FATCO Syndrome Variant - Fibular Hypoplasia, Tibial Campomelia and Oligosyndactyly –– A Case Report
Navendu Goyal1, Randeep Kaur2, Manu Gupta3, Shiraz Bhatty4, Rajesh Paul5
1 Consultant, Department of Orthopaedics, Surgeon, SGHS Hospital, Sohana, Mohali, Punjab, India.
2 Senior Resident, Department of Anesthesia, PGIMER, Chandigarh, India.
3 Consultant, Department of Anesthesia, Surgeon, Panchkula, Haryana, India.
4 Associate Professor, Department of Anesthesia, GGMCH, Faridkot, Punjab, India.
5 Professor and Head, Department of Anesthesia, GGMCH, Faridkot, Punjab, India.
NAME, ADDRESS, E-MAIL ID OF THE CORRESPONDING AUTHOR: Dr. Navendu Goyal, House No. 1039, Sector-4, Panchkula, Haryana-134112, India. Phone : +91-9646599819,
E-mail: navendugoyal@gmail.com
The word aplasia/hypoplasia is used for partial or total absence of a bone. Fibula, a lower limb bone is one of the most common to be involved with this and its incidence is amongst the highest in long bone deficiencies.
FATCO syndrome consisting of fibular aplasia, tibial campomelia and oligosyndactyly has been described in the literature but only one has been reported from India as per our literature review. However, it is important to know multiple regional involvement can occur along with this syndrome and prove to be a major difficulty for the child and the parents both.
Due to the rarity of reports on this rare syndrome and difficulty in treatment it is important that each such case should be described to make the management easier.
Absent talus, Congenital anomaly, Fibular hemimelia, Oligosyndactyly, Tarsal coalition
Case Report
A 2-year-old boy presented with valgus deformity of the right foot with oligosyndactyly of the lateral rays. There was skin dimpling in the anterior aspect of leg in the distal 1/3rd region along with antero lateral bowing. Right lower limb was 2 cm shorter than the left lower limb. The right foot was also shorter than the left foot. There was no associated anomaly in the upper limbs, the contralateral lower limb or other parts of the body.
The patient’s medical history was unremarkable. He was born to a non-consanguineous marriage by full term normal vaginal delivery. There was no history of any pre or post natal complications. Developmental milestones were at time. There is no history of pre partum drug intake .There was no history of similar complaints in the family. He had had no prior treatment for the condition.
Physical examination revealed no evidence of ankle, knee or hip instability bilaterally. The range of motion for the ankles, knees and hips was full and painless bilaterally. There was absence of lateral rays with oligosyndactyly.
[Table/Fig-1a,b] – Clinical photos of the affected limb.
Clinical photograph of affected limb

Plain radiographs showed a hypoplastic fibula with hypoplasia of ipsilateral talus. In an effort to further delineate the pathology; computerized tomographic (CT) scan of the right foot was done which further confirmed the findings.
[Table/Fig-2a,b–3]. Radiographs showing anteroposterior and lateral views of the involved and opposite limb.
Radiograph showing anteroposterior view
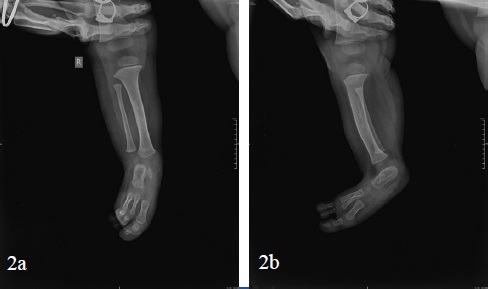
Radiograph showing lateral view of involved and opposite limb

The parents were informed about the nature of the deformity and possible treatment options, including fabrication of a new orthoses with surgical limb lengthening at a later date.
Discussion
Incidence of limb malformations in children is about 1 in 1000 [1,2]. Fibular hemimelia or absence of fibula is a rare disorder with estimated incidence of 5.7 to 20 cases per 1 million births [3]. The exact etiology is not known. It usually represents an isolated sporadic or isolated event but it may be a part of the malformation syndrome [4]. Even though it is a rare condition, it is the most common malformation amongst the long bone deficiency syndromes. The fibula is short or absent with associated tarsal anomalies including agenesis or hypoplasia. The ipsilateral foot usually lacks lateral rays and is shorter than the contralateral foot. The number of absent rays is proportional to the severity of the disease. Fibular aplasia-tibial campomelia-oligosyndactyly (FATCO) syndrome is the term describing this rare syndromic condition with the above components [1,5].
Genetic basis of fibular hemimelia is still unclear [1,6,7]. Fuhrmann syndrome and Al-Awadi Syndromes are said to be similar to FATCO syndrome [8]. However, they are different from FATCO in terms of presence of nail dysplasias and mutations in the WNT7a gene [8]. WNT7a mutations were not found in previous cases of FATCO syndrome which have been reported in the literature [6,7,9]. Phenotypic inheritance can be variable and FATCO syndrome can have autosomal dominant or recessive inheritance, both of which have been described in previously reported cases in literature [1,6,8,10].
Various other anomalies which are often associated with fibular hemimelia include anterolateral bowing of the tibia, valgus deformity at the knee, condylar hypoplasia or agenesis, short femur, proximal focal femoral deficiency and coxa vara. The patient described in this case report had mild anterolateral bowing of the tibia.
The goal of treatment for fibular hemimelia is to correct the leg length discrepancy and to functionally stabilize knee and ankle joints. Commonly accepted avenues of treatment include the use of an orthoses, epiphysiodesis, limb lengthening, and amputation with prosthesis. Successful results have been reported with the use of circular external fixators for limb salvage and, in cases where amputation was indicated, the Symes amputation has been reported to be the procedure of choice in the past [4,11].
In our case, neither instability nor pain was reported by the patient. The clinical abnormality of most concern to the patient was his short right lower extremity, and he was only symptomatic in relation to the weight of lift-orthoses and shoe combination that he used on his right side. Radiographically, this patient’s presentation is extremely rare in that fibular hypoplasia was observed in combination with hypoplasia of the talus.
It is important to note that the classical described case of FATCO involves aplasia of the fibula, however our case only had fibular hypoplasia [1,8]. Previously reported cases had a male preponderance, so was our study with the case being of a boy [1,6, 8]. Only about 9 cases have been reported in the literature with only one case being reported from the Indian subcontinent [8].
One of the important aspects of any syndromic disease is parental counselling and preparing them for what is inevitable. FATCO syndrome is also very important from this aspect and parental counselling is very important to make them aware of what the disease is and what the future holds for the parent and the child.
Conclusion
FATCO syndrome is a rare entity and can be associated with great morbidity and mortality due to its association with multiple body systems. Further parental counselling is necessary as there are chances of future generations being born with this syndrome and only a timely prenatal diagnosis and intervention can prevent complication related to the syndrome.
[1]. Courtens W, Jespers A, Harrewijn I, Puylaert D, Vanhoenacker F, Fibular aplasia, tibial campomelia, and oligosyndactyly in a male newborn infant: a case report and review of the literatureAmerican journal of medical genetics Part A 2005 134(3):321-25. [Google Scholar]
[2]. Holder-Espinasse M, Devisme L, Thomas D, Boute O, Vaast P, Fron D, Pre- and postnatal diagnosis of limb anomalies: a series of 107 casesAmerican journal of medical genetics Part A 2004 124A(4):417-22. [Google Scholar]
[3]. Geipel A, Berg C, Germer U, Krokowski M, Smrcek J, Gembruch U, Prenatal diagnosis of femur-fibula-ulna complex by ultrasound examination at 20 weeks of gestationUltrasound in obstetrics & gynecology : the official journal of the International Society of Ultrasound in Obstetrics and Gynecology 2003 22(1):79-81. [Google Scholar]
[4]. Choi IH, Kumar SJ, Bowen JR, Amputation or limb-lengthening for partial or total absence of the fibulaThe Journal of bone and joint surgery American volume 1990 72(9):1391-99. [Google Scholar]
[5]. Courtens W, Vanhoenacker F, Response to “Letter: Fibular aplasia, tibial campomelia and oligosyndactyly” by Evans and ElliottAmerican journal of medical genetics Part A 2006 140(12):1353 [Google Scholar]
[6]. Kitaoka T, Namba N, Kim JY, Kubota T, Miura K, Miyoshi Y, A Japanese male patient with ‘fibular aplasia, tibial campomelia and oligodactyly’: an additional case report. Clinical pediatric endocrinology : case reports and clinical investigationsofficial journal of the Japanese Society for Pediatric Endocrinology 2009 18(3):81-86. [Google Scholar]
[7]. Karaman A, Kahveci H, A male newborn infant with fatco syndrome [fibular aplasia, tibial campomelia and oligodactyly]: a case reportGenetic Counseling 2010 21(3):285-88. [Google Scholar]
[8]. Ekbote AV, Danda S, A case report of fibular aplasia, tibial campomelia, and oligosyndactyly [FATCO] syndrome associated with Klinefelter syndrome and review of the literatureFoot & Ankle Specialist 2012 5(1):37-40. [Google Scholar]
[9]. Woods CG, Stricker S, Seemann P, Stern R, Cox J, Sherridan E, Mutations in WNT7A cause a range of limb malformations, including Fuhrmann syndrome and Al-Awadi/Raas-Rothschild/Schinzel phocomelia syndromeAmerican journal of Human Genetics 2006 79(2):402-08. [Google Scholar]
[10]. Vyskocil V, Dortova E, Dort J, Chudacek Z, FATCO syndrome--fibular aplasia, tibial campomelia and oligosyndactylyJoint, Bone, Spine : Revue Du Rhumatisme 2011 78(2):217-18. [Google Scholar]
[11]. Epps CH Jr., Schneider PL, Treatment of hemimelias of the lower extremity. Long-term resultsThe Journal of Bone and Joint Surgery American Volume 1989 71(2):273-77. [Google Scholar]