considered it to be a factor under the control of the surgeon at the time of hip replacement surgery, the more lateral position of the femur with greater horizontal offset was said to increase the range of motion and decrease the incidence of impingement of the femoral head on the pelvis thus decrease the post-operative complications. Though CT scan is more accurate, the plain radiography is definitely the most cost effective and convenient method for offset measurement in the developing countries like India [14]. Our data showed that the average horizontal offset was 3.85 cm and 3.57 cm in male and female respectively. TR Deshmukh et al., [15] in 2010 showed that the mean HO was around 3.8 cm in both male & female population in Vidharva region of Maharasthra. Unnantana A et al., [10] who worked on proximal femoral geometry found that the HO was higher in females. Femoral offset recorded in other studies is shown in [Table/Fig-4]. Hip rotation influence the amount of horizontal offset found in plain radiography. Maruyama et al.,[9] showed that the average horizontal offset was approximately 3 mm larger when measured in internal rotation versus neutral rotation. The value of horizontal offset therefore may be underestimated on the standard radiograph obtained preoperatively. We have tried to nullify this rotation effect by selecting subjects without having any gross pathology involving hip joint and maintaining standard positioning while taking the radiography.
Our study demonstrated that the proximal femoral geometry was different between genders. All the parameters were higher in males than those from the females. A recent arthroplasty development has been focused on gender-specific implants which emphasizes the need of our study. However, one study showed that with the current implant systems, it was sufficiently versatile to address the different size and offset needs of male and female patients [16].
In our study we did not find any significant differences in the value of the measured parameters among left or right side in both sexes. Limitation of our study was that all the measurements were taken from two dimensional images, thus some of the important parameters like neck inclination or rotation could not be calculated. Computer tomography scan is the best option for measuring all the parameters but in the developing countries like India plain radiographic measurement is a better cost effective option.
Conclusion
By using anterior – posterior radiograph and standard positioning of the subjects, we obtained the measurement of three important parameters. These detailing of the proximal femur could help prosthesis manufacturer and surgeons for better understanding the proximal femoral geometry in Eastern Indian population and thus the biomechanics of total hip arthroplasty.
[1]. Kay RM, Jaki KA, Skaggs DL, The effect of femoral rotation on the projected femoral neck-shaft angleJ Pediatr Orthop 2000 20:736-39. [Google Scholar]
[2]. McGrory J, Morrey BF, Cahalan TD, Kai-Nan AN, Cabanela ME, Effect of femoral offset on range of motion and abductor muscle strength after total hip arthroplastyJ Bone Joint Surg 1995 77:865-69. [Google Scholar]
[3]. Crabtree N, Lunt M, Holt G, Kroger H, Burger H, Hip geometry, bone mineral distribution and bone strength in European men and women: The EPOS StudyBone 2000 27:151-59. [Google Scholar]
[4]. Greendale GA, Young JT, Huang MH, Bucur A, Wang Y, Seeman T, Hip axis length in midlife Japanese & Caucasians US residents: No evidence for an ethnic differenceOsteoporos Int 2003 14:320-25. [Google Scholar]
[5]. Nelson DA, Megyesi MS, Sex and ethnic differences in bone architectureCurr Osteop Rep 2004 2:65-69. [Google Scholar]
[6]. Chhibber SR, Singh I, Asymmetry in muscle weight and one sided dominance in the human lower limbsJ Anat 1970 106(553-56) [Google Scholar]
[7]. Nurzenski MK, Briffa NK, Price IR, Khoo CCB, Devine A, Beck JT, Geometric Indices of Bone Strength Are Associated With Physical Activity and Dietary Calcium Intake in Healthy Older WomenJ Bone Miner Res 2007 22(3):416-24. [Google Scholar]
[8]. Standring Susan, Ellis H, Collins P, Johnson D, Shah P, Wigley C, The Anatomical Basis of Clinical Practice 2000 39th EditionElsevier Churchil Livingstone:1431 [Google Scholar]
[9]. Maruyama M, Feinberg JR, Capello WN, Morphological features of the acetabulum and femur: anteversion angle and implant positioningClin Orthop Relat Res 2001 393:52-65. [Google Scholar]
[10]. Unnanuntana A, Toogood P, Hart D, Cooperman D, Grant RE, Evaluation of proximal femur geometry using digital photographsJ Orthop Res 2010 28(11):1399-404. [Google Scholar]
[11]. Kate BR, The angle of femoral neck in IndiansEastern Anthropologist 1967 20:54-60. [Google Scholar]
[12]. Saikia KC, Bhuyan SK, Rongphas R, Anthropometric study of the hip joint in North-eastern region population with computed tomography scanIndian J Orthop 2008 42:260-66. [Google Scholar]
[13]. Charnley J, Total hip replacement by low-friction arthroplastyClin Orthop Relat Res 1970 72:7-21. [Google Scholar]
[14]. Rubin PJ, Leyuraz PF, Aubaniac JM, Argenson JN, Esteve P, Roguin B, The morphology of the proximal femur. A three dimensional Radiographic analysisJ Bone Joint Surg[Br] 1992 74-B:28-32. [Google Scholar]
[15]. Deshmukh TR, Kuthe AM, Thakre S.B, Prediction of femur bone geometry using Anthropometric Data of Indian population:A numerical approachJ Med Sci 2010 10(1):12-18.15. [Google Scholar]
[16]. Kostamo T, Bourne RB, Whittaker JP, No difference in gender –specific hip replacement outcomesClin Orthop Relat Res 2009 467:135-40. [Google Scholar]
[17]. Rawal BR, Ribeiro R, Malhotra R, Bhatnagar N, Anthropometric measurements to design best fit femoral stem for Indian populationIndian J Orthop 2012 46(1):46-53. [Google Scholar]
[18]. Husmann O, Rubin PJ, Leyvraz PF, Roguin B, Argenson JN, Three dimensional morphology of the proximal femurJ Arthroplasty 1987 12:444-50. [Google Scholar]
[19]. Mahaisavariya B, Sitthiseripratip K, Tongdee T, Bohez EL, Sloten JV, Oris P, Morphological Study of proximal femur:A new method of geometrical assessment using 3 dimensional reverse engineeringMed Engg Phys 2002 24:617-22. [Google Scholar]
[20]. Siwach RC, Dahiya S, Anthropometric Study of proximal femur geometry and it’s clinical applicationIndian J Orthop 2003 37:247-51. [Google Scholar]