Blood pressure means the force exerted by the column of blood against any unit area of blood vessel [1]. Normally, in a young adult blood pressure is 120/70 mmHg in the sitting position [2]. Physiologically, blood pressure varies from moment to moment e.g. emotions, exercise, sleep, meals etc. Generally, blood pressure increases with advancing age. Blood pressure above 140/90 mm Hg measured on three separate occasions is termed as Hypertension [3].
An early and a regular screening to detect underlying hypertension is necessary to prevent any future complications [4]. Prevalence of hypertension is increasing rapidly among Indians. Rapid urbanization, sedentary life style, junk food and stress are the powerful environmental risk factors for increasing prevalence of hypertension, especially in younger age group [3]. Hypertension is a major risk factor for cardiovascular diseases like myocardial infarction, stroke. Hypertension is a controllable disease, early diagnosis and control can prevent 300,000 of 1.5 million deaths from cardiovascular diseases in india [5]. Lifestyle modifications like increased physical activity, salt restriction and weight reduction are effective for prevention and treatment of hypertension [6]. Exercise being the integral component of therapy [7]. Regular exercise has been shown to be effective in reducing the risks of hypertension. It is an important intervention to prevent and treat hypertension [8].
Over the years, there is much emphasis on the benefits of dynamic exercises. Static exercises were recognized as an important component of a fitness program only in 1990 by the American College of Sports Medicine (ACSM)[9]. It was suggested by ACSM that appropriately prescribed and well supervised static exercises have favourable effects on cardiovascular functioning, psychosocial well-being and endurance even though physiological mechanisms are different in both types of exercises for the improvement in cardiovascular function [10]. Isometric or Static exercise involves the contraction of skeletal muscle without a change in muscle length e.g. lifting or pushing heavy weights and contracting muscles against fixed objects in contrast to isotonic or dynamic exercise in which contraction of the skeletal muscle causes change in the length of muscle like running, swimming [11]. Isometric exercise may be of value in maintaining the desired blood pressure in individuals with inability or unwillingness to do isotonic exercises [12] .It has been shown that hypertension causes endothelial dysfunction causing less endothelial dependent, nitric oxide-mediated vasodilatation Isometric handgrip training improves endothelial dysfunction by shear-stress mediated improved bioavailability of nitric oxide and increased antioxidant activity [13]. It has been shown that there is decrease in muscle sympathetic nerve activity with exercise training [14]. Regular exercise training also increases cardiovascular capacity and decreases myocardial oxygen demand [15]. This would scientifically study explain the mechanism of cardiovascular fitness of people lifting weights in the gymnasium and other athletes doing static exercises. The studied is designed to study the effect of isometric exercise training on blood pressure in normal healthy adults.
Materials and Methods
A total of 30 normal healthy volunteers in the age group of 20-40 years were enrolled for the study. Hand grip spring dynamometer was used for IHG exercise training. It consists of two handles, connected through a flexible metallic strip. A graduated pressure scale is provided for estimation of compression force (INCO, AMBALA, INDIA) [Table/Fig-1].
Hand grip spring dynamometer

Exercise training protocol consisted of five 3-min bouts of IHG exercise at 30% of maximum voluntary contraction separated by 5 min rest periods. Exercise was performed 3 times/wk for 10 wk. Blood pressure was measured with a mercury sphygmomanometer by the auscultatory method in the sitting position before and after exercise.
Inclusion criteria: Normal healthy volunteers in the age group of 20-40 y.
Exclusion criteria: Persons suffering from hypertension, smokers, on medication or having any acute or chronic illness were excluded from the study. Volunteers with normal blood pressure not suffering from any acute or chronic illness not taking any medication who were non smokers were included in the study.
Procedure
The resting blood pressure was measured in sitting position.
The subject was asked to hold the dynamometer in the dominant hand so as to have a full grip of it. Handle of the dynamometer was compressed with maximum effort for a brief duration of 4-5 s and isometric contraction was recorded. Three attempts were given with a pause of 10 s between each attempt to prevent fatigue. Mean of these three readings was taken as maximal isometric tension (Tmax). After a rest of 5 min, the subject was asked to perform the isometric contraction at 30% of Tmax for a maximum of 3 min. The step 3 was repeated for five times with rest of 5 min after each bout of contraction.
The blood pressure was measured after a rest of 5 min.
This exercise protocol was repeated 3 times/wk for 10 wk.
Blood pressure of rest week was compared with the blood pressure after exercise training of 10 wk.
Statistical Analysis
Data is reported as mean + SD. Paired t-test was used for comparison of systolic and diastolic blood pressures from rest week to week 10. P-value of 0.05 was taken as significant. Statistical analysis was performed with SPSS version 17.0 software.
Results
Basal parameters are depicted in [Table/Fig-2].The mean (+SD) age of the sample studied was 29.8+6.29 y and consisted of 16 men and 14 women. The mean (+SD) height and weight of the sample studied was 162.33+8.86 cms and 61.33+6.31 kgs respectively. Mean BMI was 23.27 +7.3 kg/m2, signifying subjects were normal and not overweight.
Depicts anthropometric parameters in normal healthy volunteers
| Variables | Mean±SD |
|---|
| Age(yrs) | 29.8±6.29 |
| Sex(M/F) | 16/14 |
| Height(cms) | 162.33±8.86 |
| Weight(kgs) | 61.33±6.31 |
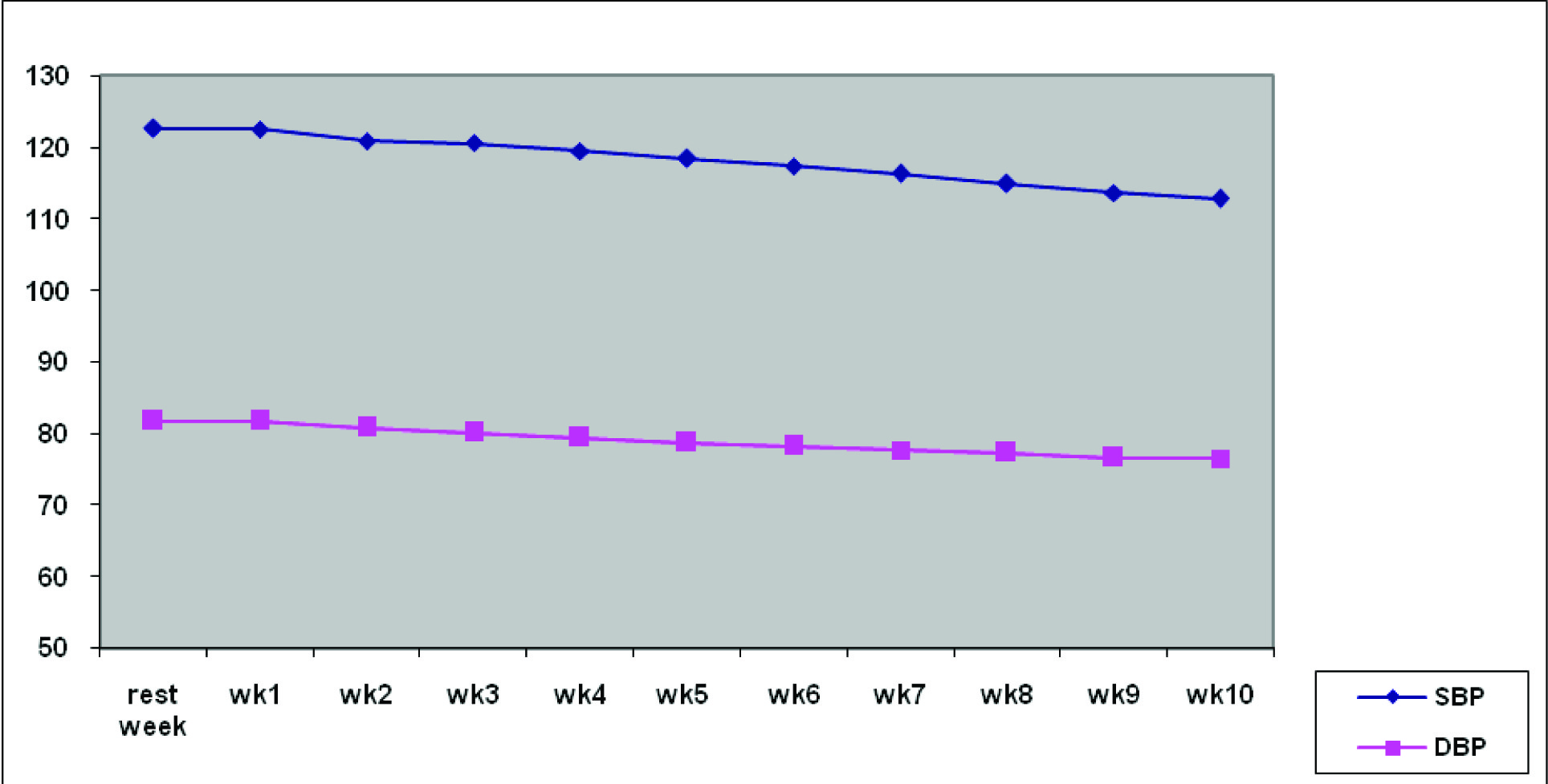
Though intermediate readings were taken, no significant effect was seen in an exercise less than 10 wk.
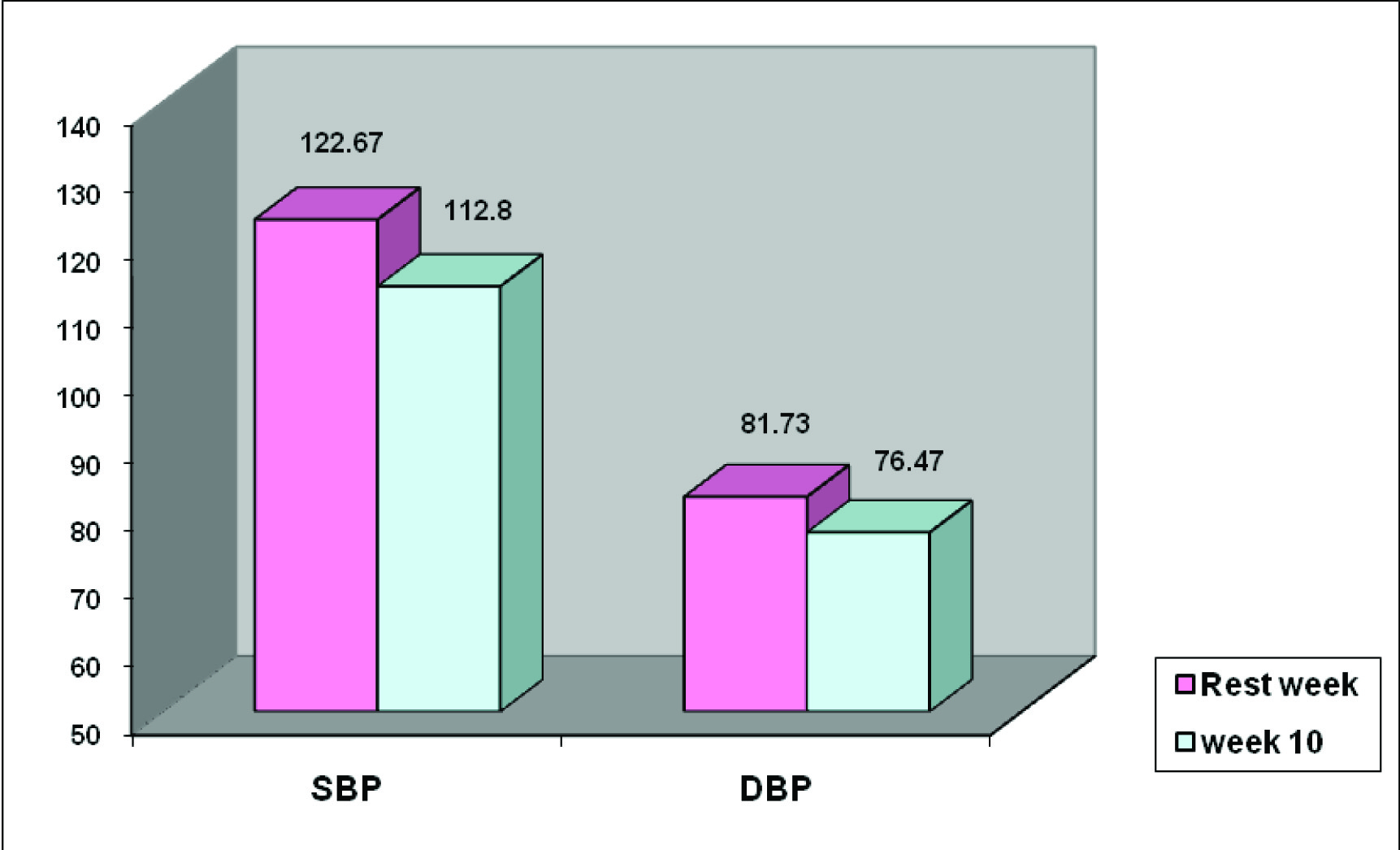
[Table/Fig-3,4] shows the comparison of systolic (SBP) and diastolic blood pressure (DBP) at rest wk and 10 wk after exercise. Both SBP and DBP were found to be significantly lower (p<0.001, p<0.001). 10 wk after exercise as compared to rest wk.
Bar diagram showing mean of SBP and DBP at rest week and 10 weeks
Graph showing decrease in SBP and DBP from rest week to 10 weeks
Discussion
Our study showed that there is decrease in resting blood pressure with IHG exercise training for a period of 10 weeks in normal healthy volunteers. Systolic blood pressure reduced from 122.67±2.31 mm Hg in the rest week to 112.8±1.86 mmHg after 10 wk (p<0.001), statistically highly significant. Diastolic blood pressure reduced from 81.73 ± 2.66 mmHg in the rest wk to 76.47 ±3.00 mmHg after 10 wk (p<0.001), statistically highly significant.
Results of the present study were similar to that of Wiley et al., [16] who reported significant reduction in blood pressure after a isometric exercise training of 8 wk. Significant reductions in systolic blood pressure (122 ±3 mmHg to 112±3 mm Hg, p<0.001) and diastolic blood pressure (70±1mmHg to 67± mm Hg, p<0.05) over the training period of 8 wk were also reported by Millar et al., [17].Our results are partially similar to that of Devereux et al., [18] who showed significant reduction in resting systolic blood pressure (4.9 ± 5.8 mmHg) and diastolic blood pressure (2.8 ± 2.4mmHg), but exercise protocol consisted of bilateral-leg isometric training for a period of 4 wk.
Following 8 wk, IHG participants demonstrated significant reductions in resting blood pressure. Systolic and diastolic blood pressures were reduced from 122 ± 3 mm Hg to 112 ± 3 mm Hg (p < .001) and from 70 ± 1 mm Hg to 67 ± 1 mm Hg (p < .05), respectively. Hierarchical linear modeling analysis also revealed a significant cross-level (i.e., group ÷ time) interaction, with an estimated reduction in systolic blood pressure of 5.4 mm Hg (p < .001) over the training period in the IHG group [19].
Hierarchical linear modeling analysis revealed a linear pattern of blood pressure decline over time with estimated reductions of 5.7 and 3 mmHg reductions in systolic and diastolic pressure, respectively in 43 hypertensive participants who performed the IHG test similar to our protocol. Participants with higher initial systolic pressure showed greater rates of blood pressure decline (r=−0.67), inferring that individuals with higher blood pressure stand to achieve greater benefits from this method of training [20].
Eighty-one men and women (42 exercise and 39 control) from three of 287 reviewed studies were pooled for analysis. Using random-effects models, statistically significant exercise minus control group reductions of approximately 10% were observed for both resting SBP and DBP (SBP: Xd, -13.4 mmHg; and DBP: X, -7.8 mmHg). Results were also statistically significant when fixed-effects models were used (SBP: X, -13.8 mmHg; 95% BCI, -15.3 to -11.0 mmHg and DBP: X , -6.1 mmHg; 95% BCI, -16.5 to -3.2 mmHg) [21].
Normally during exercise, there is increase in the concentrations of metabolites like lactic acid and adenosine that are detected by metabolite-sensitive nerve endings within the skeletal muscle interstitium. These substances increase the discharge of group IV(metaboreceptor) afferent fibers, initiating a potent reflex that increases sympathetic nerve activity. This leads to vasoconstriction, which contributes to the rise in BP. This is the mechanism postulated for immediate effect of exercise, which we saw in acute readings taken immediately after the manoeuvre. Regular exercise however, decreased blood pressure, as seen in the results after ten weeks. The postulated mechanism can be explained by Mostoufi- Moab S et al., who proved that [22] with regular exercise training, there is increased capillary density, increased mitochondrial density, activation of oxidative enzymes, and increased O2 extraction in the skeletal muscle .Increased vascular flow, along with an increased ability of trained muscle to maintain aerobic metabolism, lowers interstitial concentrations of metabolites, causing less stimulation of metaboreceptors, thereby evoking a smaller sympathetic response, causing less rise of blood pressure. Thus, regular isometric exercise training reduces the risk of development of hypertension in future.
Various authors have shown that during isometric training, chemoreceptor reflex responsible for sympathetic nerve activity is reduced and thus causing attenuation of sympathetic nerve response to sympathetic nerve activity which is responsible for decrease in resting blood pressure over a period of time [23].
It has been shown that exercise training improves local, endothelium dependent vasodilation in medicated hypertensives [11]. It was found that the incidence of hypertension was lower in individuals engaged in occupations that had component of isometric effort [24].
Limitations of Our Study
Sample size of our study is less. We have not measured NO level in blood to understand the mechanism of action of decrease in BP in IHG participants. Future studies on hypertensive participants are needed to analyse the therapeutic application of our study.
Conclusion and Future aspects of the study: IHG exercise training might be a simple, cost-effective and non-pharmacological method in lowering blood pressure. Further studies are needed.