Primary Subcutaneous Inguinal Hydatid Cyst: Diagnosis by Fine Needle Aspiration Cytology
Permeet Kaur Bagga1, Satish Kumar Bhargava2, Neema Aggarwal3, Yogesh Chander4
1 Associate Professor, Department of Pathology, Government Medical College, Amritsar, India.
2 Professor and Head, Department of Radiology, School of Medical Sciences & Research and Sharda Hospital, Sharda University, Greater Noida, U.P, India.
3 Assistant Professor, Department of Radiology, School of Medical Sciences & Research and Sharda Hospital, Sharda University, Greater Noida, U.P, India.
4 Professor & Head, Department of Microbiology, School of Medical Sciences & Research and Sharda Hospital, Sharda University, Greater Noida, U.P, India.
NAME, ADDRESS, E-MAIL ID OF THE CORRESPONDING AUTHOR: Dr. Permeet Kaur Bagga, Associate Professor, Department of Pathology, Government Medical College, Amritsar, Punjab, India.
Phone: 8146479004,
E-mail: permeetbagga18@yahoo.co.in
Hydatid disease or human cystic echinococcosis, recognized by ancient scholars such as Hippocrates, Galen and Rhazes, is one of the oldest diseases known to man. Though hydatid cyst may develop in almost any part of the body, a solitary primary subcutaneous localization is an extremely rare entity. We herein report a case of primary subcutaneous inguinal hydatid cyst which was diagnosed by fine needle aspiration cytology. Radiological examination done subsequently corroborated with the cytodiagnosis of Hydatid cyst and did not show involvement of any other organ or site. Histopathological examination of surgically removed cyst confirmed the diagnosis of Hydatid cyst. Hydatid disease should be considered in the differential diagnosis of all unusual swellings in soft tissues, especially in regions where the disease is endemic.
Cytology, Echinococcosis, Hydatid, Primary, Subcutaneous
Case Report
A 33-year-old male reported to Surgery Department of our institute which is a tertiary care centre in northern India, about two years ago. His chief complaint was a painless swelling in the left inguinal region which was gradually increasing in size for the last eight months. There was no history of trauma, fever or weight loss. On physical examination, a non-tender, soft, irreducible swelling of about 4x3 cm in the left inguinal region was present. It was inert, non inflammatory cystic mass. The overlying skin was normal [Table/Fig-1].
Patient having swelling in left inguinal region

General physical examination, liver profile and other laboratory tests revealed no abnormality. Chest X-ray and Ultrasonography of the abdomen were normal. The patient was referred to Cytopathology Department for FNAC without prior clinical suspicion of hydatid disease.
The swelling was aspirated under palpation by trained Cytopathologist using 25 gauze needles. FNA done yielded about 10ml of clear, watery fluid and swelling decreased in size. Smears prepared from the centrifuged deposits of fluid were stained with May Grunwald Giemsa (MGG) and Hematoxylin & Eosin (H&E) stain. Few smears were left unstained for any special stain if required subsequently.
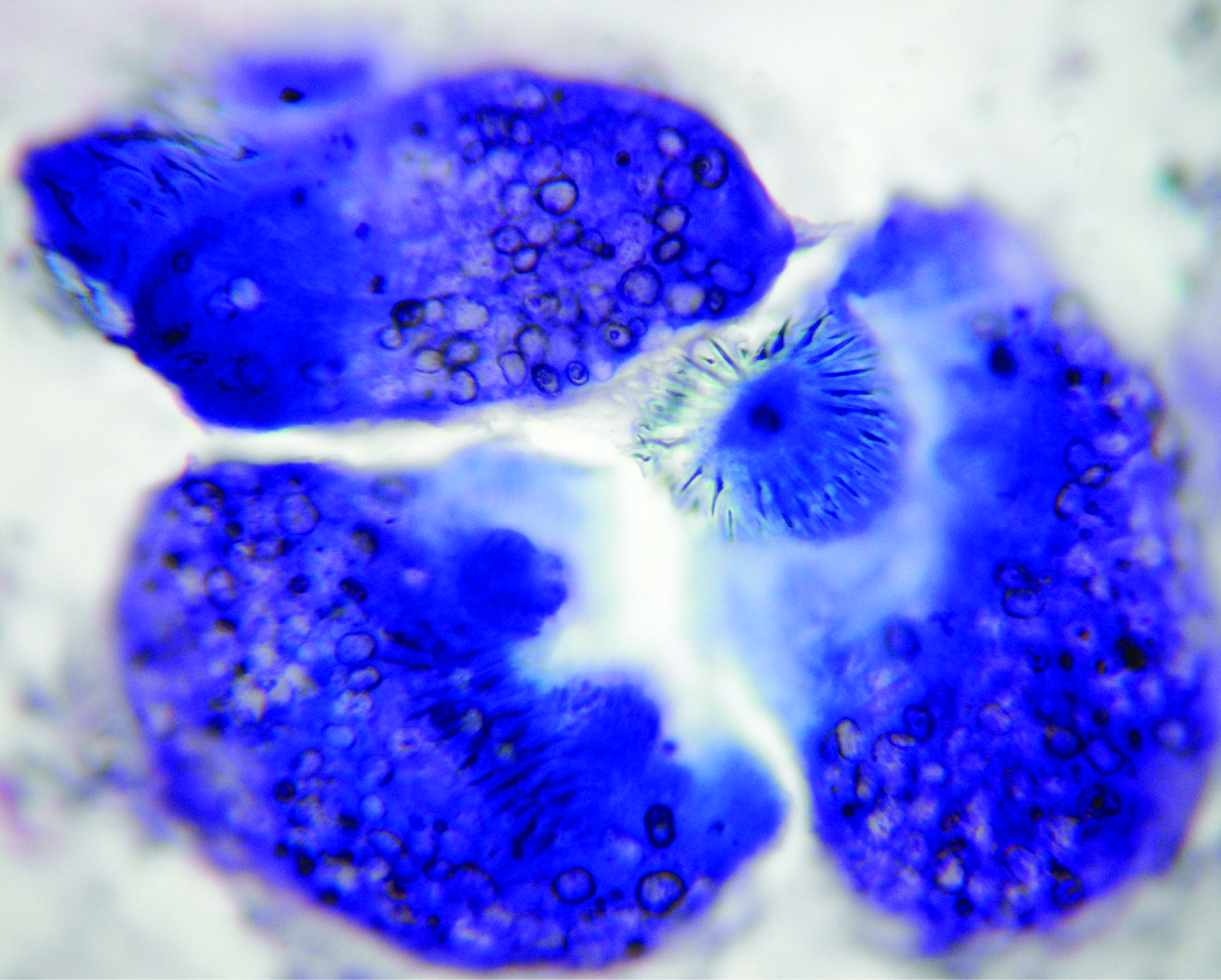
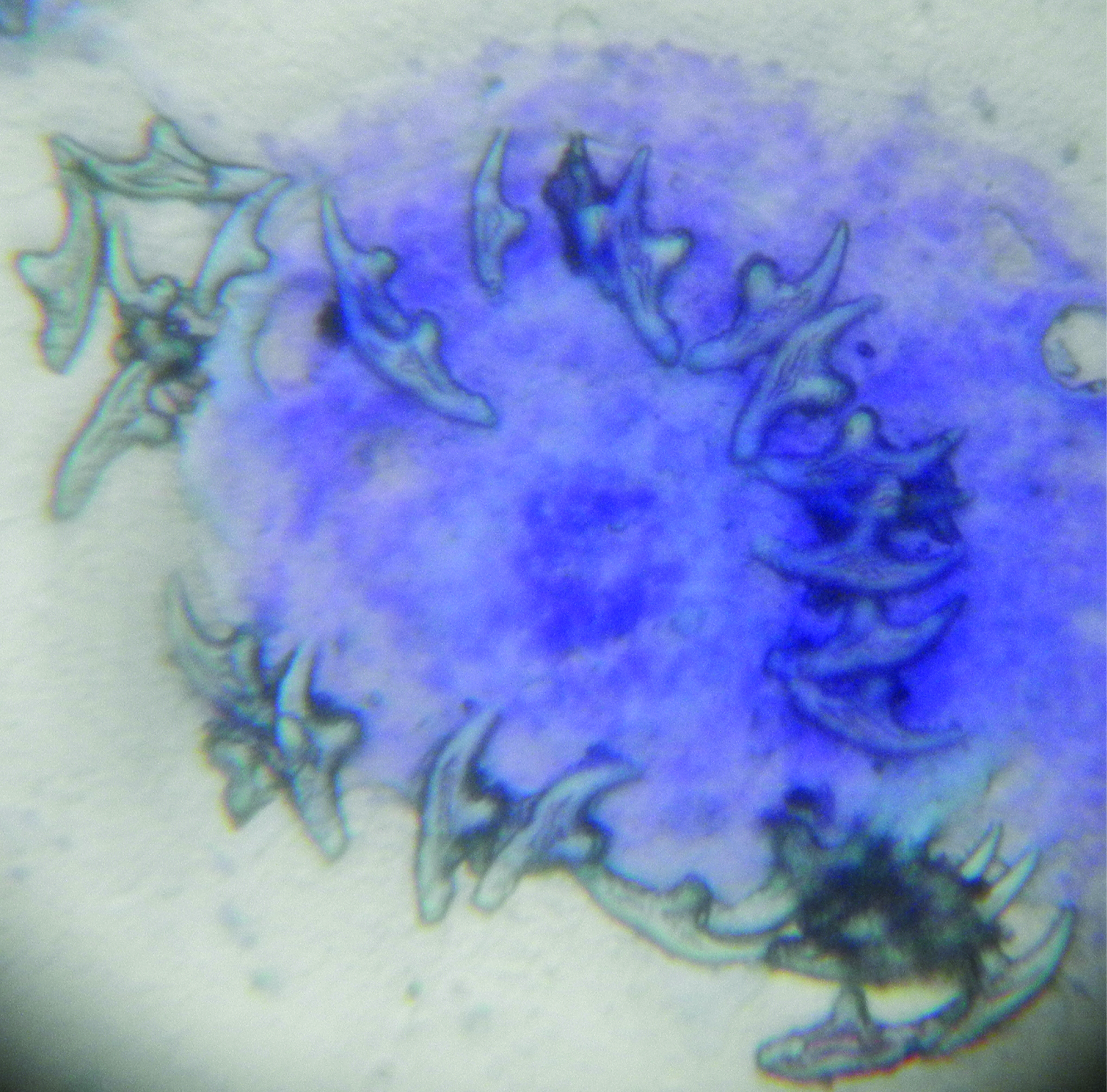
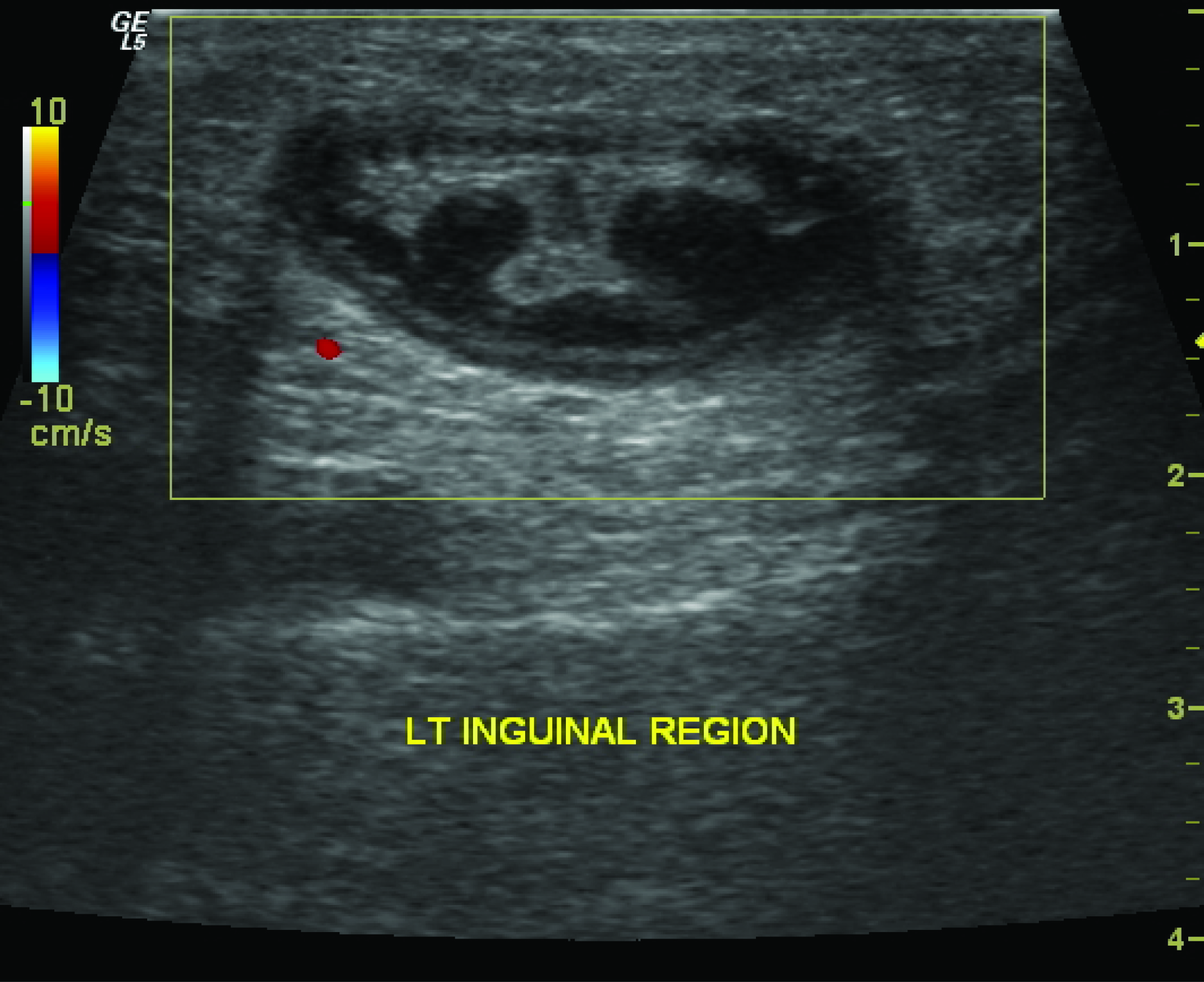
Microscopic examination of the smears demonstrated many scolices with attached hooklets along with scattered hooklets and inflammatory cells in the background. [Table/Fig-2,3] Fragments of acellular material with delicate parallel striations representing remnants of laminated membranes were also present. PAS stain done subsequently demonstrated clearly delicate, parallel laminations of the membrane. So on Fine Needle Aspiration Cytology, the diagnosis of hydatid disease was made. Ultrasonography of the swelling done subsequently showed a well-defined, ovoid, thick walled cystic lesion measuring 3.5 x 1.8 cm with posterior acoustic enhancement, in the subcutaneous plane of left inguinal region. The lesion was around 3mm deep from the skin surface and superficial to the muscular plane. It showed floating collapsed membranes within. No calcification was evident [Table/Fig-4].
Photomicrograph showing scolices with hooklets (MGG,X400)
Photomicrograph showing scolex with hooklets (MGG,X400
USG- cyst with floating membranes
Clinical and radiological examination done subsequently to look for evidence of hydatid disease in other organs, did not show involvement of any other organ or site. The patient also did not give any past history of hydatid cyst in any other organ. So final diagnosis of primary subcutaneous Hydatid cyst of inguinal region was made. As typical features of Hydatid disease were present on cytology and later corroborated by radiology, so serological tests which are expensive tests with low diagnostic sensitivity and specificity, were not done
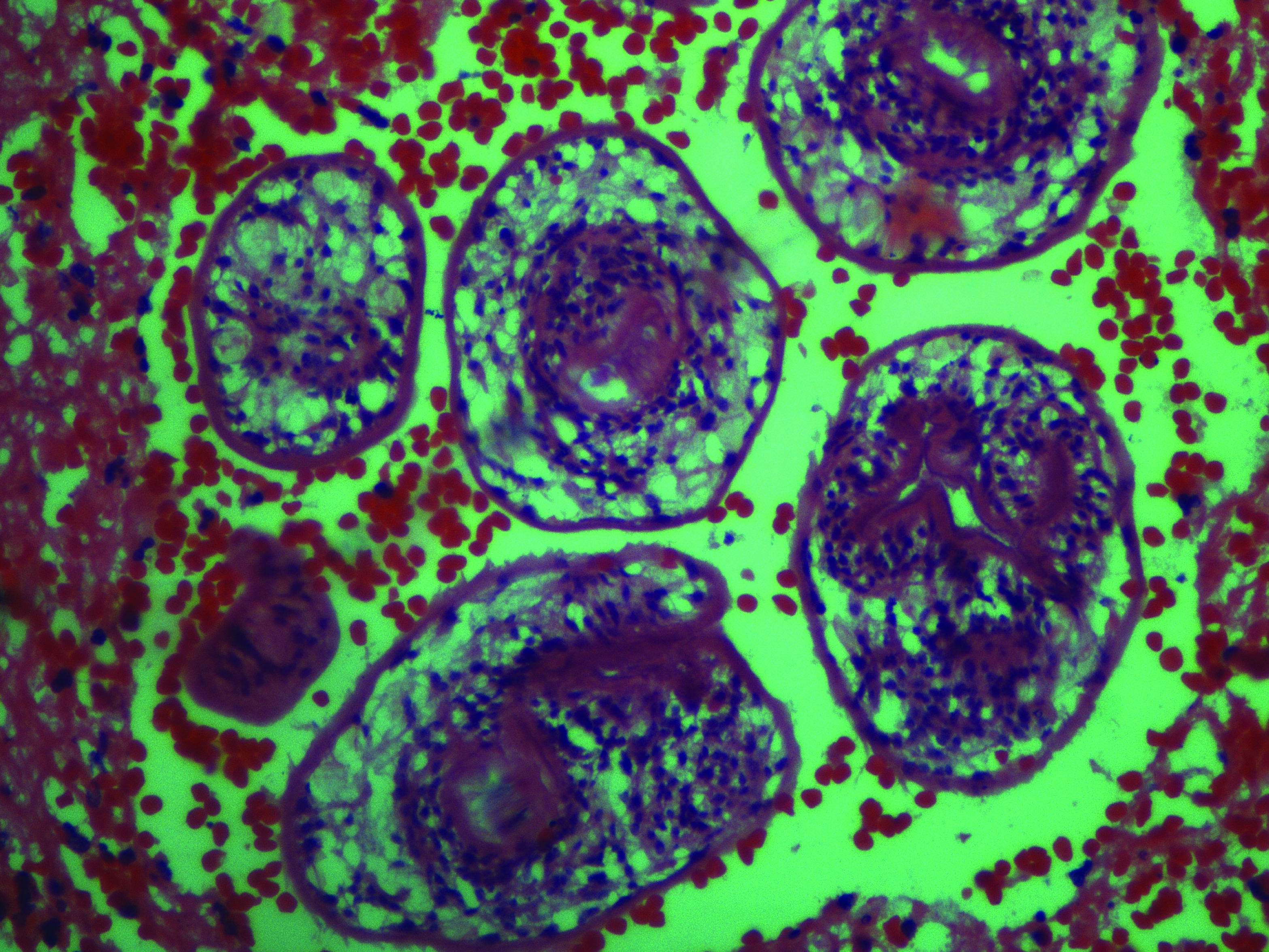
Histopathological examination of surgically removed cyst confirmed our diagnosis [Table/Fig-5]. Our patient received perioperative adjuvant antihelminthic treatment with albendazole. Our patient did not have any adverse reaction during the diagnostic and therapeutic procedure. The patient was followed up for one year and no recurrence of hydatidosis had been detected.
USG- cyst with floating membranes
Discussion
Hydatid disease or human cystic echinococcosis is a parasitic infestation caused in majority of cases by Echinococcus granulosus and multilocularis. The definite host is dog. Intermediate hosts are sheep, goat and cattle. Humans are the coincidental intermediate hosts. The liver is the most frequently involved organ(75%) followed by lungs(15%) although hydatid cyst may develop in almost any part of the body, including soft tissues [1,2]. Musculoskeletal or soft tissue hydatidosis account for about 0.5% to 5.0% of all echinococcal infections in endemic areas [1,3]. The frequency of subcutaneous tissue involvement associated with involvement of other solid organs, has been reported to be approximately 2% [4]. A solitary primary subcutaneous localization is an extremely rare entity, even in countries where the echinococcus infestation is endemic [4–7] and real incidence is not known.
The mechanism of primary subcutaneous localization of hydatid cyst is still not clear. The ingested parasite larvae penetrate the intestinal wall, enter the circulation and via portal vein reach the liver, where most of them are caught in the hepatic sinusoids. Few may pass through the liver( first filter) and reach the lung (second filter) and systemic circulation, causing hydatid disease in other organs and sites. Dissemination through lymphatic channels has also been suggested as a possible mechanism and accounting for cases with solitary cysts in uncommon sites [2]. Another mechanism may be direct spread from adjacent sites [8].
In cases with atypical locations, the clinical findings are also non-specific and depend on the site of involvement and size of the cyst. Usually it presents as painless, non-inflammatory, slow growing soft tissue masses which may mimic other pathological conditions such as soft tissue tumours in some cases [9]. In these cases, FNAC may be used for initial evaluation of such lesions, as was done in the present case. Radiological investigations (USG, CT & MRI) are useful in rendering diagnosis by demonstrating characteristic appearance of unilocular or multilocular cysts, showing the size, localization, relationship to adjacent tissues and to look for evidence of hydatid disease in other locations [8].
The diagnosis of hydatid disease can be supplemented by various serological tests which have replaced the Casoni’s test. However, all serological tests have low diagnostic sensitivity and specificity. These serological tests are complementary to pathological and radiological tests and if on cytology and radiology characteristic features of hydatid cyst are present, then serological tests may not be done ,especially in developing countries where they are expensive tests and not readily available in all diagnostic centers. In our case also, typical features of hydatid disease were present on cytology and later corroborated by radiology, so serological tests were not done and surgical excision of the cyst was done.
Preoperative diagnosis is important because of the risk of cyst rupture during the treatment. Contamination of surrounding tissues with the cyst contents may cause local recurrence or anaphylaxis.
Amongst all the hydatid cyst cases involving any organ, subjected to FNAC and described in literature, only occasional adverse reactions like anaphylactic reactions and infection of the cysts have been reported [10,11]. In a study in which 22 cases of primary subcutaneous hydatid cysts were reviewed, no anaphylaxis or recurrences were reported [12]. Our patient also did not have any adverse reaction during the diagnostic and therapeutic procedure.
The best treatment option is complete surgical excision of the intact cyst which avoids leakage of cyst contents. If it is not possible, the cyst contents can be removed intraoperatively and the cyst pouch irrigated with scolicidal solutions. The combination of adjunctive chemotherapy with antihelminthics pre and post operatively is also recommended to cover the risk of dissemination [1,4]. Our patient also received perioperative adjuvant antihelminthic treatment with albendazole.
Conclusion
Mostly hydatid cyst can be diagnosed on the basis of clinical history and imaging findings. However, when it is present in atypical locations, the diagnosis can be challenging. Hydatid disease should be considered in the differential diagnosis of every subcutaneous cystic mass, especially in areas where the disease in endemic. FNAC in collaboration with radiological investigations is very useful in the preoperative diagnosis of such clinically unsuspected hydatid cysts in atypical locations.
[1]. Dirican A, Unal B, Kayaalp C, Kirimlioglu V, Subcutaneous hydatid cysts occuring in the palm and the thigh: two case reportsJ Med Case Rep 2008 2:273 [Google Scholar]
[2]. Ok E, Sozuer EM, Solitary subcutaneous hydatid cyst: a case reportAm J Trop Med Hyg 2000 62:583-84. [Google Scholar]
[3]. Karaman E, Yilmaz M, Ada M, Yilmaz RS, Isildak H, Unusual location of primary hydatid cyst: soft tissue mass in the parapharyngeal regionDysphagia 2011 26(1):75-77. [Google Scholar]
[4]. Ousadden A, Elbouhaddouti H, Ibnmajdoub KH, Mazaz K, Taleb KA, A solitary primary subcutaneous hydatid cyst in the abdominal wall of a 70-year- old woman: a case reportJ Med Case Rep 2011 5:270 [Google Scholar]
[5]. Mirzaei T, Hooshyar H, Primary Subcutaneous Hydatid Cyst in ScapulaIran J Pathol 2012 7(4):259-61. [Google Scholar]
[6]. Olmez A, Itik V, Aydin C, Kayaalp C, Primary Subcutaneous Hydatid cyst at the flank: A case reportEur J Surg Sci 2010 1(3):93-95. [Google Scholar]
[7]. Burgazli KM, Ozdemir CS, Ozdemir EB, Mericliler M, Polat ZP, Unusual localization of a primary hydatid cyst: a subcutaneous mass in the paraumbilical regionEur Rev Med Pharmacol Sci 2013 17(13):1766-68. [Google Scholar]
[8]. Safioleas M, Nikiteas N, Stamatakos M, Safioleas C, Manti CH, Revenas C, Echinococcal cyst of the subcutaneous tissue: a rare case reportParasitol Int 2008 57(2):236-38. [Google Scholar]
[9]. Basarir K, Saglik Y, Yildiz Y, Yetis T, Cebesoy O, Primary muscular hydatidosis mimicking soft tissue tumour: a report of five casesJ Orthop Surg 2008 16(3):368-72. [Google Scholar]
[10]. Agarwal PK, Husain N, Singh BN, Cytology findings in aspirated hydatid fluidActa Cytol 1989 33:138-40. [Google Scholar]
[11]. Yue X, LiuX LoS, Fine needle aspiration biopsy resulting in a local anaphylactic reactionActa Cytol 1987 :31-84. [Google Scholar]
[12]. Kayaalp C, Dirican A, Aydin C, Primary subcutaneous hydatid cysts: a review of 22 casesInt J Surgery 2010 9(2):117-21. [Google Scholar]