The Utility of Caesarean Myomectomy as a Safe Procedure: A Retrospective Analysis of 21 Cases with Review of Literature
Ramesh Kumar R1, Manjula Patil2, Shruthi SA3
1 Associate Professor, Department of Obstetrics and Gynecology, SDM College of Medical Science and HospitalSattur, Dharwad, Karnataka, India.
2 Assistant Professor, Department of Obstetrics and Gynecology, SDM College of Medical Science and HospitalSattur, Dharwad, Karnataka, India.
3 Resident, Department of Obstetrics and Gynecology, SDM College of Medical Science and HospitalSattur, Dharwad, Karnataka, India.
NAME, ADDRESS, E-MAIL ID OF THE CORRESPONDING AUTHOR: Dr Ramesh Kumar R, Associate Professor, Department of Obstetrics & Gynecology, SDM Medical College & Hospital, Sattur, Dharwad, Karnataka-580009, India. Phone : 9886071742, E-mail : dr_rameshrk@rediffmail.com
Background: Myomectomy at the time of caesarean delivery has been discouraged because of the risk of intractable haemorrhage and increased postoperative morbidity. The aim of this study is to determine the safety and feasibility of caesarean myomectomy.
Materials and Methods: A retrospective case control study done between June 2012 to May 2013 in a tertiary care teaching hospital in Karnataka, India which included 21 pregnant women with uterine fibroids who underwent myomectomy during caesarean section and were compared with 42 matched controls without uterine fibroids who had caesarean section alone during the same period. Primary outcome measures studied were incidence of haemorrhage and need for blood transfusion. Secondary outcome measures were duration of operation, length of hospital stay, postpartum fever and wound infection. Statistical analysis is done using IBMSPSS 20.0 software and students t-test. For calculation of incidence of haemorrhage Fisher’s exact test is used.
Results: Mean age of the 21 cases was 31.81yrs and 47.62% were primigravida. Total 37 fibroids were removed. Subserosal were 30 cases(81.08%) while 1(2.07%) was submucous. 21(56.76%)fibroids were situated in fundal region and 3(8.11%) were in lower segment. Mean change in the haemoglobin from preoperative to postoperative period in the cases was 1.3gm/dl(±1.155mg/dl) and control was 1.05% (±.854mg/dl). Two of the cases(9.52%) required blood transfusion compared to none in control. None in either group required hysterectomy. Mean duration of surgery was 68.57min (±15.012min)and 51.55min (±9.595min) for controls which is statistically significant.
Conclusion: This study shows that myomectomy during caesarean section is a safe procedure and is not associated with major intraoperative and postoperative complications.
Caesarean section, Haemorrhage, Myomectomy, Myoma
Introduction
Leiomyomata (fibroids) are the benign smooth muscle cell tumours of the uterus and female pelvis [1]. Myomas are usually asymptomatic however sometimes patients present with menorrhagia, dysmenorrhoea, pressure related symptoms of bowel and bladder and infertility. Definitive treatment for symptomatic fibroids is only surgery [2].
Myomas are observed in 2.7% to 12.6% of pregnant women [3]. Most often they do not pose any problem during pregnancy but approximately 10% to 30% of pregnant women develop complications [4]. The location of fibroids determines the risk of bleeding in pregnancy with those situated close to placental site having more bleeding complications [3,5].
Myomectomy during caesarean delivery has traditionally been discouraged. With the exception of small, pedunculated fibroids most of the textbooks advice against caesarean myomectomy due to theoretical risk of massive hemorrhage and increased postoperative morbidity [2]. Contrary to the traditional belief some of the recent reports indicate that in selected patients, myomectomy during caesarean delivery does not appear to result in an increased risk of intrapartum or short term postpartum morbidity and is a safe and effective procedure [6–9].
This retrospective study was conducted in our institution in an attempt to identify the safety and feasibility of caesarean myomectomy.
Materials and Methods
This retrospective study is done in a tertiary care teaching hospital in Karnataka, India in an attempt to identify the safety and feasibility of caesarean myomectomy. All pregnant women who underwent caesarean myomectomy during the period June 2012 to May 2013 were enrolled into study group & 42 pregnant women who underwent caesarean section alone in the same period were taken as control. Controls were matched for age, parity, period of gestation at caesarean section, preoperative haemoglobin and baby birth weight. Data is collected from inpatient and outpatient medical records and operative notes. Data abstracted includes age, parity, period of gestation at caesarean delivery, indication for caesarean delivery, preoperative haemoglobin, size, number, location of myomas removed, birth weight, postoperative haemoglobin which was routinely done 24 hrs of operation in our hospital. In all women, myomectomy was performed after delivery of the baby [Table/Fig-1] except in three cases where myoma was located in the lower uterine segment at the proposed line of incision, myomectomy was done prior to delivery of the baby. Uterine incision for LSCS was closed in two layers with No 1 vicryl. Myomectomy was done by making an incision over the myoma and enucleating it [Table/Fig-2]. The dead space was obliterated by interrupted sutures with 1-0 vicryl. Myoma located near the cornua(1 case) was not removed for fear of distortion of anatomy and patency of fallopian tube. Abdomen was closed in layers after ensuring haemostasis. Techniques used to reduce bleeding were electrocautery, intramyometrial PGF2α and oxytocin infusion [Table/Fig-3].
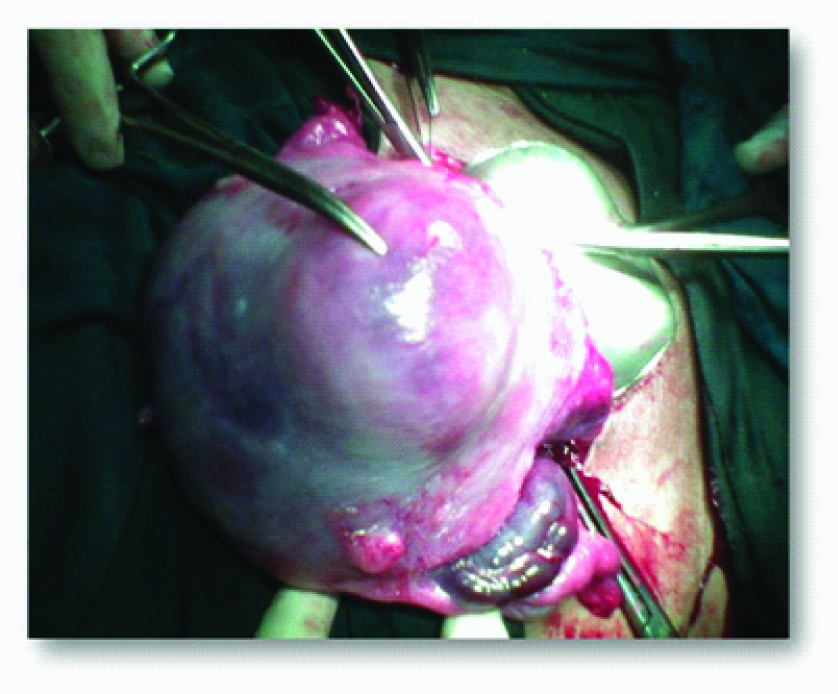
Enucleation of anterior wall fibroid using electrocautery


Primary outcome measures studied were incidence of haemorrhage, significant intraoperative difficulties and blood loss requiring immediate blood transfusion.
Secondary outcome measures were operative time, postpartum fever, wound infection and length of hospital stay. Hemorrhage was defined for study purpose as a decrease in haemoglobin by 3gm/dl or more from the preoperative value to the postoperative value and or the need for intraoperative or postoperative blood transfusion. Operative time was noted from skin incision to skin closure. Fever was defined as postoperative rise in temperature of 38.0°C or greater.
All the data were analysed using IBMSPSS 20.0 software fisher’s exact test for comparison of incidence of haemorrhage and students t-test for other parameters.
Results
During study period of one year, 21 women underwent caesarean myomectomy. Majority of the women i.e. 15 (71.43%) women were in the age group of 31 to 38 years and 10(47.62%) were primigravida [Table/Fig-4]. Most commonly caesarean section was done at term except in two cases of which one had prolonged preterm premature rupture of membranes at 31 weeks of gestation with chorioamnionitis with precious pregnancy and the same patient had 11 fibroids. In other case hysterotomy was done at 22 weeks for a woman with previous 3 LSCS with severe pre eclampsia in present pregnancy. Most common indication for caesarean section was cephalopelvic disproportion followed by foetal distress. Surgical time for caesarean myomectomy was 60 to 75 minutes in majority, 16(76.19%) of the cases and most of the cases blood loss was less than 350ml, In 13cases (61.90%) ,there is </= 1 difference in preoperative & post operative hemoglobin(gm/dl). [Table/Fig-5].
| Number n=21 | Percentage |
|---|
| Age (years) |
| <20 | 01 | 04.76 |
| 20-25 | 02 | 09.52 |
| 26-30 | 03 | 14.29 |
| 31-35 | 11 | 52.38 |
| >35 | 04 | 19.05 |
| Parity |
| Primigravida | 10 | 47.62 |
| 2 | 03 | 14.29 |
| 3 | 04 | 19.05 |
| ≥4 | 04 | 19.05 |
| Gestational age at CS (Weeks) |
| <32 | 02 | 09.52 |
| 32-34 | 00 | 00.00 |
| 35-37 | 03 | 14.29 |
| 38-40 | 15 | 71.43 |
| ≥41 | 01 | 04.76 |
Distribution of secondary outcome
| Number n=21 | Percentage |
|---|
| Duration of surgery (minutes |
| <60 | 02 | 09.52 |
| 60-75 | 16 | 76.19 |
| 75-90 | 02 | 09.52 |
| >90 | 01 | 04.76 |
| Duration of hospital stay (days) |
| <5 | 01 | 04.76 |
| 5-7 | 16 | 76.19 |
| 7-10 | 02 | 09.52 |
| >10 | 02 | 09.52 |
| Difference in preoperative and postoperative haemoglobin(gm/dl) |
| ≤1 | 13 | 61.90 |
| 1.1-2 | 03 | 14.29 |
| 2.1-3 | 04 | 19.05 |
| 3.1-4 | 01 | 04.76 |
A total of 37 fibroids were removed from 21women though multiple fibroids were present in only 5 (23.81%). Mostly fibroids were subserous 30(81.08%) located in the upper segment 34(91.89%)[Table/Fig-6]. Statstical analysis was carried out for the outcome [Table/Fig-7]. There is no statistically significant difference in the mean change of haemoglobin and duration of hospital stay between cases and controls. Incidence of haemorrhage in case group was 3 out of 21 (14.29%) while control was 2 out of 42(4.76%) with p-value .323 which is statistically not significant. One patient in each group had post partum fever and none had wound infection. The difference between operative time in cases and controls is statistically significant.
Distribution of Leiomyomata
| Number | Percentage |
|---|
| Number of fibroids (n= 21) |
| 1 | 16 | 76.19 |
| 2 | 02 | 09.52 |
| 3 | 01 | 04.76 |
| ≥4 | 02 | 09.52 |
| Type of fibroid(n=37) |
| Subserous | 30 | 81.08 |
| Intramural | 06 | 16.22 |
| Submucous | 01 | 02.70 |
| Location of fibroid(n=37) |
| Fundus | 21 | 56.76 |
| Body | 13 | 35.14 |
| Lower segment | 03 | 08.11 |
| Size of fibroid(in cms) ; n= 37 |
| <3 | 14 | 37.84 |
| 3-6 | 14 | 37.84 |
| >6 | 09 | 24.32 |
Statistical analysis of outcome of caesarean myomectomy cases compared with controls
| Group | N | Mean | Std. Deviation | P Value |
|---|
| Hb difference | Cases | 21 | 1.33 | 1.155 | .271 |
| Controls | 42 | 1.05 | .854 |
| Discharge day | Cases | 21 | 7.62 | 3.667 | .183 |
| Controls | 42 | 6.55 | 2.578 |
| OT time | Cases | 21 | 68.57 | 15.012 | .005 |
| Controls | 42 | 51.55 | 9.595 |
Discussion
Leiomyomas are extremely common with the incidence of 40 to 60% by the age of 35 and 70 to 80% by the age of 50 years, the precise aetiology however, still remains unclear [1]. Most of our patients also belonged to the age group of 31 to 35 years (52.38%). Treatment is primarily surgery in the form of myomectomy or hysterectomy if necessary. Hysterectomy is performed for many other indications but leiomyomata uteri are the most common indication for hysterectomy [2]. In our study no patients in either group required hysterectomy.
Fibroids in pregnancy can give rise to complications like preterm delivery, malpresentation, caesarean section and postpartum endomyometritis [3]. Myomas are associated with a significantly increased risk of spontaneous abortion [2], and studies have shown that incidence of spontaneous miscarriage has declined from 41% to 19% following myomectomy [10]. Location of the fibroid is also considered important in predicting reproductive outcome. Klatsky et al., [3] noted that submucosal fibroids had increased association with miscarriages. Majority of fibroids in our study was fundal and subserosal in location (56.76% and 81.08%respectively) resulting in better reproductive outcome.
Fibroids encountered during caesarean section pose a therapeutic dilemma. Myomectomy has traditionally been discouraged during caesarean section. In recent years some authors have advocated routine removal of all anterior wall uterine fibroid during caesarean section [11]. The advantages of caesarean myomectomy is that it obviates the need for interval myomectomy, decreases complications associated with fibroid in subsequent pregnancies and gives sense of relief to patients. It also increases the chances of vaginal delivery in subsequent pregnancies when removed from the lower uterine segment [12].
Burton et al., [9] reported 13 cases of myomectomy at caesarean section. In this study only one case was complicated by intraoperative hemorrhage. They concluded that myomectomy during caesarean section may be safe in carefully selected patients. In the present study incidence of haemorrhage in case group was 14.29% while control was 4.76%.
There was no statistically significant difference in mean change in haemoglobin, incidence of haemorrhage, need for blood transfusion and hospital stay noticed in our study which correlated with studies by Roman et al.,[6], Li et al.,[8] and Brown et al.,[13]. There is statistically significant difference in operative time, which is because of two cases. One case in which 11 fibroids were removed taking 120 minutes and other was a 10x15 cm fibroid was removed taking 90 minutes. The safety of the procedure in moderate or severely anaemic patients could not be evaluated as none of our patients were anaemic.
In this study, it was observed that myomectomy during caesarean section is not associated with increased risk of haemorrhage, need for blood transfusion, prolonged operative time, hospital stay, postoperative fever or wound infection. These results indicate that myomectomy during caesarean delivery can be a safe procedure. With more number of case series in the future proving the safety of caesarean myomectomy it may no longer remain an absolute contraindication.
[1]. Day BD, Dunson DB, Hill MC, High cumulative incidence of uterine leiomyoma in black and white women: ultrasound evidenceAm J Obstet Gynecol 2003 188:100-07. [Google Scholar]
[2]. Breech Lesly L, John AR, Leiomyomata uteri and myomectomy. In, John A. Rock, Howard W.Jones IIITelindes operative gynaecology 2008 10th editionLippincottWilliams & Wilkins:687-726. [Google Scholar]
[3]. Klatsky PC, Tran ND, Caughey AB, Fujimoto VY, Fibroids and reproductive outcomes: a systematic literature review from conception to deliveryAm J ObstetGynecol 2008 198:357-66. [Google Scholar]
[4]. Katz VL, Dotters DJ, Droegemueller W, Complications of uterine leiomyomas in pregnancyObstet Gynecol 1989 73:593-96. [Google Scholar]
[5]. Lee HJ, Norwitz ER, Shaw J, Contemporary management of fibroids in pregnancyRev Obstet Gynecol 2010 3(1):20-27. [Google Scholar]
[6]. Roman A S, Tabsh K M, Myomectomy at time of caesarean delivery: a retrospective cohort studyBMC Pregnancy Childbirth 2004 4(1):14 [Google Scholar]
[7]. Myomas and reproductive function : The Practice Committee for the American Society for Reproductive Medicine in collaboration with The Society of Reproductive SurgeonsFertility and Sterility 2008 90:S125-30. [Google Scholar]
[8]. Li H, Jin L, Shi Z, Liu M, Myomectomy during caesarean sectionActaObstetGynecol Scand 2009 88(2):183-86. [Google Scholar]
[9]. Burton CA, Grimes DA, March CM, Surgical management of leimyomata during pregnancyObstetGynecol 1989 74:707-09. [Google Scholar]
[10]. Buttram VC, Reiter RC, Uterine leiomyomata: etiology, symptomatology and managementFertil steril 1981 36:433 [Google Scholar]
[11]. Kwawukume EY, Myomectomy during caesarean sectionInt J Gynaecol Obstet 2002 76:183-84. [Google Scholar]
[12]. Omar S Z, Sivanesaratnam V, Damodaran P, Large lower segment myoma: Myomectomy at lower segment section - a report of two casesSingapore Med J 1999 40:109-10. [Google Scholar]
[13]. Brown D, Fletcher HM, Myrie MO, Reid M, Caesarean myomectomy-a safe procedure. A retrospective case controlled studyJ Obstet Gynaecol 1999 19(2):139-41. [Google Scholar]