Oral Hygiene Practices and Dentition Status of Public Transport Workers of India- A Cross-sectional Study
Ramandeep Singh Gambhir1, Ramandeep Kaur Sohi2, Gurminder Singh3, Rajdeep Brar4, Harpreet Singh5, Heena Kakar6
1 Reader, Department of Public Health Dentistry, Gian Sagar Dental College and Hospital, Rajpura, Punjab, India.
2 Senior Lecturer, Department of Public Health Dentistry, Rayat and Bahra Dental College and Hospital, Mohali, Punjab, India.
3 Professor, Department of Prosthodonics, Gian Sagar Dental College and Hospital, Rajpura, Punjab, India.
4 Assistant Professor, Department of Oral Medicine and Radiology, Harvansh Singh Judge Dental College, Chandigar, India.
5 Associate Professor, Department of Conservative Dentistry and Endodontics, Gian Sagar Dental College and Hospital, Rajpura, Punjab, India.
6 Consultant, Community Dental Centre, Chandigarh, India.
NAME, ADDRESS, E-MAIL ID OF THE CORRESPONDING AUTHOR: Mr. Ramandeep Singh Gambhir, Reader, Gian Sagar Dental College, Rajpura, Punjab-140601, India. Phone : +91-99156-46007, Fax : +91-1762 520011, E-mail : raman1g@yahoo.co.in
Objectives: To evaluate the oral hygiene practices and dentition statuses of transport workers who were working in a public bus transport system (C.T.U.) of Chandigarh (U.T.), India.
Materials and Methods: The data were recorded on a modified W.H.O. format (1997). A total of 1008 subjects constituted the final sample size. Information was obtained regarding the oral hygiene practices and clinical examinations were conducted. Statistical analysis was done by using ANOVA and Z-test.
Results: The mean age of the subjects was 45.3 ± 7.8 years. Mean DMFT of the subjects who were not using tobacco in any form was 5.02. 80.2% (808). 88.7% of the subjects brushed their teeth as least once a day. Mean number of decayed and missing teeth were 1.67 ± 2.16 and 1.46 ± 2.8, respectively and their relation with age was found to be statistically significant.
Conclusion: Dental caries was found to be major indication in all the age groups. More elderly subjects than young needed extractions. This study emphasized the need of an improved dental awareness and availability of dental facilities to transport workers.
Dentition Status, Oral Hygiene Practices, Oral Health, Transport Workers
Introduction
Health continues to be a neglected entity despite continuous efforts which are being made for health promotions, worldwide. Health is often taken for granted, and its value is not fully understood, until it is lost [1]. Oral health is an integral part of general health and a valuable asset for any individual. The occupational environment is one of the major determinants for health. There are certain working classes who spend most of their time on wheels, travelling from one place to another, without regular food, rest, recreation and even sleep. These people work in odd climatic conditions, with frequent changes in their day and night shifts, which lead to changes in their schedules or life-styles, which are compounded by delays and breakdowns [2].
Chandigarh, a union territory, is the capital city of two states, Haryana and Punjab. Chandigarh has a great network of a local bus transport system which is known as Chandigarh Transport Undertaking (C.T.U.). C.T.U. has a total strength of 517 buses; 209 buses run on local/suburban routes and 208 buses run on interstate routes, with a staff strength of 2100 people at 3 bus depots. CTU’s staff ratio per bus is the lowest in the country: just 5.54 employees per bus as compared to those seen in Mumbai (10.99), Delhi (9.16), Calcutta (11.66) and Ahmedabad (10.33) [2].
Tooth loss is mainly attributed to dental caries and periodontal diseases, but psychosocial factors as well as age, gender, lifestyle (dietary habit, smoking, alcohol intake, etc.) and oral health behaviour may modify the progression of these disorders. 40-45% of the subjects in Chandigarh (35-44 years) reported oral health complaints in one year (2009). The adult population of Chandigarh (35-44 years) had a mean DMFT of 9.5, which was higher as compared to those seen in the other states of India. 20-25% of subjects (35-44 years) who lived in Chandigarh used to smoke tobacco in the form of bidis, followed by cigarettes and 33% of subjects used to consume alcohol [3,4].
In an era of evidence based medicine and oral health, scientifically testing fundamental concepts such as oral hygiene and dentition status among specific occupational people should be given highest research priority, as very few researches who deal with the prevalence of dental disorders have been carried out among Indian population, especially among subjects who belonged to specific occupational groups. Literature on the oral hygiene statuses of transport employees is almost non-existent. The aim of this paper was-
To gather information on the oral hygiene practices and dentition statuses of workers of Chandigarh Transport Undertaking (C.T.U.) buses, Chandigarh.
For planning specific programs which were aimed at improving the oral health statuses of this particular occupational group.
Materials and Methods
Recording and Diagnosis Criteria
The ‘WHO’ oral health proforma -1997 was used to record the demographic information and clinical findings [2]. The proforma was comprised of questions like age, gender, marital status, income, educational qualifications of the subjects and it also contained questions which pertained to oral hygiene practices of the study subjects, like frequency of brushing, any type of deleterious habits, cleansing aid which was used, etc. Dental examination was conducted in the bus depot by using additional artificial light. For the diagnosis of dental caries, a WHO type III examination was done by using mouth mirrors and sharp probes [3].
Statistical Analysis
The data were analyzed by using SPSS package, version 13.0. One-way analysis of variance (ANOVA) and Z-test were used to determine differences at a 5 percent significance level (p<0.05), whereas proportions were compared by using the Chi-square test. p-values of < 0.05 were considered to denote statistical significance.
Results
Mean age of subjects was 45.3± 7.8 years. Maximum numbers of subjects (45.3+1.3= 46.6) were present in 41-50 year age-group [Table/Fig-1]. A total of 97% (978) males and 3% (30) females were interviewed and examined.
Distribution of study population by age and gender

A majority of the subjects (55.4%, 558) were educated till high school, 12.6% (127) were graduates and 2.7% (27) were post graduates.
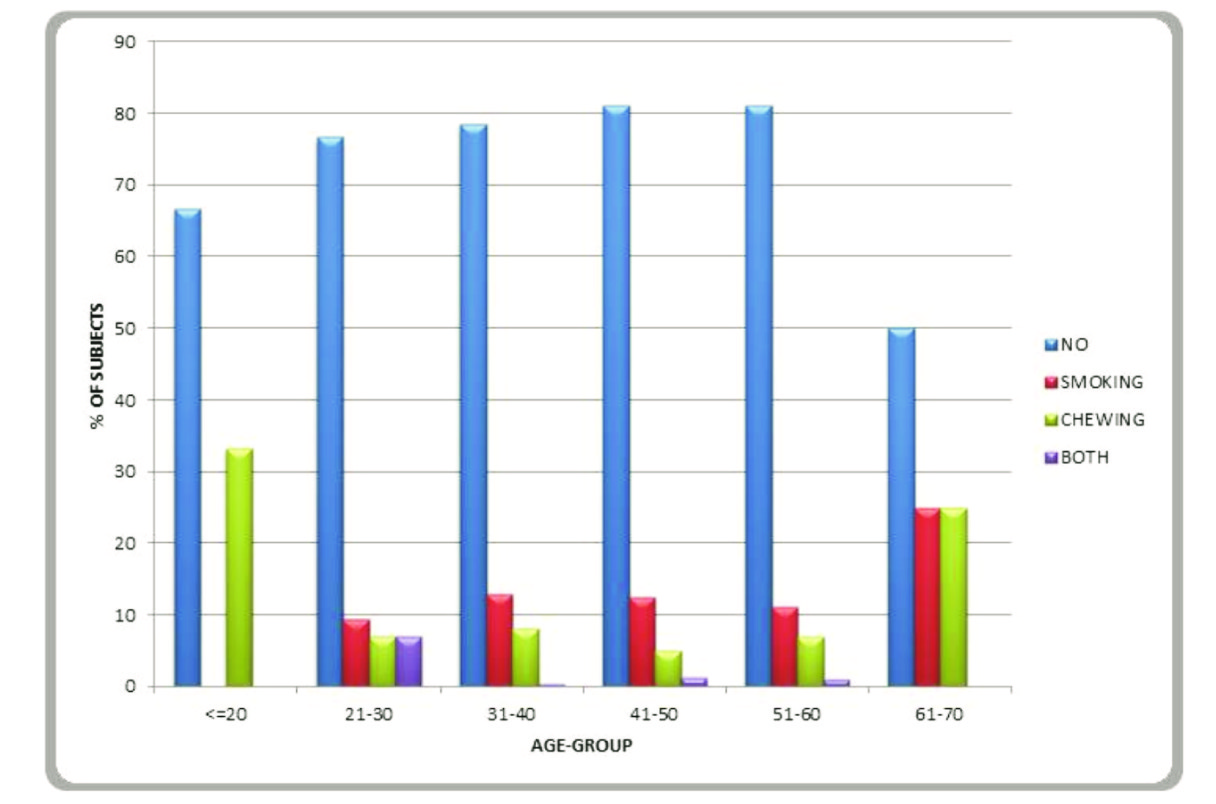
Tobacco consumption among the study subjects
80.2% (808) of the subjects were not consuming tobacco in any form. Maximum number of subjects who used to smoke and chew tobacco (12.5% and 5%) belonged to the age group of 41-50 years [Table/Fig-2].
Age wise tobacco habits of study population
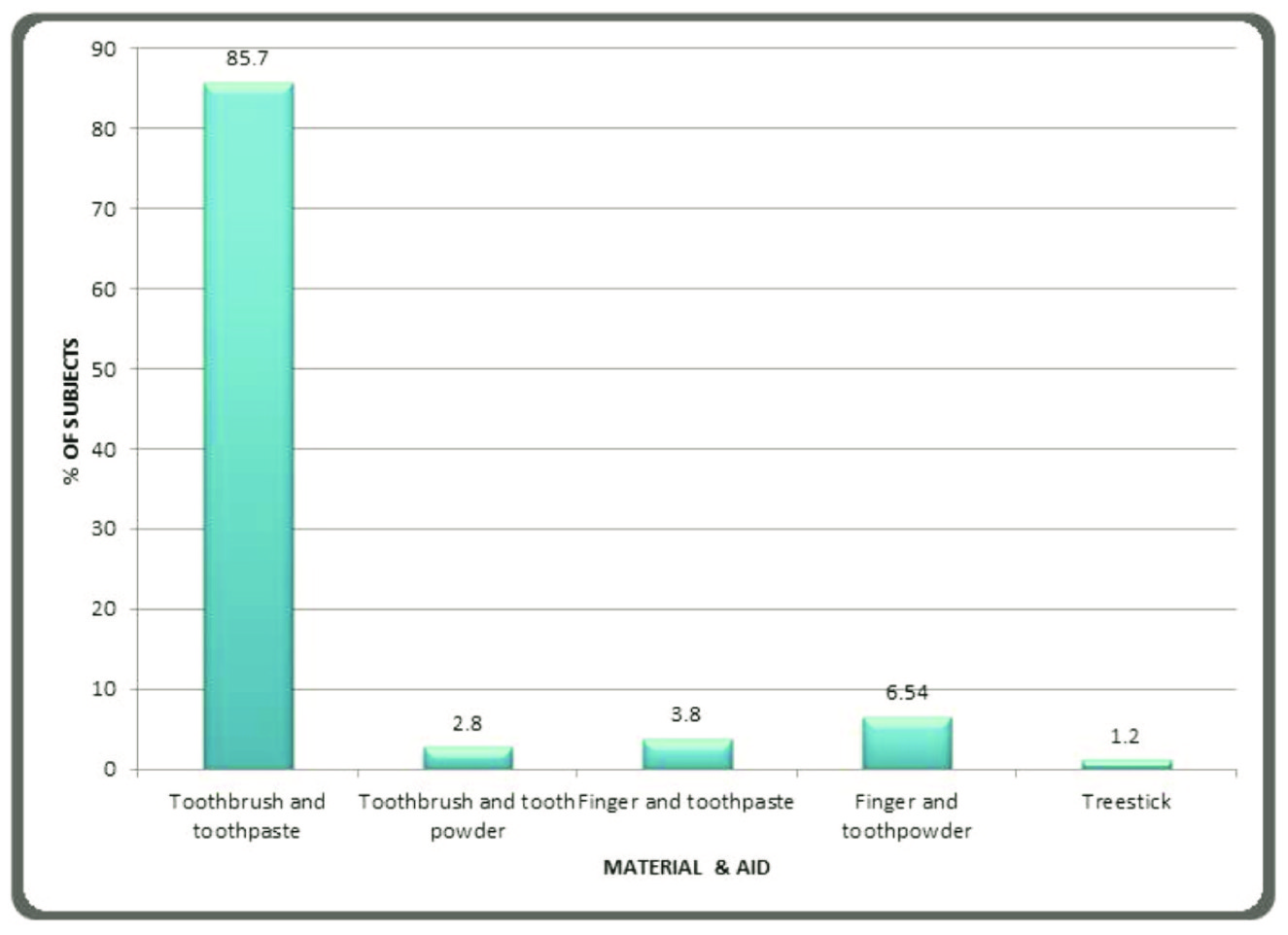
Oral Hygiene Practices
Regarding brushing habits, 88.7% of the subjects used to brush their teeth at least once a day, 9.8% (99) of the subjects brushed their teeth twice a day, while 0.6% (6) of the subjects never used to brush their teeth. While 2.8% (28) of the subjects used toothbrushes and toothpowder [Table/Fig-3]. 79.3% (96) of the smokers brushed their teeth at least once a day, as compared to 14% (17) of the smokers who brushed their teeth twice daily.
Various oral hygiene aids used by the study subjects
Dentition Status
Mean DMFT of the study population was 5.02. Mean numbers of decayed and missing teeth were 1.67 ± 2.16 and 1.46 ± 2.84, respectively and their relationship with age was found to be statistically significant (p<0.01, ANOVA). Mean number of teeth which required one surface filling, two surface fillings and extractions were 0.26 ± 0.74, 0.36 ± 0.72 and 1.1 ± 1.81 respectively [Table/Fig-4a,b] [1]. Subjects who brushed their teeth once a day had higher mean numbers of decayed (1.72) and missing teeth caused by caries (1.47), than subjects who brushed their teeth twice a day (1.56 and 1.26 respectively) [Table/Fig-5]. Mean number of teeth which required extractions were higher in subjects who brushed their teeth once a day, as compared to those seen in subjects who brushed their teeth twice a day. Proportionally, more elderly than younger adults needed extractions, and caries was the major indication for extractions in all age groups.
Comparison between dentition status and age of study population
| Age | n | | Decay | Filled with decay | Filled without decay | Missing due to caries | Missing for other reason | Bridge abutment | Decayed roots |
|---|
| <=20 | 6 | Mean | .17 | .00 | .00 | .00 | .00 | .00 | .00 |
| S.D. | .40 | .00 | .00 | .00 | .00 | .00 | .00 |
| 21-30 | 43 | Mean | 1.12 | .02 | .21 | .40 | .00 | .00 | .00 |
| S.D. | 1.59 | .15 | .63 | 1.49 | .00 | .00 | .00 |
| 31-40 | 209 | Mean | 1.25 | .02 | .37 | .72 | .30 | .01 | .01 |
| S.D. | 1.57 | .13 | 1.07 | 1.53 | .85 | .13 | .099 |
| 41-50 | 457 | Mean | 1.67 | .04 | .32 | 1.53 | 1.04 | .09 | .02 |
| S.D. | 2.28 | .24 | .88 | 2.83 | 2.77 | .59 | .16 |
| 51-60 | 289 | Mean | 2.10 | .07 | .20 | 2.11 | 3.58 | .02 | .02 |
| S.D. | 2.35 | .32 | .69 | 3.53 | 6.98 | .20 | .15 |
| 61-70 | 4 | Mean | 1.25 | .00 | .00 | .00 | .00 | .00 | .00 |
| S.D. | 1.50 | .00 | .00 | .00 | .00 | .00 | .00 |
| Total | 1008 | Mean | 1.67 | .04 | .29 | 1.46 | 1.56 | .05 | .02 |
| S.D. | 2.16 | .24 | .86 | 2.84 | 4.39 | .41 | .14 |
| p value | | | < 0.001 | .24 | .22 | < 0.001 | < 0.001 | .14 | .872 |
*- Statistically significant S.D.- Standard deviation N= Number of subjects in each age-group [1]
Comparison of age of study population with treatment needs
| Age | n | | One surface filling | Two surface filling | Extraction |
|---|
| <=20 | 6 | Mean | 0.0 | 0.0 | 0.0 |
| S.D. | 0.0 | 0.0 | 0.0 |
| 21-30 | 43 | Mean | .39 | .44 | .30 |
| S.D. | .82 | .73 | .96 |
| 31-40 | 209 | Mean | .37 | .33 | .53 |
| S.D. | .82 | .65 | 1.0 |
| 41-50 | 457 | Mean | .24 | .36 | 1.14 |
| S.D. | .75 | .74 | 1.9 |
| 51-60 | 289 | Mean | .20 | .39 | 1.59 |
| S.D. | .65 | .74 | 2.05 |
| 61-70 | 4 | Mean | 0.0 | 0.0 | 1.25 |
| S.D. | 0.0 | 0.0 | 1.5 |
| Total | 1008 | Mean | .26 | .36 | 1.1 |
| S.D. | .74 | .72 | 1.81 |
N= Number of subjects in each age group, S.D.= Standard Deviation [1]
Comparison of dentition status of study population with brushing frequency
| Brushing frequency | | N | Decay | Filled with decay | Filled without decay | Missing due to caries | Missing due to other reason | Bridge abutment | Decayed roots |
|---|
| Never | | Mean | 1.00 | .00 | .00 | .00 | 16.67 | .00 | .00 |
| S.D. | .00 | .00 | .00 | .00 | 14.64 | .00 | .00 |
| Once a day | | Mean | 1.72 | .05 | .27 | 1.47 | 1.19 | .04 | .02 |
| S.D. | 2.07 | .25 | .83 | 2.72 | 3.01 | .39 | .14 |
| Twice a day | | Mean | 1.56 | .03 | .49 | 1.26 | 1.72 | .18 | .02 |
| S.D. | 2.99 | .17 | 1.17 | 2.29 | 4.57 | .64 | .14 |
| Less than once a day | | Mean | 1.11 | .00 | .11 | 1.63 | 1.11 | .00 | .00 |
| S.D. | 1.24 | .00 | .31 | 2.98 | 1.85 | .00 | .00 |
| Total | | Mean | 1.69 | .05 | .29 | 1.44 | 1.29 | .05 | .02 |
| S.D. | 2.16 | .24 | .86 | 2.68 | 3.35 | .42 | .14 |
| p value | | | .543 | .759 | .082 | .681 | < 0.001 | .010* | .948 |
*- Statistically significant S.D.- Standard deviation N= Number of subjects in each age-group
Discussion
In India, there is no national oral health service as there are in other developed countries. Although the government provides formal medical care in the form of primary health centres and community health centres, there is no provision for dental care.
A majority of the study subjects of the present study were not using tobacco and related products, which was contrary to the findings of some other study which was conducted elsewhere in India [4]. According to reports of another studies which had been conducted on health care employees, more number of subjects used to smoke tobacco as compared to that seen in the present study [5,6]. Almost all the subjects in the present study brushed their teeth at least once in a day, which was similar to the results of a study which was conducted in Libya [7] but in the present study, a higher number of smokers used to brush their teeth. Reports of another study conducted on university employees revealed that 68% of the subjects used to brush their teeth more than once daily ,which was much higher than that seen in the present study [8]. This study revealed that more than 80% of the study subjects used toothbrushes to brush their teeth; this is in agreement with findings of a study which was conducted by Patil et al., [9]. This could be attributed to the superior plaque control of toothbrushes, as the bristles of the toothbrushes could reach inter proximal areas as well as pits and fissures of teeth. A statistically significant difference was found with respect to the no. of missing teeth, which was caused by caries, between those who brushed once and those who brushed twice daily, in the present study. This was contrary to findings of Patil et al., [9]. Another study found that 29% of operational engineers used to smoke cigarettes, which was more than that which was seen in the present study [10].
Also, a much lower DMFT was found among the municipal employees of Mysore city as compared to those seen in participants of the present study [11]. According to another study which was conducted in Malaysia, a higher prevalence of dental caries and a higher mean DMFT were recorded among the subjects [12]. Percentage of subjects who had at least one decayed surface in the present study, was almost similar to that seen in some other study which was conducted in southern Illinois [13]. The frequency of decayed teeth and average DMFT in the study population were very less as compared to the findings seen among some mill workers [14]. Mean number of teeth which were missing due to caries was higher in the present study, as compared to that seen in another study which was conducted on government employees [15]. The mean number of teeth which were lost per worker showed a significant increasing trend with age, which was similar to findings of other studies [9,16,17].
Gordon et al., [18] reported in his study that oral surgical needs increased with age and that the older group required more treatment than the younger age-group, which were in agreement with the findings of this study also. This could be due to lack of time for dental treatment and accumulation of treatment needs over a period of time, which were faced by older age groups.
Conclusion
The present study found higher DMFT values among the transport employees. Moreover, caries was a major indication in all age groups. The present study had some limitations. No previous data was available, which was comparable with ours; therefore, the findings of the present study were compared with those of studies done on factory and industrial workers and other employees who worked in similar environments. As permission was granted by the transport authorities to undertake the present study from 9 AM-4 PM; we were not able to enroll those subjects in our study, who reported before and after the study timings. Reducing inequality in oral health between different socio-economic groups in developing countries, has been among the major global goals which have been set for oral health. People of low socio-economic statuses and those who were Below Poverty Line (BPL) realize their lack of expertise in the technical and scientific aspects of health care, but they want a real control in matters of priority, delivery of care, and perhaps, even personnel selection. When any dental awareness programme or campaign is being planned priority should be given to the people who have higher prevalences of dental diseases and unmet treatment needs. This can be done effectively by combining government and multinational initiatives for spreading oral awareness among such populations. Considering the cost of the campaign, if it is often the biggest consideration and limitation when a campaign is being organized, the involvement of different stakeholders in cost sharing would be beneficial.
Recommendations
Transport workers should be educated about oral symptoms, in an effort to forestall or avert the earliest clinical manifestations of disease. Larger studies of this kind are needed, as the results of the present study represent only a section of the transport workers.
[1]. Gambhir Ramandeep S, Sogi Girish M, Kakar Heena, Dental health status and treatment needs of transport workers of a northern Indian city: A cross-sectional studyJ Net Sci Biol Med 2013 4(2):451-56. [Google Scholar]
[2]. Oral Health Surveys Basic methods 1997 4th edGenevaWorld Health Organization [Google Scholar]
[3]. Gordan VV, Riley JL, De Carvalho RM, Snyder J, Sanderson JL Jr, Anderson M, Methods used by dental practice-based research network dentists to diagnose dental cariesTex Dent J 2013 130(4):321-32. [Google Scholar]
[4]. Nagarajappa R, Sanadhya S, Sharda AJ, Asawa K, Tak M, Batra M, The oral health status and the treatment needs of salt worker at sambhar lake, Jaipur, IndiaJ Clin Diagn Res 2013 7(7):1498-503. [Google Scholar]
[5]. Gazdek D, Samardzic S, Croatian smoke-free law and smoking habits among employees of health care facilities in Koprivnica-Križevci CountyCroat Med J 2013 54(4):407-10. [Google Scholar]
[6]. Stojanovic M, Musovic D, Petrovic B, Milosevic Z, Milosavljevic I, Visnjic A, Smoking habits, knowledge about and attitudes toward smoking among employees in health institutions in SerbiaVojnosanit Pregl 2013 70(5):493-500. [Google Scholar]
[7]. Eldarrat A, Alkhabuli J, Malik A, The Prevalence of Self-Reported Halitosis and Oral Hygiene Practices among Libyan Students and Office WorkersLibyan J Med 2008 3(4):170-76. [Google Scholar]
[8]. Sakalauskienc Z, Vehkalahti MM, Murtomaa H, Maciulskienc V, Factors related to gender differences in toothbrushing among Lithuanian middle-aged university employeesMedicina (Kaunas) 2011 47(3):180-86. [Google Scholar]
[9]. Patil V, Shigli K, Hebbal M, Agrawal N, Tooth loss, prosthetic status and treatment needs among industrial workers in Belgaum, Karnataka, IndiaJ Oral Sci 2012 54(4):285-92. [Google Scholar]
[10]. Choi SH, Pohl JM, Terrell JE, Redman RW, Duffy SA, Factors associated with smoking among operating engineersWorkplace Health Saf 2013 61(9):385-92. [Google Scholar]
[11]. Chandra Shekar BR, Reddy C, Oral health status in relation to socioeconomic factors among the municipal employees of Mysore cityIndian J Dent Res 2011 22(3):410-18. [Google Scholar]
[12]. Jasmin B, Jaafar N, Dental health status and treatment needs in the infantry regiment of the Malaysian Territorial ArmyAsia Pac J Public Health 2011 23(2):203-08. [Google Scholar]
[13]. Lukes SM, Simon B, Dental decay in southern Illinois migrant and seasonal farmworkers: an analysis of clinical dataJ Rural Health 2005 21(3):254-58. [Google Scholar]
[14]. Bachanek T, Pawlowicz A, Tarczydlo B, Chalas R, Evaluation of dental health in mill workers. Part-I. The state of dentitionAnn Agric Environ Med 2001 8:103-05. [Google Scholar]
[15]. Kim HY, Lee SW, Cho SI, Patton LL, Ku Y, Associations between missing teeth with unmet needs and socioeconomic status among South Korean dentate government employeesJ Public Health Dent 2007 67(3):174-78. [Google Scholar]
[16]. Petersen PE, Tanase M, Oral health status of an industrial population in RomaniaInt Dent J 1997 47(4):194-98. [Google Scholar]
[17]. Hayashi N, Tamagawa H, Tanaka M, Hanioka T, Maruyama S, Takeshita T, Association of Tooth Loss with Psychosocial Factors in Male Japanese EmployeesJ Occup Health 2005 43:351-55. [Google Scholar]
[18]. Gordon M, Kusner W, Shifman A, Ronen E, Newbrun E, Assessing the dental treatment needs of an adult Israeli military populationCommunity Dent Oral Epidemiol 1986 14:244-49. [Google Scholar]