Intramuscular Hemangioma of the Oral Cavity - A Case Report
Sushruth K Nayak1, Prachi Nayak2
1Reader, Department of Oral and Maxillofacial Pathology & Microbiology, Chattisgarh Dental College and Research Institute, Rajnandgaon, Chhattisgarh, India.
2Faculty, Department of Oral and Maxillofacial Pathology & Microbiology, Chattisgarh Dental College and Research Institute, Rajnandgaon, Chhattisgarh, India.
NAME, ADDRESS, E-MAIL ID OF THE CORRESPONDING AUTHOR: Dr. Sushruth K. Nayak, Reader, Department of Oral and Maxillofacial Pathology & Microbiology, Chattisgarh Dental College and Research Institute, Rajnandgaon - 491441, Chhattisgarh, India.
Phone: +919755443274,
E-mail: sushruthnayak@yahoo.com
Haemangiomas are the most common benign soft tissue tumor of the oral cavity. It often presents at birth or soon after, and appears as a soft and vascular swelling in lip, tongue, or buccal mucosa. This article reports a rare case of intra muscular haemangioma of the buccal mucosa in a 27-year-old female patient.
Buccal mucosa, Ulcer, Swelling
Case Report
A 27-year-old female patient reported with the complaint of pain in right cheek region since one week. Pain was intermittent, dull, increased in cold climate and relieved on medication. Patient gave the history of swelling which had slowly increased in size in right cheek region since 10 years. There was history of increase in intensity of pain which was not associated with any other particular activities since one week. Past medical history revealed that patient had undergone operation in the same region for the swelling previously which has not been reported in any of the early literature. There was no associated drug and family history associated with the patient.
Extra oral inspection revealed a diffuse soft tissue swelling on right middle third of the face measuring 2 x 2cm. Swelling was extending 3 cm behind corner of mouth and 2.5 cm anterior to the ramus. Superiorly, it extended up to zygomatic arch and inferiorly 3cm above lower border of mandible. On palpation the swelling was tender and soft to firm in consistency, with no change in the colour. The overlying skin was normal.
Intraoral examination revealed a diffuse swelling in right cheek extending anteriorly from distal lower premolar region measuring 2 x 2cm. Mucosa covering the lesion was ulcerated adjacent to molar region. Ulcer was measuring 0.5 x 0.4cm with erythematous surrounding mucosa and a white base [Table/Fig-1]. On palpation ulcerated area was tender, with no induration of borders, soft in consistency and compressible in nature without any secretion.
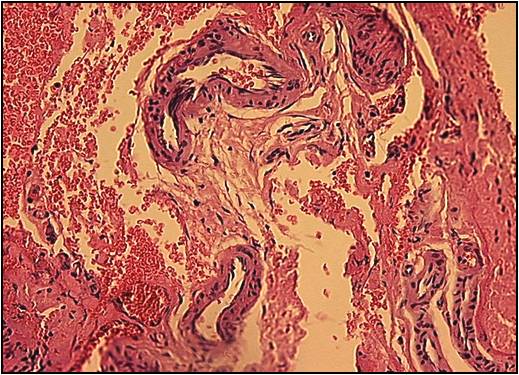
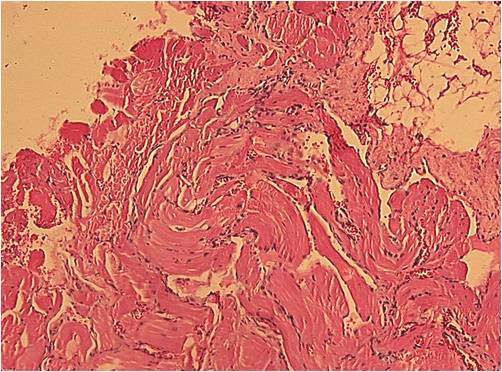
Provisional diagnosis of traumatic ulcer, with differential diagnosis of aphthous ulcer and irritational fibroma was made. An incisional biopsy was done after taking the informed consent of the patient. The specimen was subjected to histopathological examination. H&E stained sections revealed the presence of blood vessels of different sizes with in dense stroma along with longitudinal and transverse section of muscles, areas of hemorrhage and adipose tissue along with very mild inflammatory infiltrate[Table/Fig-2,3].
The histopathologic features were suggestive of Hemangioma (intramuscular type). Surgical excision of the lesion was done and the patient was under follow up for one year without any recurrence.
Intraoral examination showing ulcer

H&E showing presence of blood vessels
H&E showing adipose tissue and mild inflammatory infiltrate
Discussion
Intramuscular haemangioma are rare benign congenital neoplasms which account for less than 1% of all haemangioma, and less than 20% of these are found in the head and neck area. The masseter muscle is the most frequently involved site in the head and neck area accounting for 5% of all intramuscular haemangioma [1-3]. Unlike infantile cutaneous haemangioma, they do not regress spontaneously, and have a deep location with unfamiliar presentation [1,2]. These tumors usually appear after birth, grow rapidly, and involute over the years [4]. Within the spectrum of vascular lesions, intramuscular haemangioma are very rare, accounting for less than 1% of all haemangioma, and the masseter muscle is the most frequent muscle, accounting for 5% of all intramuscular haemangioma [2,3]. Afsar FS [5] reported a case of intramuscular haemangioma of the masseter muscle in a 9 year old girl, where the patient presented with bluish macules on the right inferior eyelid and right zygomatic area with mild pain on the right cheek from last one year. In the present case, patient was 27-year-old with swelling on the right cheek which had gradually increased in size from last 10 years associated with intermittent and dull pain which increased in intensity since one week. Jain V [6] and Zengin AZ [7] also reported the cases of intramuscular haemangiomas of the oral cavity. Most of the cases reported in the literature are in children below 10 years of age when compared to our case where the age was 27 years. Intramuscular haemangioma are non-metastasizing benign congenital tumors that, after remaining unrecognized for long periods, may suddenly start to grow in the second or third decade of life [2,3] and are usually asymptomatic until a growth spurt occurs, at which time pain occurs in about 50% of cases as in the present case. A possible hormonal role in the growth of intramuscular haemangioma was speculated, but no specific data was available to prove this hypothesis [2]. A palpable, fluctuant or firm mass is present in up to 98% of cases1 as compared to the present case where the lesion on palpation was soft to firm in consistency.
Conclusion
Most haemangioma are recognized clinically and do not require any investigation or any treatment as they will subside spontaneously. However, in the present case where clinical diagnosis is difficult with the presence of ulcer intra orally, the histopathological diagnosis and the treatment plan will be of atmost importance.
[1]. GT Terezhalmy, CK Riley, WS Moore, Intramuscular hemangiomasQuintessence Int 2000 31:142-43. [Google Scholar]
[2]. GT Wolf, F Daniel, CJ Krause, A Arbor, RS Kaufman, Intramuscular hemangiomas of the head and neckLaryngoscope. 1985 95:210-13. [Google Scholar]
[3]. JL Rossiter, RA Hendrix, LW Tom, WP Potsic, Intramuscular hemangiomas of the head and neck. Otolaryngol Head Neck Surg 1993 108:18-26. [Google Scholar]
[4]. TJ Gampper, RF Morgan, Vascular anomalies: hemangiomasPlast Reconstr Surg. 2002 110:572-85. [Google Scholar]
[5]. FS Afsar, E Oziz, Y Hamdioglu, I Karasay, B Uguz, Intramuscular Haemangioma of the masseter muscle in a 9 year old girl.Acta Angiol 2007 13(1):42-46. [Google Scholar]
[6]. V Jain, N Bahri, HP Parekh, SS Mody, Intramuscular haemangioma of the masseter: Erectile haemangiomaInternational Journal of Head and Neck Surgery 2011 2(3):169-71. [Google Scholar]
[7]. AZ Zengin, P Celenk, AP Sumer, Intramuscular haemangioma presenting with multiple phleboliths: a case report.Oral Surg Oral Med Oral Pathol Oral Radiol 2013 115:32-36. [Google Scholar]