Masticatory performance is cumulative contribution of various factors like bite force, severity of malocclusion, occlusal contact areas, body loss of teeth, restorations from molars to canine, facial forms and other motor activities, out of which biting force is one of the key factors [1,2].
The bite force measurements can be recorded directly by using a suitable transducer which is a convenient way of assessing the maximum voluntary bite force. Another method to record bite force is indirect evaluation by means of electromyography. It has been observed in various investigations that there is a linear relationship between direct force measurement and electromyographic activity potential [3,4].
Various anatomical and physiologic factors have been listed in literature which influences direct measurement of bite force [4]. Bite force measurement has been reported back in 17th century. With the development of various electronic equipments in 20th century, bite force is evaluated with more precision and accuracy. Determining the patient’s facial form in treatment planning helps the prosthodontist to achieve better clinical outcome. Further, if a relationship between the patient’s facial form and bite force can be established it can help in better patient education and prognosis of the treatment.
Evaluation of maximum bite force relative to facial morphology in natural dentition has been studied [5,6]. However, no study has yet been done to evaluate the variations of bite force in different facial forms in complete denture patients and its comparison to natural dentition. The following study highlights the variations of bite force in dentulous and edentulous subjects and the effect of various facial forms on it.
Materials and Methods
Source of data
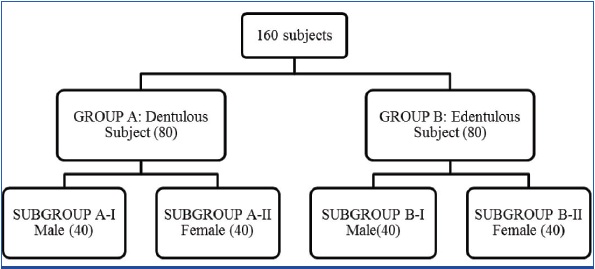
Eighty dentulous subjects (40 male & 40 female) aged between 20- 25 yrs were randomly selected from the students studying in Pacific dental college, Udaipur, India. Eighty edentulous subjects (40 male & 40 female) aged between 50-70 years who had receive complete denture in the Department of Prosthodontics, Pacific dental college in between January 2011 to December 2012 [Table/Fig-1].
Inclusion Criteria
For Dentulous subject
Presence of complete permanent dentition.
All participants were required to have Angle’s class I molar relationship.
For Edentulous subject
All the patients having class I ridge relationship, who received their complete denture within eight months of the total extraction.
Absence of any temporomandibular joint dysfunction or any documented systemic disease.
Exclusion criteria
Patients with systemic disease.
Patients with facial asymmetry.
Patients on drug therapy.
Any form of tobacco user.
Pregnant/lactating mothers.
The nature and design of the clinical study was explained to all 160 subjects (both dentulous and edentulous) and an informed consent was obtained for their participation. Once the subjects fulfilled the inclusion criteria, their bite force measurements [Table/Fig-2] were recorded. A 2mm thick thermoplastic sheet was used to protect the teeth from getting damaged while applying bite pressure and it was further covered by gloves to protect it from saliva contamination. The device was positioned between the most distal maxillary and mandibular molars (for dentulous subject), [Table/Fig-3] and between the second premolars and first molar (for edentulous subject) [Table/Fig-4]. At the time of denture insertion in edentulous patient bite force were recorded for both right and the left side. The maximum value on the display was recorded [Table/Fig-5,6]. This was repeated for 2-3 times till the subjects get familiar to the device. Then the value was finally documented and the mean of right and left side maximum bite force value was accepted for the statistical analysis.
Bite force measuring device,

Bite force measurement in dentulous subject,

Bite force measurement in edentulous subject

Maximum voluntary bite force recorded in dentulous subject

Maximum voluntary bite force recorded in edentulous subject

Bite Force was recorded using a Process Indicator 3016 [Table/Fig-2]. This weighing Indicator model-SMIT-3016 is based on the popular 8-bit micro controller. It is generally used for measuring and displaying the Weight in Industrial Systems. The System gives Excitation Voltage to Load Cell and reads mV output from the Load cell. The Weight Indicator converts it into Weight and displays the value. The system has a Six-digit 7-segment red LED display. It has 4-key keypad organized in 4 x 1 matrices. The device is designed to measure the bite force values in kilogram force which is the gravitational metric unit of force. Sensitivity of the device is 0.01 kg of force.
After the measurement of bite force, 160 subjects were divided into groups of 80 dentulous and 80 edentulous subjects. These groups were further divided into subgroups according to the gender [Table/Fig-1].
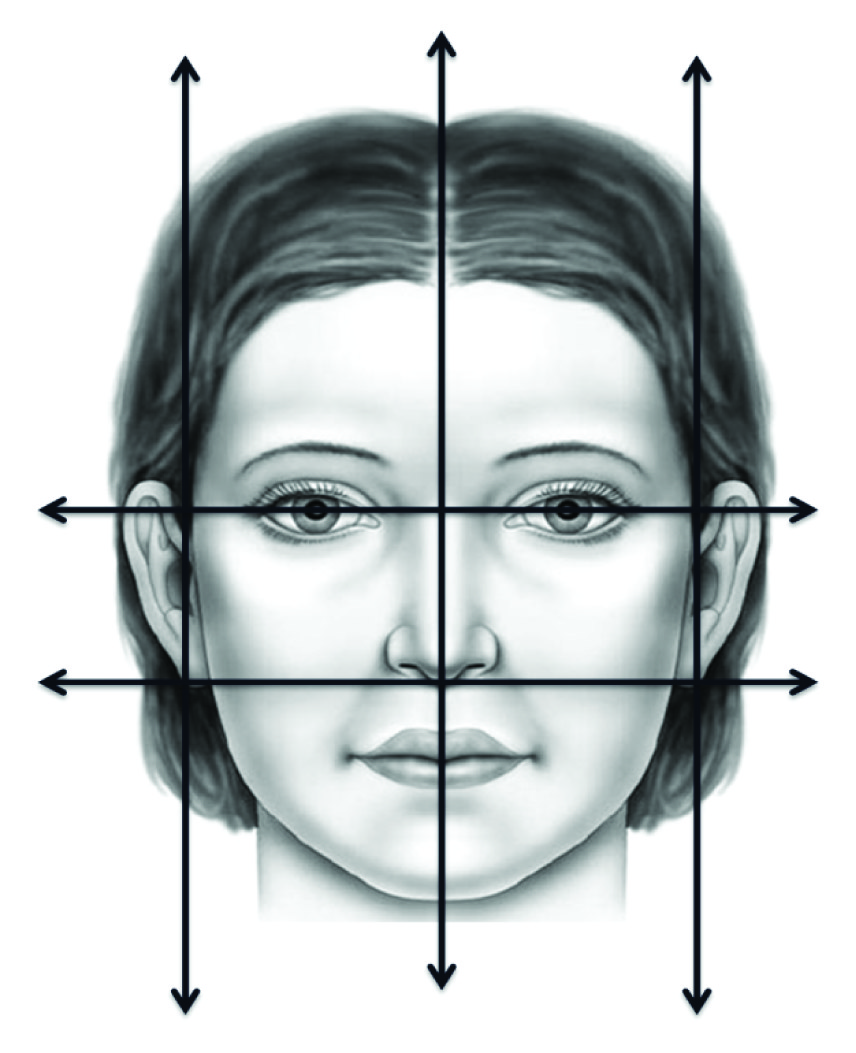
Bite force of the every subject was recorded followed by facial form evaluation using digital images. All images were taken by one camera (L-120 Coolpix Nikon) and from one individual from a distance of 1m with flash and lens pointing towards the nose and perpendicular to the subject’s face who sat upright with natural head position. Image was analysed by single individual in Adobe Photoshop CC to correct any deviation of the face. Vertical lines were marked and horizontal lines was placed one in supraorbital ridge and one at the base of nose perpendicular to facial midline, which divided the face in three parts. Then the facial form was evaluated based on the relation between facial outline and vertical line [Table/Fig-7]. Square facial forms have facial outline almost parallel to the vertical guide lines. The square-tapering facial form have facial outline tapering inward from middle third of the face. The tapering face form have facial outline tapering inward from upper third of the face. The oval face form was determined by a curved facial outline against the vertical guide lines.
Horizontal and vertiacl lines drawn to determine the facial form
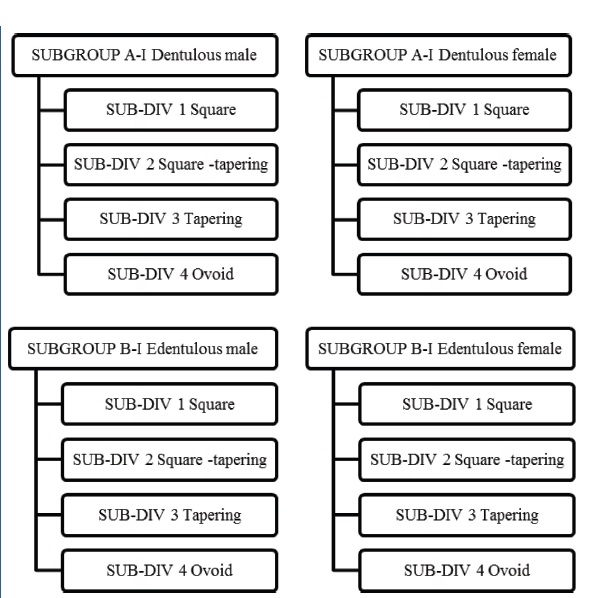
After determining the facial form of all the subjects, each subgroup was further divided into four subdivisions according to the Square, Square-tapering, Tapering, Ovoid types of facial forms in the following manner: as shown in [Table/Fig-8].
Distribution into subdivision
Finally the data was tabulated and transferred to a spread sheet which was subsequently converted into a SPSS format file to be analysed and evaluated using SPSS version 15.
Result
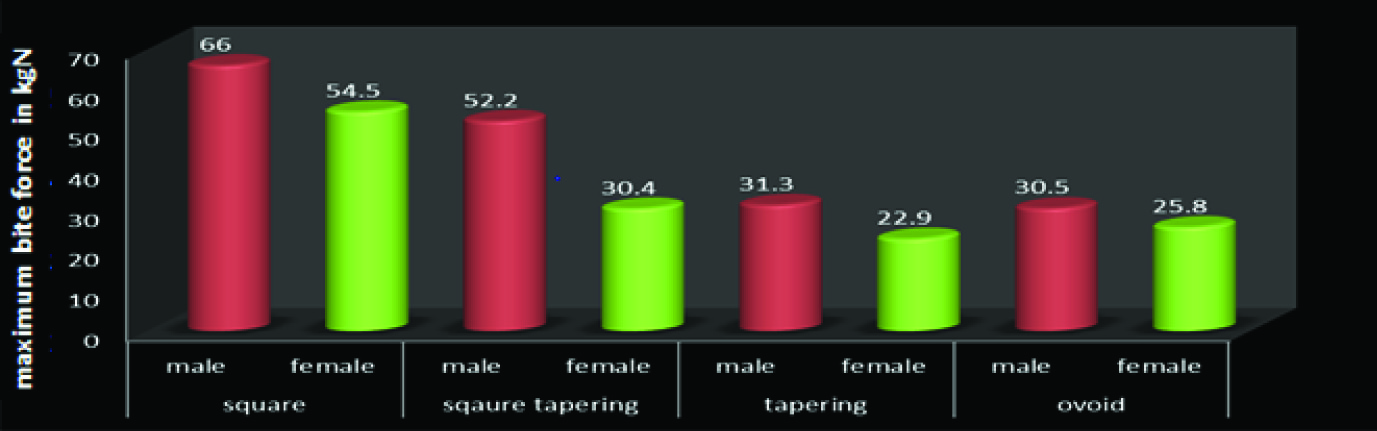
Mean value of maximum bite force of dentulous (male and female) and edentulous (male and female) according to their facial form are tabulated and summarized in [Table/Fig-9,10] respectively.
Mean value of maximum bite force of dentulous
Mean value of maximum bite force of edentulous
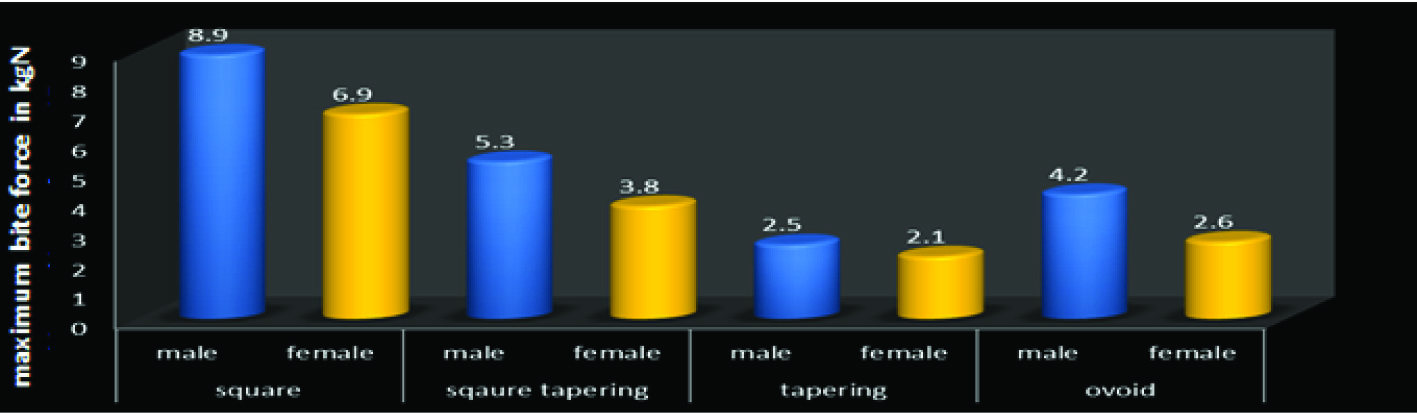
After the analysis of the bite force of all the subjects, mean with standard deviation based on the readings obtained were evaluated and comparisons were made. ANOVA Test was applied to the mean value to evaluate the comparison between and within the groups and the results was found to be highly significant. Further, Scheffe Test was applied and it revealed that maximum bite force difference was highly significant when compared between square facial forms and other facial forms in all the groups.
It was interesting to find that bite force variation according to facial form was significantly evident not only in the dentulous but also in the edentulous group. Square facial form subjects had relatively higher biting force than other facial forms in both the groups.
Further comparative assessment of maximum bite force between various groups is as follows:
For Dentulous and edentulous subjects, Independent sample t-test, [Table/Fig-11] revealed that bite force of dentulous subject was greater than edentulous patients and the result was statistically highly significant (p≤0.001).
For Dentulous male and female subjects, [Table/Fig-12] Independent sample t-Test was applied and result revealed that maximum bite force of males was greater than females and the result was statistically significant (p≤0.05).
For Edentulous male and female [Table/Fig-13] subjects, Independent sample t-Test was applied and results revealed that maximum bite force of male patients was greater than female patients and the result was statistically significant (p≤0.05).
Comparison of maximum bite force in dentulous and edentulous>
| Group | N | Mean(in KgN) | Std. Deviation | p-value |
|---|
| Dentulous | 80 | 44.7775 | 15.20345 | 0.001* |
| Edentulous | 80 | 5.1475 | 2.63049 | |
Comparison of maximum bite force in dentulous males and females
| Group | N | Mean(in KgN) | Std. Deviation | p-value |
|---|
| Male | 40 | 44.7775 | 15.20345 | 0.022* |
| Female | 40 | 32.0450 | 12.36222 | |
Comparison of maximum bite force in edentulous males and females
| Group | N | Mean(in KgN) | Std. Deviation | p-value |
|---|
| Male | 40 | 5.1475 | 2.63049 | 0.038* |
| Female | 40 | 3.7275 | 1.85472 | |
Discussion
Success of any dental treatment primarily depends upon thorough knowledge of masticatory system. Masticatory performance is influenced by several factors like loss and/or restoration of posterior teeth, bite force, malocclusion, body size, facial form, occlusal contact area, and other motor activities.
Duygu Koc [2] stated that bite force is one of the important indicator of the functional state of stomatognathic system. Determination of bite force of the patient before planning the prosthetic treatment can enhance the clinical outcome of the treatment.
With the advancement in age the bite force gradually decreases, because of gradual loss of dental component. Edentulous individuals are orally handicapped when compared to dentulous individual; even with the well fabricated complete denture they have reduced capacity to perform various masticatory functions.
Most studies concluded that denture wearers have only about one fifth to one fourth the bite strength and masticatory force in comparison to the natural dentition subjects. In edentulous patient, there are many factors that influence the magnitude of the biting force of an individual such as the anteroposterior inclination of the occlusal plane on biting force [7], effect of altering the vertical dimension of occlusion on biting force [8,9], type of teeth used and occlusion pattern [10].
The present study aimed to evaluate the variations of bite force in dentulous and edentulous subjects according to different facial forms. Following this, further comparisons were made between the variations in dentulous and edentulous subjects.
In this study, the maximum bite force was evaluated for 160 subjects (80 dentulous, 80 edentulous) using unilateral bite force measuring device. It has been stated in the study conducted by Van der Bilt [4], that there is no significant difference between unilateral and bilateral bite force measurements. The method used for this particular study to measure the bite force was the direct method where in bite force process indicator is placed between the predesignated areas.
Earlier studies have proved that the direct method of measuring bite force is more convenient and accurate when compared to indirect evaluation of the bite force measurement by employing electromyography test for Masseter and Temporalis muscle [2,10,11,12] which are be functionally related to the force production.
After the analysis of the bite force of all the subjects, mean values and standard deviation values obtained were evaluated and comparisons were made. ANOVA Test was applied on the mean to evaluate the comparison between and within the groups and comparison results were found to be highly significant. Further, Scheffe Test was applied and it revealed that maximum bite force difference was highly significant in square facial form than other facial forms in all the groups.
The result revealed that square facial form subjects of all the groups had greater maximum bite force than other facial forms. As the ramus become more vertical and gonial angle acute, elevator muscle exhibit greater mechanical advantage because of which the square facial form individual exhibit remarkably higher biting force. There was no significant difference between square-tapering, tapering and ovoid facial forms, which can be explained by the fact that in all these groups lower part of the face is converging unlike square facial form.
It was interesting to find that bite force variation according to facial forms was significantly evident not only in the dentulous but also in the edentulous group. Square facial form subjects had much higher biting force than other facial forms in both the groups.
Comparison of maximum bite force between dentulous and edentulous groups using Independent Sample t-Test, revealed significant result due to the loss of dental component and ageing which markedly reduces the biting force by 1/5th to 1/10th of the bite force seen in younger individuals with the natural teeth. Due to loss in dental component there is loss in periodontal support. It is been documented earlier that biting force induced by elevator muscles are mainly influenced by the mechanoreceptors in periodontal ligament. Slagter [13] have stated earlier that people with loss of attachment have shown impaired sensory function resulting in reduced control of biting force.
In many previous studies, bite force has been higher in males. In order to evaluate this finding, equal male and female subjects were included in this study for both dentulous and edentulous groups. Mean with standard deviation was evaluated and the Independent Sample t-Test was applied. The result proved that male subjects had significantly higher bite force than females both in dentulous and edentulous groups. The difference obtained was higher in this study when compared to the results of previous studies [1,2,6] Higher biting force in male is attributed by greater muscular potential because of anatomic variation. Also, males have type-II fibers in masseter muscle, which have larger diameter. Dental component of males is also larger than in females which in turn increases the periodontal support further contributing to increased biting force [14].
It was concluded that higher bite force is expected in square facial form individual in comparison to other face forms. Result also proved without doubt that patients with complete denture with any facial form have much lower mean maximum bite force when compared to dentate subjects.
Conclusion
From the results obtained, and within the limitations of the study, the following conclusions could be drawn:-
Dentulous as well as edentulous subject with square facial form have higher maximum mean bite force in comparison to square-tapering, tapering and ovoid types of facial forms and the difference found is highly significant(p ≤ 0.001). The possible reason for this is that the ramus is more vertical and the gonial angle is more acute in square shaped faces, hence the elevator muscle exhibits greater mechanical advantage.
Maximum mean bite force in dentulous subjects was remarkably higher than in edentulous subject and the result was statistically highly significant (p ≤ 0.001). This may be due to the loss of dental component and ageing which remarkably reduces the bite force.
On comparison of maximum mean bite force between dentulous male and female subjects and between edentulous male and female subjects revealed that male subjects had higher maximum mean bite force than females in both the groups and the result was statistically significant (p<0.05). This result may be attributed because of the greater muscle potential of the male patients.