Dental caries has afflicted mankind, since the prehistoric era; however, its’ incidence is said to have increased in modern times [1].
The pit and fissure area is especially susceptible to caries as it is inaccessible to oral hygiene aids and provides a safe haven to microbes [2,3]. The closed nature of caries process following remineralisation may lead to sub-surface spread of the lesion.
The emergence of higher prevalence of non-cavitated lesions, due to preventive measures led to development of detailed visual indices; which recorded early visible signs of carious process e.g. opacities, micro-cavity etc [2]. The international caries assessment and detection system –II (ICDAS -II) index has been extensively used for caries detection and has been shown to have excellent correlation with lesion histopathology [4].
While visual examination alone has been advocated for caries detection; visual-tactile assessment is preferred by most clinicians, as tactile assessment is said to be an important criteria in determining lesion activity [5]. The WHO recommended the use of community periodontal index- treatment needs (CPI- TN) probe for caries detection [6].
Hence, this study aims to assess the impact of low level magnification in the form of loupes (1.8x) and dental operating microscope (3.4x) on the detection of incipient caries and its impact on restorative decision making.
Methodology
This study was conducted in the Department of Conservative Dentistry and Endodontics and Department of Oral Pathology in a Dental college in Karnataka, India over duration of six months.
Specimen Preparation
A total of 60 extracted human molars and premolars were selected. Any tooth damaged during extraction or those having large occlusal, buccal, lingual or proximal caries/ restoration were excluded. Ethical clearance was obtained from the university institutional review board for the use of teeth extracted for periodontal / orthodontic reasons (2010/5/2). The extracted teeth were placed overnight in 1 % sodium hypochlorite to prevent cross infection. The teeth were then hand scaled and polished using pumice and a polishing brush (KENDA Slimline polish, Vadus, Liechtenstein) prior to use in order to remove extrinsic stains, calculus and debris. Following this they were rinsed using a 3- way syringe and occlusal surface was dried for 10 seconds using air pressure, to remove any pumice from within the fissures. They were stored in saturated Thymol (VDH organics Ltd., Ghaziabad, India) solution, until used for the study.
Digital images of the occlusal surface of the samples were captured at 5x magnification (Canon IXUS, Tokyo, Japan). An experienced dentist, not involved with the experimental procedure was asked to mark the site, which was to be examined on the image. The sites were selected as being a reflection of changes in the appearance of enamel from apparently sound surface to those with discoloration. The marking of the site on a photograph allows for the same location being examined by each operator, while not aiding in the detection of caries.
The teeth and photographs were numbered to avoid confusion. Two operators were asked to assess each sample using three different techniques.
Visual- Tactile Examination (unenhanced)
Enhanced visual –tactile examination using loupes at 1.8x (shiLED,ohio, USA)
Enhanced visual –tactile examination using surgical operating microscope (SOM) at 3.4x (OPMIpico Carl Zeiss,Oberkochen, Germany)
Examiners were asked to assess the visual changes using modified ICDAS –II. On a scale of 0 - 4. In order to familiarise the observers with ICDAS- II index examiner calibration was carried out.
Examiner Callibration
A presentation was held regarding ICDAS–II index, details of each score were discussed and a series of images were displayed corresponding with each score to demonstrate the small and subtle changes between them. Four teeth (not included in the study with different ICDAS –II scores were then assessed by each examiner to allow for calibration).
There was no training in the use of magnification as the examiners were familiar with it for clinical procedures performed routinely by them.
A patient model was proposed keeping in mind that treatment decision making depends on patient factors like oral hygiene, DMFT index etc. The proposed model for this study was that of an urban teenager, with good oral hygiene and DMFT less than three.
Specimen Examination
Each observer examined the teeth in similar surroundings using a dental unit light (Confident Dental, Bangalore, India), a 3-way syringe, CPI- TN probe (Hu Friedy, Chicago, USA). The teeth were examined at a standard tooth to eye distance of 32 cm, using loupes at 1.8x and SOM at 3.4x. The examiners assessed each specimen blinded to the others findings.
The first round of testing was done using unenhanced visual-tactile technique. The examiners were asked to note visual findings as per the modified ICDAS score [Table/Fig-1].
International caries assessment and detection system (ICDAS-II)
| Score | Presentation |
|---|
| 0 | Sound tooth surface; no evidence of caries after prolonged air drying. |
| 1 | First visual change in enamel;opacity or discoloration visible at entrance to pit and fissure after prolonged air drying. |
| 2 | Distinct visual change in enamel visible when wet, lesion must be visible when dry. |
| 3 | Localized enamel breakdown (without clinical visual signs of dentinal involvement) seen when wet and after prolonged drying. |
| 4 | Underlying dark shadow from dentine. |
| Score | Presentation |
|---|
| 0 | No enamel demineralization or edge effect |
| 1 | Enamel demineralization limited to the outer 50% of the enamel surface |
| 2 | Demineralisation involving between 50% of the enamel and outer 1/3 of the dentin |
| 3 | Demineralization involving the middle third of the dentin |
| 4 | Demineralization involving the inner third of the dentin |
Tactile findings were indicated as
0- No abnormality detected
1- Presence of roughness /presence of catch/ depression
2- Presence of softness
Based on visual-tactile assessment, they were asked to state whether caries was present (1) or absent (0); further they were asked to indicate appropriate treatment modality for each lesion;
No Treatment Required (NT) - 0
Preventive Treatment (PT) - 1
Restorative Treatment (RT) – 2
The specimens were stored in distilled water between examinations.
The examination of all 60 teeth was repeated using loupes at 1.8x after two days. Following which the teeth were examined using SOM at 3.5x, after another two days. The teeth were randomized at each examination. The time gap of two days between successive examinations was introduced to reduce observer bias.
After one week 50% (n=30) of extracted teeth were selected randomly and re-examined using each technique, following the pattern of the first round of examination to assess intra-examiner reproducibility.
Following which, the teeth were resected just apical to cement-enamel junction (CEJ). The crowns were then hemi sectioned through the area of examination using a diamond disk at slow speed (Diamant, Horico, New Jersey,USA). Both sections were then examined and the part with the most extensive changes was selected. The selected section was ground to 1 mm thick slice. These were observed at regular intervals to ensure that caries lesion was not ground away. The disk was replaced after every two specimens to ensure uniformity.
Histological Examination
The sections were stored in distilled water for 24 hrs to permit rehydration. The depth of enamel demineralisation represented by greatest area of discoloration was assessed on wet sections. The depth of dentin demineralisation was measured at the area where colour changed from yellowish to grey along a line at 90o to DEJ towards the pulp.
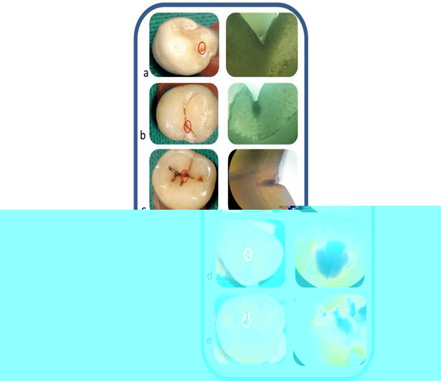
The wet sections were observed under a stereomicroscope (AxMx, Lawrence and Mayo, Bengaluru, India) by an experienced oral pathologist at 5x magnification and the changes were assessed using Ekstrands’ criteria [Table/Fig-3] [14].
Shows the occlusal surface of teeth with incipient carious changes, with site of examination marked on the picture and the corresponding histopathologic picture arranged in ascending order of Ekstrands’ criteria
Statistical Analysis
Inter and intra- examiner agreement was measured using Kappa statistics for each detection method and treatment decisions [Table/Fig-4,5].
Kappa values for intra and inter examiner reproducibility for treatment decision making using (unaided, Loupes and microscope techniques) different techniques.
| Diagnostic Aids | Intra- Examiner Reproducibility | Inter- Examiner Reproducibility |
|---|
| Examiner A | Examiner B | Examiner A - B |
|---|
| Unaided | 0.44 | 0.44 | 0.40 |
| Loupes | 0.50 | 0.67 | 0.51 |
| microscope | 0.55 | 0.75 | 0.63 |
Kappa values for intra and inter examiner reproducibility for caries diagnosis using (unaided, Loupes and microscope techniques) different detection techniques
| Diagnostic Aids | Intra- Examiner Reproducibility | Inter- Examiner Reproducibility |
|---|
| Examiner A | Examiner B | Examiner A - B |
|---|
| Unaided | 0.72 | 0.54 | 0.46 |
| Loupes | 0.53 | 0.40 | 0.46 |
| Microscope | 0.67 | 0.74 | 0.63 |
Sensitivity, specificity and likelihood ratios (LR+ and LR-) for a positive and negative test were calculated for both examiners with and without magnification. The above parameters were calculated at D1 diagnostic threshold (sound = no lesion; disease = all grades of disease). The McNemar test was used to compare sensitivity, specificity and likelihood ratios between examiners and examinations.
The degree of agreement of each examiner using different techniques with histological status was done via ROC statistics and the area under the curve was calculated. A non-parametric test in ROC statistics was used to assess the difference among Az values. The significance level for all the statistical tests was set at p < 0.05 the statistical analysis was performed using SPSS 16.0 software.
Results
The results regarding sensitivity, specificity and likelihood ratios for a positive and negative test per examiner with and without magnification at D1 threshold are illustrated in [Table/Fig-6]. The use of loupes was associated with lower sensitivity by one examiner, who also showed a markedly high likelihood ratio (LR) for the same. The Az value for both operators was higher for use of microscope.
Sensitivity, specificity, likelihood ratio and az value per examiner
| Value to be measured | Visual -Tactile | Loupes | Microscope |
|---|
| A | B | A | B | A | B |
|---|
| SENSITIVITY | 0.67 | 0.71 | 0.65 | O.42 * | 0.75 | 0.71 |
| SPECIFICITY | 0.73 | 0.72 | 0.61 | 0.9* | 0.68 | 0.69 |
| LR+ | 2.5 | 2.5 | 1.69 | 13.7* | 2.4 | 2,28 |
| LR- | 0.45 | 0.39 | 0.56 | 0.59* | 0.36 | 0.41 |
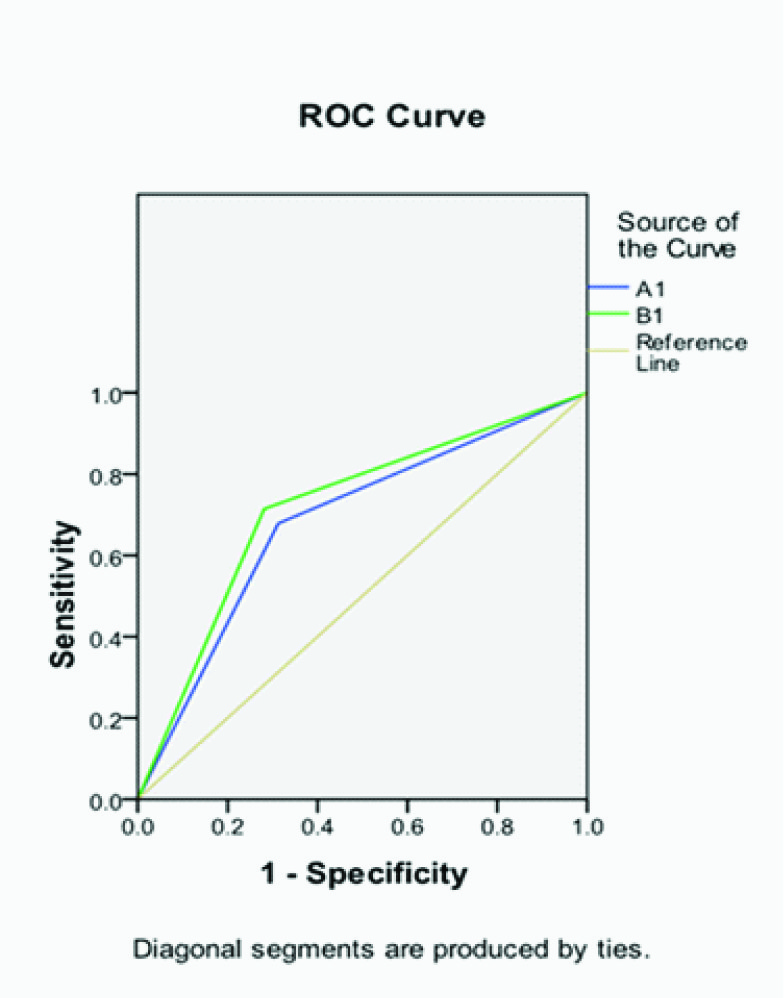
| Az | 0.683+/ 0.007* | 0.717+/ 0.006* | 0.636+/ 0.07* | 0.699+/ 0.07* | 0.719+/ 0.06* | 0.701+/ 0.07* |
| CI | 0.55- 0.82 | 0.58-0.85 | 0.49- 0.78 | 0.56 – 0.84 | 0.58-0.85 | 0.56-0.84 |
LR - Likelihood Ratio
Az – Area Under The Curve
A - Examiner A, B - Examiner B
Discussion
The diagnosis of caries is unique in that it is lacking the hypothetico-deductive reasoning [15]. Rather it is based on experiences of an individual, hence forming a caries script for cases encountered in the future. This highlights the subjective nature of occlusal caries detection [16,17].
In order to reduce interpretational bias, many visual indices were developed. The unaided implementation of ICDAS–II in various studies have led to diverging scientific data on reproducibility [4,13,18].
Surface texture is, an important criterion, for determining activity of the lesion and reaching an appropriate treatment decision.Unfortunately visual examination cannot assess surface texture, therefore, in the current study tactile criteria was adopted along with ICDAS-II. The CPI- TN probe was recommended by the WHO for caries detection as its blunt, rounded tip allows for better assessment of surface characteristics without causing surface defects [6,19].
Low level magnification was selected, as it is believed to be optimal for diagnosis, allowing for better visualisation and not compromising the width and depth of field of vision excessively. Both, these parameters are essential for appreciation of occlusal anatomy and to reach the correct diagnosis. Different magnification powers were chosen for loupes and microscope to allow for standard fixed distance between eye of the observer and the object.
Newer, exclusively diagnostic aids like Quantitative laser fluorescence (QLF), DIAGNOdent, electric resistance measurement have been introduced. These methods are based on differences in optical properties of demineralized and normal tissue, allowing for early caries detection. However, studies show no improvement with fluorescence over the use of ICDAS- II for initial caries detection [18].
Along, with an accurate detection, a correct treatment modality must be selected as unnecessary restorative treatment may reduce lifespan of the tooth, by premature entry of the tooth in the restoration cycle.
Histologic results were correlated with clinical picture. A diagnostic cut –off level of two on Ekstrands’ criteria was selected as indicative of presence of caries and restorative therapy. Previous studies have shown that in dentinal caries softness precedes discoloration [14] indicating that score three would lead to a high false negative result.
The values of intra and inter examiner reproducibility [Table/Fig-7] obtained in this study was lower than that derived in previous studies [11–13]. This may be attributed to the difference in histological cut-off and techniques used. The highest values for both inter and intra examiner reproducibility was obtained for SOM (0.63), compared to unenhanced visual–tactile and loupes. This could be attributed to coherent illumination provided by microscope that would allow for better visualisation of defects.
ROC curve for comparison of caries detection between the two examiners
Previous studies have reported that ICDAS index gives high level of specificity and magnification resulted in higher sensitivity than unenhanced detection [18]. The lower specificity noted in this study (comparatively) may be due to complexity of the groove-fossa system, which could lead to stain retention leading to false positive values. Differences in degree of magnification experience of examiners may lead to a variation in the level of sensitivity and specificity noted from earlier studies. Relatively lower values may also be due to histologic technique used, namely hemi-section, as it may lead to loss of peripheral lesion leading to inaccurate extent of caries being determined. An attempt was made to minimize this by examining the sections repeatedly as they were ground to ensure that the lesion was not lost during processing.
In the present study Az [Table/Fig-6] values for most observations were comparable to each other. No statistically significant difference was noted between the two examiners and various modalities.
Use of magnification for caries detection should always be done keeping in mind its inherent limitations like reduction in field and depth of vision. This study has attempted to circumvent this problem by using low level magnification.
Further studies are needed to compare enhanced vision with newer modalities like fluorescing devices to directly compare the relevance of both. In-vivo correlation of these in-vitro findings should be attempted.
Conclusion
Use of SOM showed marked improvement in inter-examiner reproducibility for caries detection and treatment decision making. Use of loupes was associated with lesser sensitivity, but higher specificity of caries detection. Within the limitations of this study, the results indicate that use of low level magnification would allow for easier and more reliable incipient caries detection.
LR - Likelihood Ratio
Az – Area Under The Curve
A - Examiner A, B - Examiner B