Dental protrusion is common in many ethnic groups around the world. It is characterized by dentoalveolar flaring of maxillary or both the maxillary and the mandibular anterior teeth with resultant protrusion of the lips and the convexity of the face. The present trend to treat protrusion is by extracting all the first premolars, followed by anterior tooth retraction to obtain the desired dental and soft-tissue profile changes [1].
Anchorage is a critical component in anterior en-masse retraction. Strategies for anchorage control have been a major factor in achieving successful orthodontic treatment since the specialty began [2]. There are situations where absolute anchorage is needed, however as Newton’s Third Law states for every action there is an equal and opposite reaction [3], failure to maintain the position of the anchorage units leads to ‘anchor loss’, which results in incomplete achievement of anterior retraction [4].
Reinforcement of anchorage can be done by including as many teeth as possible to the anchor unit [5]. Other methods of reinforcing anchorage are: use of Interarch elastics, Transpalatal arch, Nance holding appliance, headgear with one pound pressure per side or at least 128gm on each side for 16-18 hours every day [6,7], muscular forces, cortical anchorage, use of torque, etc. However, all these methods have their inherent disadvantages like need for precise wire bending, need for patient co-operation and clinician’s time [6–8].
Orthodontic research has undergone an ocean of changes in the last 50 yrs. In order to elucidate mechanical changes taking place within a biological system numerous studies like photoelastic [10], strain gauge [11] and laser holographic [12] interference techniques have been attempted. While these approaches have provided some information in precise evaluation of displacement and stress induced in stomatognathic system, it would be impossible to carry them out without actual tissue damage in human beings.
The Finite Element Method (FEM), which was introduced as one of the numerical analyses has become an useful technique for stress and strain analysis in biological systems.
FEM has revolutionized dental biomechanical research. Basically, the object to be studied is graphically simulated in a computer, which defines the geometry of the body being studied. It is divided into a number of sub-units termed elements. These are connected at a finite number of points called nodes. The elements are prescribed the appropriate material properties of the structure they represent. What is achieved is a mathematical model of the likely physical response of that object to load; large volumes of information about stresses, strains, and displacements being obtained through the continuum defined [13].
FEM makes it possible to analytically apply various force systems at any point and in any direction and also quantitatively assess the distribution of such forces through the wire and related structures. Hence, this tool was chosen for the current study.
The aim of this study is to find if it is possible to control maxillary anterior teeth in sagittal and vertical plane during retraction by altering the vertical levels of force application in posterior region i.e. to identify the type of movement of maxillary anterior teeth which occurs when force is applied from four different levels i.e. High, Medium, Low pull Implants and from a conventional Molar hook and also to quantify the retraction and intrusion components of force during retraction with implants.
Materials and Methods
Construction of geometric model [Table/Fig-1,2]
[Table/Fig-1,2]
Construction of Geometric Model

Construction of Geometric Model

The geometric models of the maxillary central incisor, lateral incisor, canine, second premolar and first molar were constructed using the dimensions and morphology found in Wheeler’s text book [16]. First premolar was not constructed in order to simulate retraction in 1st premolar extraction cases. These teeth were then arranged in ovoid archform [17]. In order to establish mesio-distal angulations and labio-lingual inclination of the teeth, the maxillary dentition was arranged according to MBT norms [17].
In order to establish the natural anatomy, periodontal ligament (PDL) was constructed with an average thickness of 0.25mm around the roots of all the teeth. Next alveolar bone was constructed; PDL and the teeth were fitted into the bone.
Bracket with slot size 0.022” × 0.028” was made and attached to the crowns such that the Facial axis point was coinciding with the center of the bracket slot (base point and slot point).
Stainless steel arch wire of dimension 0.019” × 0.025” was designed with hook of 2mm between the lateral incisor and canine.
Conversion of geometric model to finite element model
Geometric model was converted into finite element model i.e. finite number of elements and nodes. 4-node tetrahedron elements were used.
The number of elements and nodes used are mentioned in [Table/Fig-3].
Number of elements and nodes in the FEM model
| Model | No. of Nodes | No. of Element |
|---|
| Maxillary Central Incisor | 2195 | 10413 |
| Maxillary Lateral Incisor | 1318 | 5742 |
| Maxillary Canine | 3098 | 14988 |
| Maxillary Second Premolar | 2059 | 9648 |
| Maxillary First Molar | 5613 | 27215 |
| PDL (of all teeth) | 5532 | 16771 |
| Alveolar bone | 21488 | 101896 |
| Brackets | 456 | 1222 |
| Arch wire/Hook | 43 | 42 |
| Complete model | 41802 | 187937 |
Material Property Data Representation
Teeth, PDL, alveolar bone, Brackets, arch wire were considered as isoparamertic and homogenous.
Brackets and archwire were given the properties of stainless steel.
The different structures involved in this study have a specific material property.
The material properties used in this study were derived from Chang et al.,[18] mentioned in [Table/Fig-4].
Material properties used in the FEM model
| Material | Young's modulus (kg/mm2) | Poisson's ratio |
|---|
| Tooth | 2.0 x 103 | 0.30 |
| PDL | 6.8 x 10-2 | 0.49 |
| Alveolar Bone | 1.4 x 103 | 0.30 |
| Bracket | 21.4 x 103 | 0.30 |
| Arch wire / Hook | 21.4 x 103 | 0.30 |
Defining the boundary condition
At the connected nodes between the archwire and the brackets, translational degrees of freedom in the two flexural directions of the archwire were coupled to deform together, and translational degrees of freedom in the axial direction of the archwire were unconstrained.
Therefore, free axial rotation movement of the archwire in the brackets was allowed, while friction between the archwire and brackets along the axial direction was ignored.
The boundary conditions were also defined to simulate how the model was constrained and to prevent it from free body motion. The nodes attached to the area of the outer surface of the bone were fixed in all directions to avoid free movement.
Application of forces
Anterior en-masse retraction was done with force vectors from four different levels i.e. from High pull implant [4] (13.5mm from archwire), medium pull implant [4] (9mm from archwire), low pull implant [4] (4.5mm from archwire) which were placed buccally between the roots of second premolar and first molar and from a conventional molar hook to the hook positioned between the brackets of the maxillary lateral incisor and canine on the archwire.
Here a force of 150gm/side was applied [1,6,14,19,20].
Coefficient of friction between the bracket slots and archwire was assumed to be 0.2 [21,22].
Evaluation of En-masse retraction
The analysis was carried out using software ANSYS11(Swanson Analysis System Inc., Canonsburg, Pennsylvania, USA) and movement was calculated.
Results were represented in Y and Z axis, where Y and Z axis represented movements in the sagittal and vertical plane respectively. Positive value indicated distal movement in Y axis and the upward movement in Z axis. The negative value indicated mesial movement in Y axis and downward movement in Z axis.
Results
Initial displacement of the teeth at the crown and root tip was calculated on Y and Z axis. All results were expressed in rad mentioned in [Table/Fig-5].
Recorded teeth displacements at crown and root tips in Y and Z axis from different levels of force application (All results are expressed in rad)
| Tooth | Position | Axis | From Molar Hook | At 4.5 mm | At 9 mm | At 13.5 mm |
|---|
| Central Incisor | Crown Tip | Y | .110E-03 | .106E-03 | .106E-03 | .103E-03 |
| Z | -.112E-06 | .108E-04 | .121E-04 | .138E-04 |
| Root Tip | Y | -.218E-04 | -.189E-04 | -.185E-04 | -.180E-04 |
| Lateral Incisor | Crown Tip | Y | .131E-03 | .129E-03 | .129E-03 | .125E-03 |
| Z | -.111E-06 | .110E-04 | .125E-04 | .145E-04 |
| Root Tip | Y | -.486E-04 | -.447E-04 | -.445E-04 | -.440E-04 |
| Canine | Crown Tip | Y | .108E-03 | .107E-03 | .107E-03 | .107E-03 |
| Z | -.097E-06 | .107E-04 | .119E-04 | .135E-04 |
| Root Tip | Y | -.826E-04 | -.234E-04 | -.230E-04 | -.225E-04 |
Displacement of teeth in Y axis [Table/Fig-6].
Displacement of teeth in Y axis (All results are expressed in rad)
| Tooth | Central Incisor | Lateral Incisor | Canine |
|---|
| Crown tip | Root tip | Crown tip | Root tip | Crown tip | Root tip |
|---|
| From Molar Hook | .110E-03 | -.218E-04 | .131E-03 | -.486E-04 | .108E-03 | -.826E-04 |
| At 4.5 mm | .106E-03 | -.189E-04 | .129E-03 | -.447E-04 | .107E-03 | -.234E-04 |
| At 9 mm | .106E-03 | -.185E-04 | .129E-03 | -.445E-04 | .107E-03 | -.230E-04 |
| At 13.5 mm | .103E-03 | -.180E-04 | .125E-03 | -.440E-04 | .107E-03 | -.225E-04 |
In sagittal plane when force was applied from
Molar hook: central incisor, lateral incisor and canine tipped lingually. Amount of tipping was more in canine and least in central incisor.
4.5mm implant: Here also tipping was seen, but the amount of tipping was less when compared to the retraction from the molar hook.
9mm and 13.5mm implant: Here also tipping was seen and the amount of tipping was almost same as that occurred from 4.5mm.
At all levels of force application tipping of central incisor, lateral incisor and canine occurred.
Displacement of teeth in Z axis [Table/Fig-7].
Displacement of teeth in Z axis (All results are expressed in rad)
| Central Incisor | Lateral Incisor | Canine |
|---|
| From Molar Hook | -.112E-06 | -.111E-06 | -.097E-06 |
| At 4.5 mm | .108E-04 | .110E-04 | .107E-04 |
| At 9mm | .121E-04 | 125E-04 | .119E-04 |
| At 13.5mm | .138E-04 | .145E-04 | .135E-04 |
In vertical plane when force was applied from
Molar hook: Extrusion of central incisor, lateral incisor and canine were seen.
4.5mm implant: Intrusion of central incisor, lateral incisor and canine were seen.
9mm implant: Here also intrusion was seen, but the amount of intrusion was more than that from 4.5mm implant height.
13.5mm implant: Here too, intrusion was seen, but the amount of intrusion was more than that from 9mm implant height.
Archwire deformation was seen downwards. Amount of distortion of the wire was almost same at all levels.
Discussion
Orthodontics has developed rapidly since the past few decades. Various facts about the subject has been discovered and new technologies are continuously being developed. One of the major challenge faced by the orthodontists is to understand and predict the complexities involved in the response of the teeth to the forces and the moments.
Many methods have been used to study the relationship between force systems and distribution of stress/strain on tooth and its surrounding tissues. Some of the methods are FEM, Laser holographic techniques, Mathematical models representing the in vivo situation and Photoelastic studies. Each of these techniques have inherent advantages and disadvantages.
The 3D FEM used in the present study provides the freedom to simulate orthodontic force applied clinically and to analyse the response of the dentition to the force in three-dimensional space. The point of force application, magnitude and direction of force may easily be varied to simulate the clinical situation.
Studies have shown that implants remain stable and thus serve as an absolute anchorage unit [1,23]. Therefore fixed nodes were used for force application.
Force of 150gms/side was used as it is within the physiologic limits for enmasse retraction as told by Rickets and others [1,6,14,19,20].
In this view a model of maxillary dentition was developed with defined material properties. The model was analyzed to calculate displacement, when force was applied from four different locations.
Displacement of teeth when force was applied from Molar hook [Table/Fig-8].
Displacement of teeth when force was applied from Molar hook
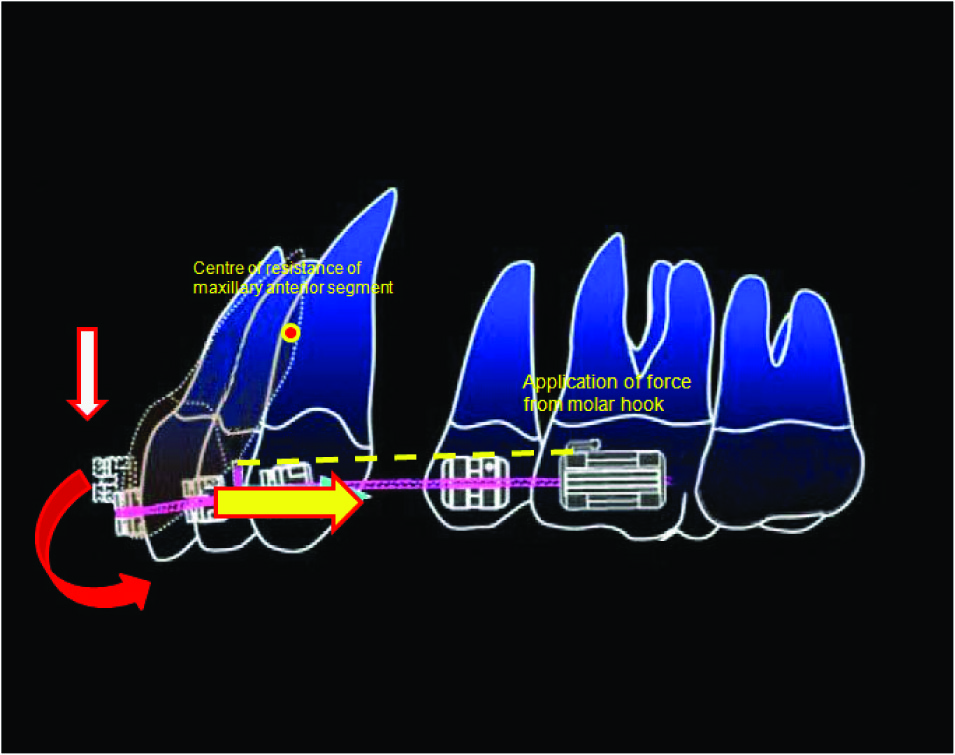
In Sagittal plane (Y axis) uncontrolled tipping of all the teeth was seen, central incisor, lateral incisor and canine tipped distally. Here tipping occurred because the point of force application was below the center of resistance. The center of resistance of the six anterior teeth was estimated to be halfway\between the center of resistance of the four incisors and canines(red dot in figure) [5,14,20] as told by Melsen, Hyo-Sang Park and others i.e. 13.5 mm apical and 14.0mm posterior to the incisal edge of the upper central incisor. These results correlated with the findings mentioned by Graber, where retraction with conventional methods of anchorage preservation noted anchorage loss with mesial tipping of molars [24].
In Vertical plane (Z axis) small amount of extrusion was seen. As the point of force application was under the center of resistance, extrusion of teeth has occurred.
Displacement of teeth when force was applied from Implant at 4.5mm from Archwire [Table/Fig-9].
Displacement of teeth when force was applied from 4.5mm, 9mm,13.5mm mini implant height

In Sagittal plane (Y axis) uncontrolled tipping of the central incisor, lateral incisor and canine was seen. Here tipping occurred because point of force application was below the center of resistance [5,25,26]. Here amount of tipping is less when compared to force from molar hook.
In Vertical plane (Z axis) intrusion was seen. Here intrusion occurred because of the vertical component of force.
When we resolve a force vector into horizontal and vertical components, horizontal force vector is responsible for retraction and vertical for intrusion. The angle formed between the horizontal and main force vector is called as Theta (θ). Horizontal force is equal to (cosθ x force) and vertical force is equal to (sin θ x force) [27,28].
At 4.5mm implant height θ is 10°. So cos10 = 0.9841and sin10 = 0.1771. So horizontal force is 0.9841x150 = 147628gms and vertical force is 0.1771x150= 26.57gms.
This finding correlated with studies done by Hyo-Sang Park, Madhur Upadhyay where along with a retraction, 2mm of intrusion was also seen [5,19].
Displacement of teeth when force was applied from Implant at 9mm from Archwire [Table/Fig-9].
Here tooth movement occurred almost similar to that which occurred when force was applied from 4.5mm implant level. But here the amount of intrusion is slightly more as the line of action was slightly nearer to center of resistance. The angle formed from the line of action to the horizontal component of force is increased when compared to 4.5mm implant level, as this angle increases intrusion component of the force also increases causing more intrusion [27].
Here θis 20°. Horizontal force is 0.9396x150 = 140.95gms and vertical force is 0.342x150 = 51.3gms.
Displacement of teeth when force was applied from Implant at 13.5mm from Archwire [Table/Fig-9].
Here tooth movement occurred almost similar to that which occurred when force was applied from 4.5mm and 9mm implant levels. But the amount of tipping was slightly less and the intrusion was slightly more when compared to the other two levels of implants. The probable reason for this is again the same.
Here θ is 28°. Horizontal force is 0.8829x150 = 132.44gms and vertical force is 0.4694x150 = 70.42gms.
When the force is applied from implants: A large and predominant retractive force and a smaller intrusive force will be acting, causing en-masse retraction and some intrusion of the anterior teeth. Additionally, there is a clockwise moment on the anterior segment as the total force passes below the estimated center of resistance of the anterior teeth [29].
Quantification
If we know the horizontal distance from implant to retraction hook and implant height we can find outθ angle by formulae tan-1(implant height divided by the horizontal distance from retraction hook to implant). Once we know the θ angle we can resolve the force applied into horizontal and vertical vectors and get retraction and intrusion component of forces.
If we consider approximately 25mm as the distance of implant from retraction hook, for every mm of implant placed apically θ angle increases by 2degrees so retraction component of force reduces approximately by around 1%, and intrusion component of force increases approximately by around 0.3%.
Conclusion
Based on the results of this study, we can reckon that changing the position of implant in vertical plane will have very little effect on the type of tooth movement.
How much ever higher we place the implants, force application in anterior region will always be below the centre of resistance, ergo there will be always tipping. As the point of force application moves apically amount of lingual tipping is slightly reduced and amount of intrusion is slightly increased.
For every mm of apical displacement of implant, the retraction component of force reduces approximately by around 1%, and intrusion component of force increases approximately by around 0.3%.
FEM has been widely used in engineering; however, its application to health sciences is relatively new, and because of the multiple variables in real life, certain approximations and assumptions are needed. Analytical results of FEM are highly dependent on the models developed; therefore they have to be constructed to be equivalent to real objects in various aspects. The results of this study were obtained from a simulated model, from which biologic variability’s may occur.
However, one should be aware that the structural and spatial relationships of various dentofacial components vary among the individuals. It is important to realize that these factors may contribute to varying responses of the dentofacial components on loading, thus affecting the locations of the center of resistance.
Other limitations of our study include approximations in the material behavior and shapes of the tissues. Similar to previous studies, the PDL was modeled as a layer of uniform thickness and was treated as linear elastic and isotropic, even though the PDL exhibits anisotropy and non linear viscoelastic behavior because of tissue fluid. There is no reliable and adequate data that pertain to anisotropic and nonlinear properties of the PDL.
The teeth were modeled as a uniform solid and the various dental tissues were not modeled. Similarly, bone was modeled only as a cancellous bone and cortical bone was not included. And also the factors which affect the real tooth movement in vivo include differences in mechanical features between models and biological tissues, cumulative tooth movements following bone resorption and deposition under stress and tension could not be included.
As this study calculated only the initial tooth displacement, one more point that should be noted is: as retraction progresses anterior teeth (hook) keeps coming nearer to the point of force application (implant), so force vector keeps on changing. As a result intrusion component of force will be more in final stages of space closure. In case of retraction with molar hook, throughout the retraction procedure force vector will not change.
The further direction of FEM studies should involve the tissue reactions, more accurate simulation of loading and approximation of material behaviors as well as variations in geometries of PDL, bone and teeth in three-dimensional finite element analysis.