Sylvian Fissure Dermoid Cyst - A Rare case
Deepak Anand1, Simmi Aggarwal2, Divya Soin3, Ravinder Garg4
1 Consultant, Department of Neurosurgery, Gangaram Bansal Hospital, Sri Ganganagar, Rajasthan, India.
2 Professor & Head, Department of Radiodiagnosis, GGS Medical College & Hospital, Faridkot, Punjab, India.
3 Associate Professor, Department of Medicine, GGS Medical College & Hospital, Faridkot, Punjab, India.
4 Associate Professor, Department of Medicine, GGS Medical College & Hospital, Faridkot, Punjab, India.
NAME, ADDRESS, E-MAIL ID OF THE CORRESPONDING AUTHOR: Dr. Simmi Aggarwal, Professor & Head, Department of Radiodiagnosis, GGS Medical College & Hospital, Faridkot, Punjab – 151203, India. Phone : +91-93569-12818, E-mail : drsimmigarg@gmail.com
Intracranial dermoid cysts are rare tumours which usually occur in the midline. Sylvian fissure is a very unusual site for this lesion. This case presents a patient with unruptured dermoid cyst in the left sylvian fissure who was operated successfully without any residual deficit.
Dermoid cyst, Rare tumour, Sylvian fissure
Case Report
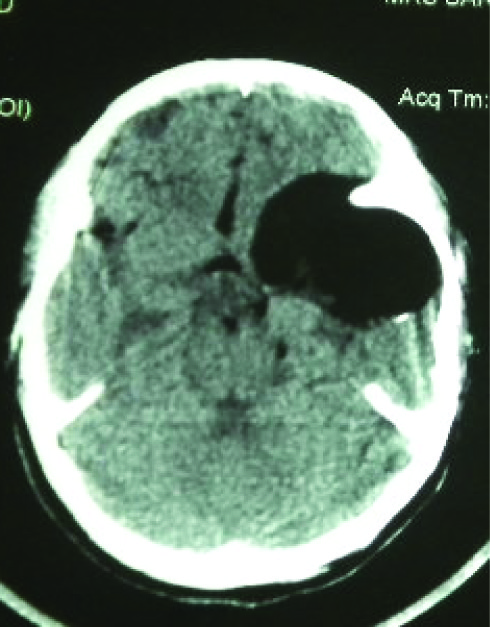
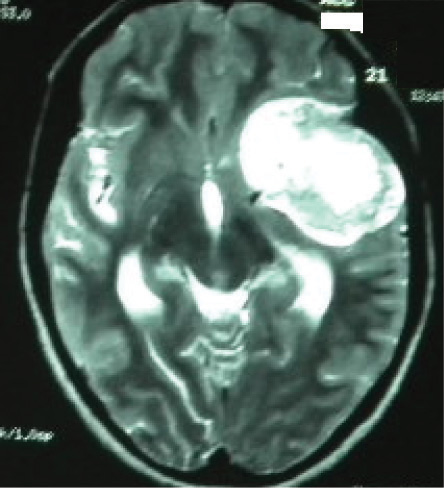
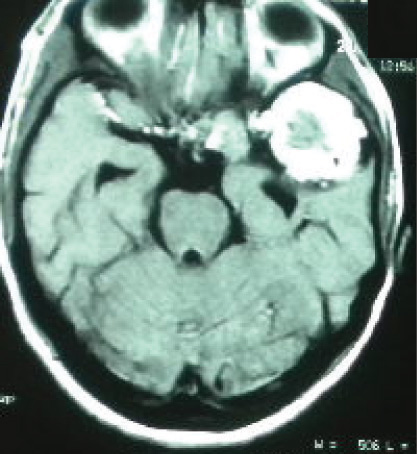
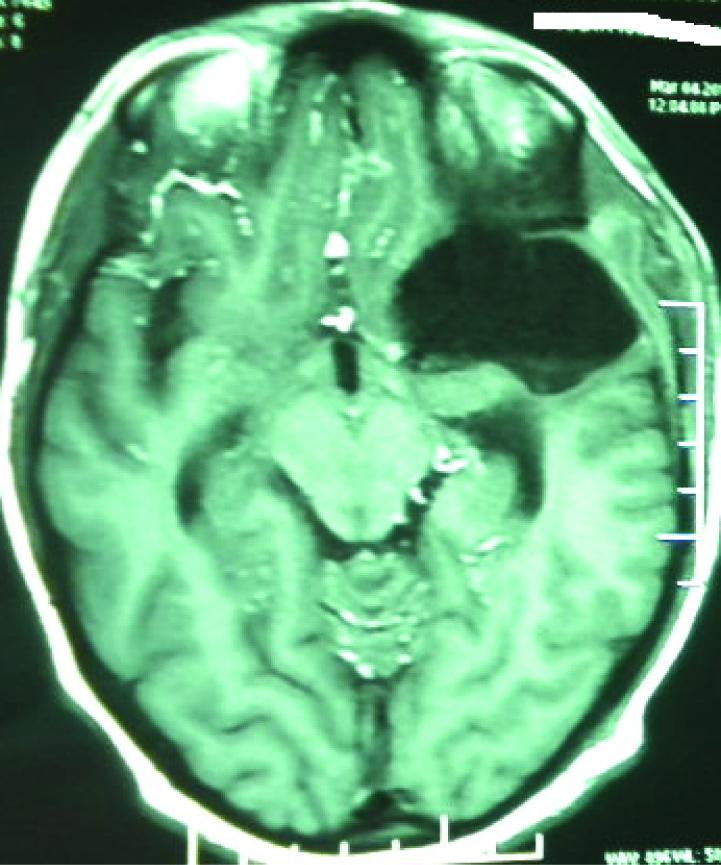
A 30-year-old female presented with complaints of headache and generalized seizures from one month. Headache was waxing and waning type, more so during night. She had no complaints of nausea, vomiting or altered mental status. On presentation, vital signs were normal. No focal neurological deficits were identified. The complete blood count, serum biochemistry and electrolytes were within normal limits. The CT scan revealed a supratentorial hypodense lesion in the left sylvian fissure with marginal calcification [Table/Fig-1]. MRI showed a heterogeneously hyperintense SOL in the left sylvian fissure on T1WI and T2WI [Table/Fig-2,3]. Post contrast images showed mild peripheral enhancement. The possibility of epidermoid cyst was given. Patient was taken up for surgery. Left pterional craniotomy with transsylvian removal of the mass was done. Dura was elevated, thick yellowish fluid came out. Cheesy material with hair was seen in between. Postoperatively, patient had one episode of seizure. Patient was given dexamethsone and antiepileptics. Patient recovered and was discharged in satisfactory condition [Table/Fig-4]. One year follow up showed no deficit. Histopathological findings were consistent with Dermoid cyst.
Axial CT Image of the patient showing a hypodense SOL showing fat attenuation with few internal hypodensities in the left fronto-temporal region. Marginal calcification is seen posteriorly.No surrounding edema is seen
Axial T2-Weighted image showing heterogeneously hyperintense SOL in left temporal with extension into frontal region. No surrounding edema is seen
Post contrast axial T1WI showing SOL with heterogenous signal intensity
Post-operative image of the patient showing parenchymal defect in left temporal region. No abnormal enhancement is seen
Discussion
Dermiod cysts are rare benign tumours, accounting for less than 1% of all intracranial tumours. They are non neoplastic, congenital ectodermal inclusion cysts that contain varying amount of ectodermal derivatives to include apocrine, sweat and sebaceous cysts as well as hair follicles, squamous epithelium and teeth [1]. They may be detected incidentally on brain CT or MRI for unrelated clinical complaints or during imaging investigation of unexplained headache, seizures or olfactory delusions. They may be intact or ruptured on presentation. Unruptured dermoid cysts usually present with focal mass effect, hydrocephalus or elevated intracranial pressure. By contrast ruptured dermoid may cause seizures, aseptic meningitis, acute or chronic obstructive hydrocephalus or cerebral ischemia [2]. The peak incidence is between 3rd and 5th decade [3].They are most often found in the sellar and parasellar region, frontonasal region and reside near the skull base. In the posterior fossa they are found in close proximity to the 4th ventricle. The sylvian fissure is a rare site as dermoid cysts usually occur in the midline. It is a hypovascular tumor and sylvian fissure has rich vascularity, so surgical removal and complete resection can lead to excessive bleeding or intratumoral haemorrhage. Dermoid cyst is a well defined lobulated pearly mass of variable size. Capsule is thick and may contain plaques of calcification.The cyst contains disagreeable foul smelling, yellowish material and desquamated epithelium. Growth can lead to rupture of cyst contents, causing chemical meningitis that may lead to vasospam, infarction and even death. Malignant transformation into squamous cell carcinoma has also been described. The symptoms of intracranial dermoid cyst depend upon site, size and depth of the tumour and whether it is ruptured or unruptured. Common clinical presentation of patients with intact dermiod cysts include headache, visual defects and seizures [1]. Ruptured dermoid cysts may present with meningitis, acute hemiparesis, cherio oral syndrome, ventriculitis, hydrocephalus and cerebral ischemia [1] . Our patient manifested with off and on headache for which she was investigated radiologically. Imaging characteristics of dermoid cysts depend on the contents of the lesion. On CT scan unruptured dermoid cysts are demonstrated as homogenous unilocular hypodense SOL with attenuation value between 0-150HU. Calcification is common; contrast enhancement and edema is not seen. Small mass effect may be seen [4]. On MRI, dermoid cysts are markedly hyperintense on T1WI due to fat content which consist of triglyceride and unsaturated fatty acids. Hypointensity of the mass on T2WI may be throughout or within one or more loculations within the lesion. Other portions of the lesion demonstrate heterogenous hyperintensity due to its mixed composition [5]. FLAIR images help in differentiating fat from fliud which appears bright on background of suppressed fluid signal (dark).Chemical shift selective fat-water-imaging also helps in identification of lipid content in which the signal of water is suppressed and fat signal is selectively enhanced. A 3-D chemical shift selective gradient imaging demonstrates excellent contrast between fat, brain tissue and CSF with added advantage of demonstration of small amounts of free lipid in CSF [6]. In our patient the lesion was hypodense on CT scan with marginal calcification. On MRI, the lesion was heterogeously hyperintense on T1 and T2WI. Post contrast images showed mild peripheral enhancement. The cyst may rupture into subarachnoid space which demonstrates droplets and streaks of high intensity in subarachnoid cisterns about the tumour and more distally. Rupture within the ventricles is seen as a fat fluid level that develops in the anteriosuperior portions. Extensive pial enhancement can be seen due to chemical meningitis. Chemical meningitis is a rare complication of ruptured dermoid and occurs in approximately 7% of cases. It may elicit transient cerebral ischemia secondary to vasospasm with complicating infarction leading to death [1]. Differential diagnosis includes epidermoid cyst, arachnoid cyst and cystic cranoipharyngiomas. Epidermoid cysts have more variable location than dermoid cysts and show greater deviation from midline. Following complete or near total excision of dermoid cyst, recurrence is rare as compared to epidermoid cyst which tends to recur. Radical resection is not advised if critical neurovascular structures are involved [7]. Cystic craniopharyngiomas and arachnoid cysts can be differentiated from dermoids by presence of fat in dermoids and using FLAIR sequences [6]. Despite good availability of routine MR imaging, the diagnosis of dermoid cysts still remain a challenge, probably due to low incidence [8].
Conclusion
Although benign but this rare entity of sylvian fissure dermoid cyst can lead to complications if unrecognized or not operated in time. This case highlights the importance of early diagnosis and intervention in these rare tumours.
[1]. Ray MJ, Barnett DW, Snipes GJ, Layton KF, Opatowsky MJ, Ruptured intracranial dermoid cystProc (Bayl Univ Med Cent) 2012 25(1):23-25. [Google Scholar]
[2]. Chen JC, Chen Y, Lin SM, Tseng SH, Sylvian fissure dermoid cyst with intratumoral hemorrhage: case reportClinical Neurology and Neurosurgery 2004 1320:1-4. [Google Scholar]
[3]. Osbourn AG, Tong KA, Handbook of Neuroradiology: Brain and Skull 1996 2nd ednNew YorkCV Mosby:322-27. [Google Scholar]
[4]. Carberry GA, Medhkour A, Elsamaloty H, Intraventricular rupture of an intracranial dermoid cyst with pseudotumour cerebriPan Arab Journal of Neurosurgery 2011 15(2):64-6. [Google Scholar]
[5]. Scott AW, Magnetic Resonance Imaging of the Brain and Spine 2009 4th edn:581-84. [Google Scholar]
[6]. Venkatesh SK, Phadke RV, Trivedi P, Bannerji D, Asymptomatic spontaneous rupture of suprasellar dermoid cyst: A rare caseNeurology India 2002 50:480-83. [Google Scholar]
[7]. Li Q, You C, Zan X, Chen N, Zhou L, Xu J, Mature cystic teratama (dermoid cyst) in the sylvion fissue: A case report and review of literatureJ of Child Neurology 2012 27(2):211-17. [Google Scholar]
[8]. Schmeider UC, Koch A, Stenzel W, Thomale UW, Intracranial supratentorial dermoid cysts in paediatric patients-Two cases and review of literatureChild’s Nervous System 2012 28(2):185 [Google Scholar]