Low back pain is one of the most common musculoskeletal diseases globally, with high financial burden especially in industrialized countries where approximately 80 per cent of the population suffers from it at least once during their life [1–3]. Low back pain, after common cold, is the most widespread disease in human beings and the second cause of referring the physicians [3].
Materials and Methods
The study protocol was approved by Ethics Committee of Faculty of Medicine (ethics code: 90-10-32) and registration code of IRCT201303106480N5 was issued by Iranian Registry of Clinical Trials for this study. Sample population of this study consisted of all male and female patients, 20-50-years-old, with acute low back pain referring Orthopedic Clinic of Ayatollah Kashani Hospital, Shahrekord (southwest of Iran). Inclusion criteria were as follows: 20- to 50-year-old male and female patients with acute low back pain complaint (developed less than one month ago) referring the Clinic and completion of informed consent form and the questionnaire. The exclusion criteria were underlying (cardiovascular, renal, pulmonary, endocrine, and metabolic) diseases, trauma, taking analgesics apart from naproxen, and undergoing physiotherapy. Ninety patients suffering from acute low back pain were chosen by convenience sampling method. Three patients were excluded from the study because of refusal to receive treatment. The researcher did homogenization through assigning participants randomly in three groups of 29 each [Table/Fig-1]. All three groups were simultaneously treated with naproxen 500 mg twice a day for one week; we judged it as unethical to relieve the pain through only cryotherapy and/or thermotherapy as these two therapies are considered as supplementary ones for relieving pain. Group A (thermotherapy) was treated with hot water bottle twice a day for one week each time for 20 minutes, group B (cryotherapy) with ice twice a day for one week each time for 20 minutes, and group C (naproxen), as control, only with naproxen. All patients were examined on 0, 3rd, 8th, and 15th day after they received treatment.
The data were gathered using McGill Pain Questionnaire (MPQ). MPQ includes two main components for pain assessment. The first component consists of four measures: descriptive, examination, evaluative, and behavioral. The second component of MPQ is related to the pain measurement from an affective dimension. In Iran, Adelmanesh examined the validity and reliability of MPQ and measured its Cronbach’s alfa coefficient as 90 per cent, indicating a scientifically high reliability [15]. The data were analyzed by SPSS 11 using paired t-test, ANOVA, and chi-square.
Results
In this study, the age range of the patients was 20-50 years and their mean age was 34.48 years, of the patients, 51.72 per cent were female and each group consisted of 14 men and 15 women. No significant difference in pain was observed between men and women based on chi-square test (p ≥ 0.05). In terms of occupation, age, and duration of symptoms there was no statistically significant difference among the three groups (p ≥ 0.05).
In the first visit, the intensity of pain in all three groups was equal. In the second visit (three days later), the intensity of pain was significantly reduced in the intervention (thermotherapy and cryotherapy) groups. In addition, the decrease in pain intensity, in terms of pain examination, was higher in thermotherapy group compared to cryotherapy in the second visit. The mean score of pain in thermotherapy group ranged from 12.06 in the first visit to 7.27 in the fourth visit, and in the cryotherapy group from 12.06 in the first visit to 9.27 in the fourth visit. Meanwhile, no significant decrease was observed in the intensity of pain in naproxen group. In the second visit three groups were different regarding the descriptive, examination, and evaluative measures and the second component (affective dimension) of MPQ. Besides, in the third and fourth visits (8 and 15 days later, respectively) the intensity of overall pain decreased and in the fourth visit, the intensity of pain in thermotherapy group, cryotherapy, and naproxen groups reached 0.75, 2.20, and 5.58 respectively. In evaluative measure, decrease in the intensity of pain was higher in the thermotherapy group compared to the other two groups (p<0.05). Less pain was reported in thermotherapy and cryotherapy groups compared to naproxen (p<0.05). The results are comprehensively shown in [Table/Fig-2].
Statistical analysis of the data using McGill Pain Questioannre
| group | Thermotherapy | Naproxen | Cryotherapy | p-value |
|---|
| Variable | Visit turns | Mean ± SD* | Mean ± SD* | Mean ± SD* |
|---|
| Age (year) | 33.66±8.24 | 36.41±8.214 | 33.38±8.364 | |
| Duration of symptoms (day) | 16.38±8.769 | 13.17±6.612 | 17.72±9.471 | |
| Pain measures | Descriptive measures | First | 3.14±1.093 | 3.59±0.852 | 3.10±0.976 | 0.11 |
| Second | 03/2±778/0 | 2.66±0.721 | 2.55±0.985 | 0.01 |
| Third | 1.28±0.694 | 1.97±0.823 | 1.52±0.911 | 0.01 |
| Fourth | 0.45±0.506 | 1.38±0.677 | 0.79±0.774 | 0.00 |
| Examination measures | First | 2.21±0.675 | 2.69±0.471 | 2.48±0.509 | 0.01 |
| Second | 1.45±0.736 | 14/2±639/0 | 1.97±0.499 | 0.00 |
| Third | 0.66±0.721 | 1.72±0.528 | 1±0.463 | 0.00 |
| Fourth | 0.17±0.384 | 1.31±0.541 | 0.48±0.688 | 0.00 |
| Evaluative measures | First | 3.24±1.327 | 3.38±1.015 | 3.10±0.976 | 0.64 |
| Second | 1.86±1.026 | 2.66±0.857 | 2.31±0.806 | 0.05 |
| Third | 0.90±0.817 | 2±0.756 | 1.47±0.733 | 0.00 |
| Fourth | 0.03±0.184 | 1.48±0.634 | 0.52±0.688 | 0.00 |
| Behavioral measures | First | 3.48±1.84 | 3.31±1.004 | 3.38±0.979 | 0.82 |
| Second | 1.93±1.223 | 2.41±0.733 | 2.45±1.055 | 0.12 |
| Third | 0.90±0.673 | 2.03±0.865 | 1.17±0.848 | 0.00 |
| Fourth | 0.10±0.310 | 1.41±0.733 | 0.41±0.568 | 0.00 |
| Second component of MPQ** | First | 7.511±1.975 | 8.214±1.503 | 7.379±1.916 | 0.16 |
| Second | 4.758±1.704 | 6.551±1.594 | 4.931±2.051 | 0.00 |
| Third | 1.965±1.636 | 4.931±1.624 | 2.275±1.849 | 0.00 |
| Fourth | 0.682±0.413 | 3.827±1.774 | 1.241±1.550 | 0.00 |
| Overall pain | First | 12.0690±3.70262 | 12.9655±2.8092 | 12.06±2.63 | 0.44 |
| Second | 7.2759±3.18362 | 9.8621±2.26334 | 9.27±2.67 | <0.05 |
| Third | 3.7241±2.37391 | 7.7241±2.50566 | 5.10±2.30 | 0.00 |
| Fourth | 0.7586±0.37946 | 5.5862±2.00922 | 2.20±2.12 | 0.01 |
* Standard deviation
** McGill Pain Questionnaire
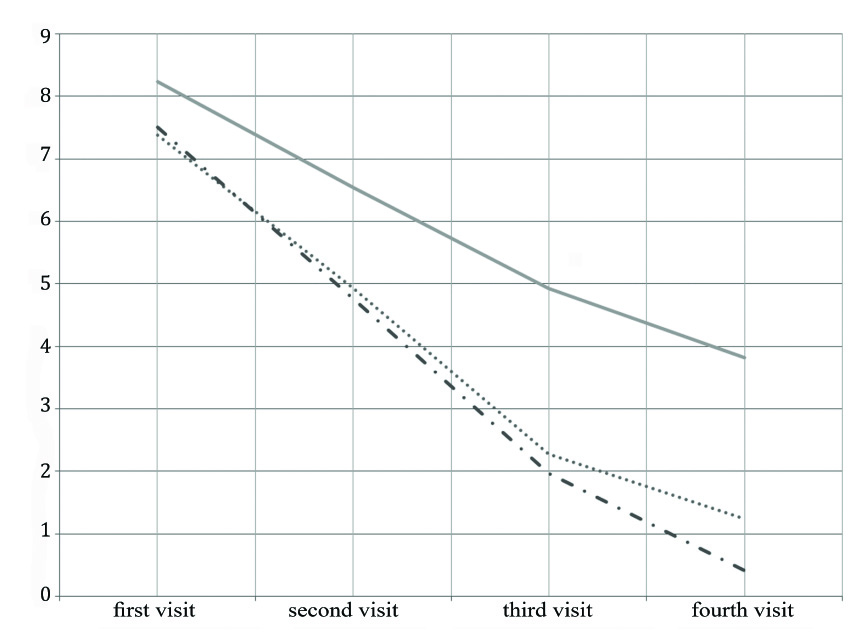
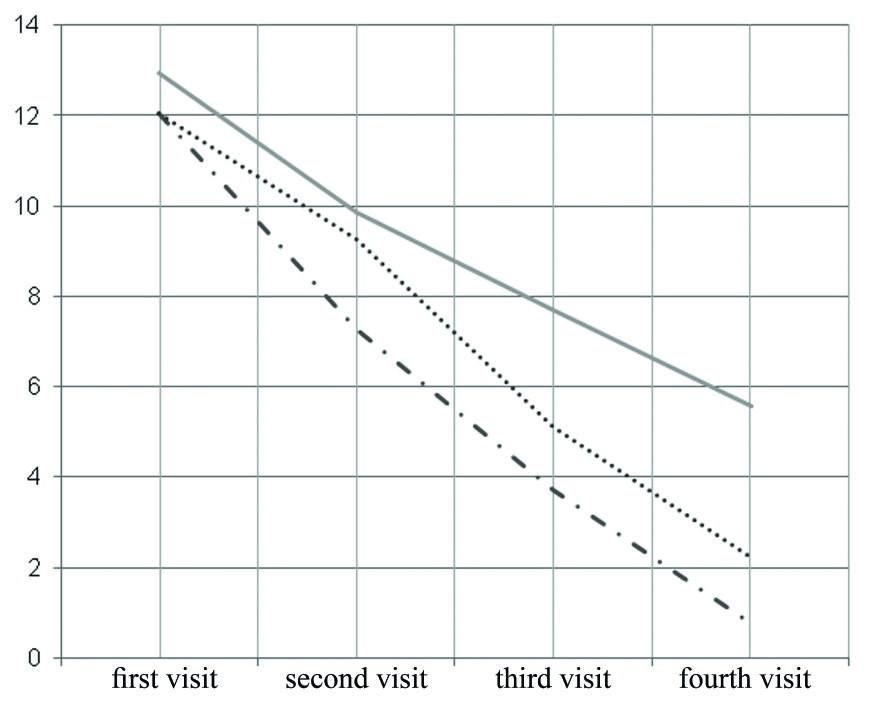
Examining the pain through the second component of MPQ (affective dimension) showed that in the first visit, no significant difference was observed among the three groups (p > 0.05). However, in the second, third, and fourth visits, there was a significant difference among the three groups (p<0.05). Generally, less pain was reported in thermotherapy and cryotherapy groups in comparison to naproxen [Table/Fig-3]. [Table/Fig-4] compares overal mean pain score among thermotherapy, cryotherapy, and naproxen groups during treatment.
The comparison of pain among thermotherapy, cryotherapy, and naproxen groups during treatment (Second component of McGill Pain Questionnaire)
Mean pain score in cryotherapy group································
Mean pain score in thermotherapy group—·——·——·—
Mean pain score in naproxen group
The comparison of overal mean pain score among thermotherapy, cryotherapy, and naproxen groups during treatment.
Mean pain score in cryotherapy group································
Mean pain score in thermotherapy group—·——·——·—
Mean pain score in naproxen group
Discussion
This clinical trial study showed the efficacy of thermotherapy and cryotherapy alongside pharmacologic treatment on relieving pain. Based on the findings of this study, various (examination, behavioral, descriptive, and evaluative) measures and affective dimension were different in the second, third, and fourth visits of the patients among the three groups, which confirms that applying supplementary methods (especially application of thermotherapy) could strengthen the efficacy of pharmacologic treatment and minimize the pain in patients.
There is little evidence on examining the effect of thermotherapy and cryotherapy on low back pain and conflicting evidence on appropriateness of these methods for this pain [16]. However, these interventions seem to yield better outcomes if applied continuously and in long term rather than frequently and in short term [17], consistent with our study’s findings.
Ours findings are consistent with the results of some other studies on the efficacy of thermotherapy and cryotherapy on low back pain relief [12,16,18,19]. In most studies, thermotherapy and cryotherapy were effective, in long term, on pain relief in the patients suffering from low back pain [12,16, 20]. In this regard, a study by Khadilkar et al., on treatment of chronic low back pain indicated that keeping the pain site warm (wrapped up by a blanket) for a long term in the patients with chronic low back pain reduced the pain efficiently [16]. In the present study, thermotherapy minimized acute low back pain in short term. This inconsistency may be due to different instruments (blanket versus hot water bottle) for keeping the pain site warm. Thermotherapy also decreased the intensity of pain in the first and second trimesters of pregnancy in various measures [21]. Continuous application of thermotherapy in a low level was effective on treating acute low back pain and nonspecific low back pain [18], confirming our findings. The results of a study on low back pain in adults showed that thermotherapy after five days reduced pain significantly compared to oral placebo. In that study, acute low back pain was relieved immediately after thermotherapy, confirming the efficacy of thermotherapy (blanket wrapped up for two weeks) on pain relief and inabilities associated with low back pain of shorter than three months [12].
The application of thermotherapy and hot water leads to increase in soft tissue flexibility, muscle resistance, easier and better contraction of smooth muscles, and improvement in the muscles’ motor function [22]. Besides, thermotherapy triggers decline in pain especially low back pain through inhibiting pain signal and exerting pressure on back muscles [18]. In a study in the USA, ice wrapped in a wet handkerchief applied on pain site for 20 minutes caused temporary pain relief and inflammation decrease [23]. In addition, when hot water bottle (especially in case of providing deep heat) was used, the patient’s focus was distracted from his/her pain, the muscles relaxed, and hence the pain relieved. The studies on the effect of thermotherapy illustrate that continued thermotherapy leads to alleviating pain in the patients with acute low back pain, which decreases muscles seizure and resolves inability [18,24]. Besides, cryotherapy leads to reduction in edema and inflammation in the pain site and relief of pain [23].
In contrast to our study, French et al., obtained little evidence on the effect of short-term thermotherapy on acute and subacute low back pain. In their study, exercise was more effective on pain relief and functional improvement [20]. In another study, cryotherapy and thermotherapy as therapeutic methods in the patients with acute and chronic low back pain had an equal effect on relieving the pain based on evaluative and descriptive measures [12], which is consistent with our findings. Kinkade’s study showed that the application of ice and heat pack had an equal effect on the patients suffering from low back pain [13]. Costello et al., concluded that the application of cryotherapy relieved pain immediately and 15 minutes after muscle tone [10], which is similar to our study in terms of efficacy but different considering evaluation time. Based on these findings, further studies could measure combined effects of different treatments including thermotherapy and cryotherapy, massage therapy, acupuncture, stretching, etc. on pain in patients with low back pain.
Conclusion
Taken together, the findings of this study indicated that thermotherapy and cryotherapy caused low back pain to be relieved. Since these methods predictably have fewer side-effects and are economical and accessible, they could be used, alongside pharmacologic treatments, as supplementary ones for reducing pain in the patients with low back pain.
* Standard deviation
** McGill Pain Questionnaire