Non-Hodgkin’s Lymphoma in Buccal Vestibule -Case Report
Indira Reddy1, Sreenath G2, Raghavendra Reddy Y3, Ravi Prakash A4, Swathi T R5
1 Senior Lecturer, Department of Oral Pathology, G. Pullareddy Dental College, Andhra Pradesh, India.
2 Senior Lecturer, Department of Oral Pathology, G. Pullareddy Dental College, Andhra Pradesh, India.
3 Reader, Department of Oral Surgery, G. Pullareddy Dental College, Andhra Pradesh, India.
4 HOD, Department of Oral Pathology, G. Pullareddy Dental College, Andhra Pradesh, India.
5 P. G Student, Department of Oral Pathology, G. Pullareddy Dental College, Andhra Pradesh, India.
NAME, ADDRESS, E-MAIL ID OF THE CORRESPONDING AUTHOR: Dr. Swathi T R, G.Pulla Reddy Dental College, Kurnool
Phone: 08500213732,
E-mail: dr.swathivijay@gmail.com
Lymphomas are malignant neoplasms arising from lymphocytes B cell or T cell that affects mainly lymph nodes, spleen and other non hematopoietic tissues. They are classified as Hodgkin’s lymphoma (HL) and non-Hodgkin’s lymphoma (NHL). Diffuse large B-cell lymphoma (DLBL) is the most common variant of non-Hodgkin’s lymphomas and frequently involves extranodal sites. In the oral soft tissues lesions can occur as hard and diffuse tumors involving oral vestibule, gums and posterior region of the hard palate. Most lymphomas, including DLBL arise from B cells are characterized by diffuse population of large cells with cleaved or non cleaved oval nuclei. Both histopathlogical and immunohistochemical (IHC) analysis were strongly advisable for proper management and prognosis. We hereby report a rare case of Diffuse large B-cell variant of non-Hodgkin’s lymphoma in a male patient of age 50yrs in left upper buccal vestibule.
Buccal vestibule, Diffuse large B-cell lymphoma, Immunohistochemistry
Case Report
A 50-year-old male patient presented with a swelling and history of pain in the left upper back tooth region since two months. There was no contributory medical and family history. Patient did not reveal any habit of tobacco or betel nut chewing.
On extra oral examination revealed solitary swelling extending from the left infraorbital region to the ala of the nose which was measuring about 4x3cm with confined borders [Table/Fig-1]. The swelling was oval in shape, firm in consistency and freely movable with the overlying skin being normal. There was mild tenderness on palpation. The left submandibular lymph nodes were palpable and tender.
Clinical photograph showing swelling, clamping of the eye & deviation of the mouth to right
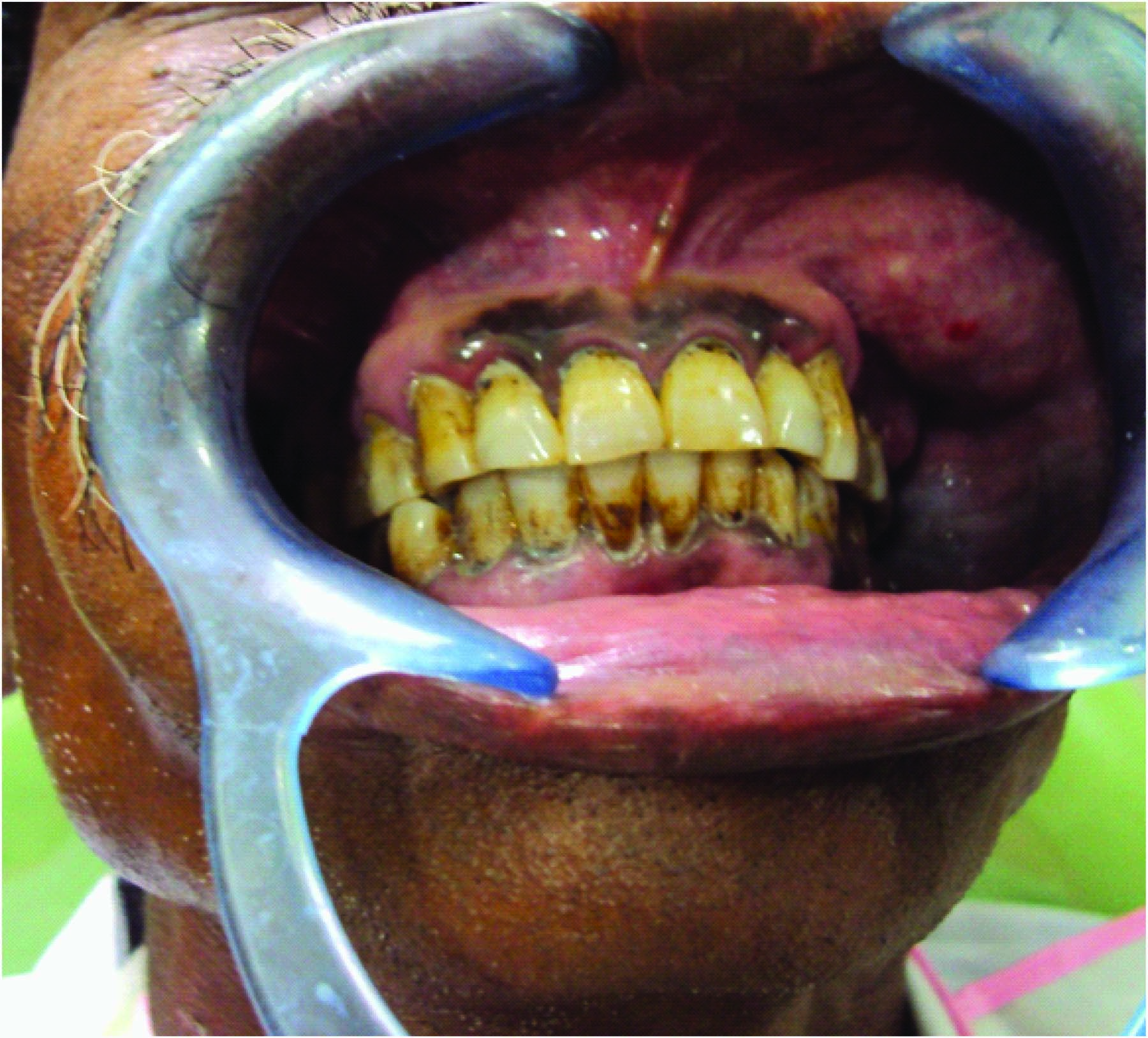
The intra oral examination revealed a swelling in the left upper buccal vestibule involving 24 & 25, measuring 3x2cm [Table/Fig-1]. The swelling was oval, firm in consistency, sessile, not fixed to the underlying structures, tender on palpation and the overlying mucosa was normal. The patient had a poor oral hygiene with grade I mobility of 24 & 25. The OPG is non contributory. Based on these clinical findings the provisional diagnosis was given as Fibroma and Lipoma.
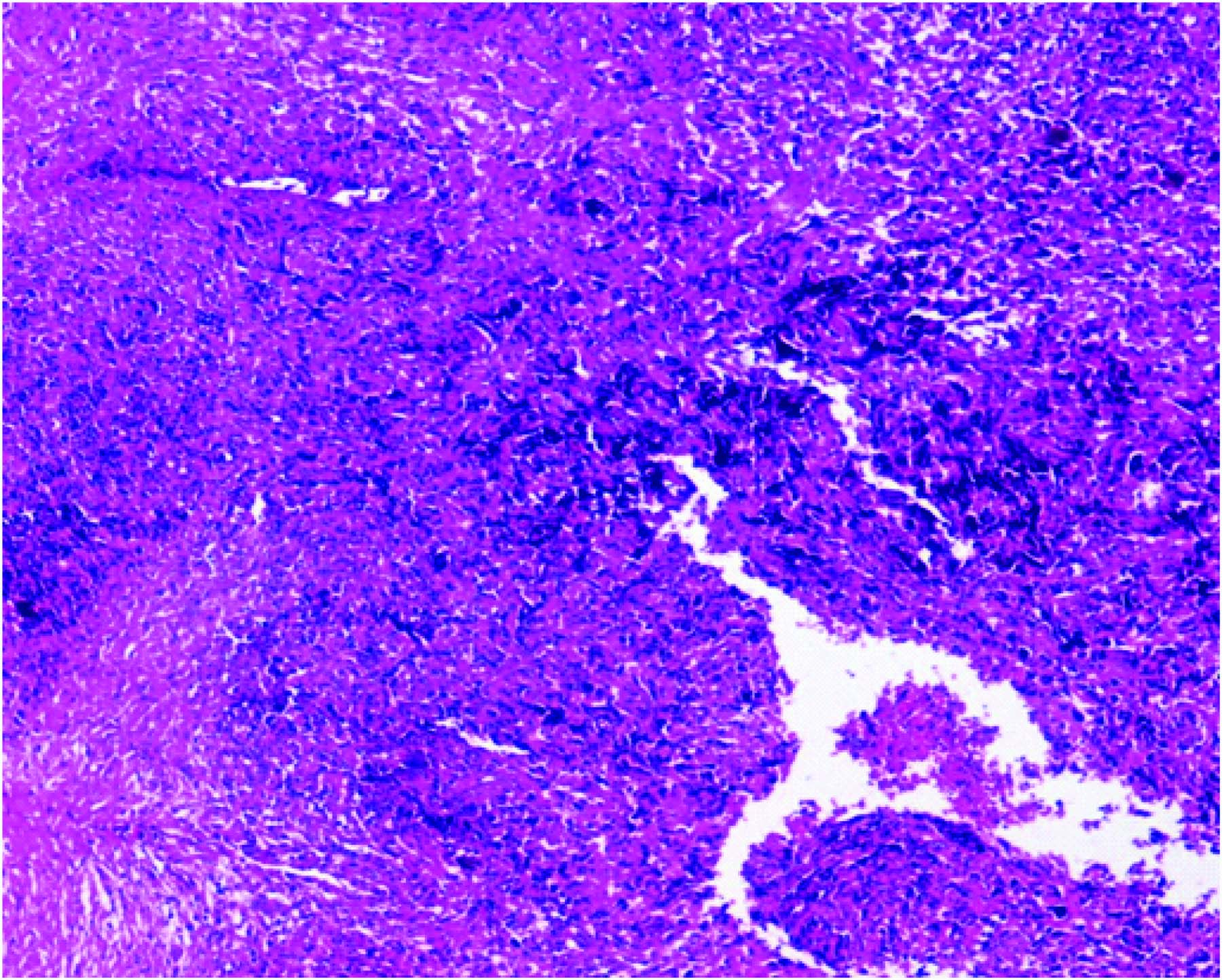
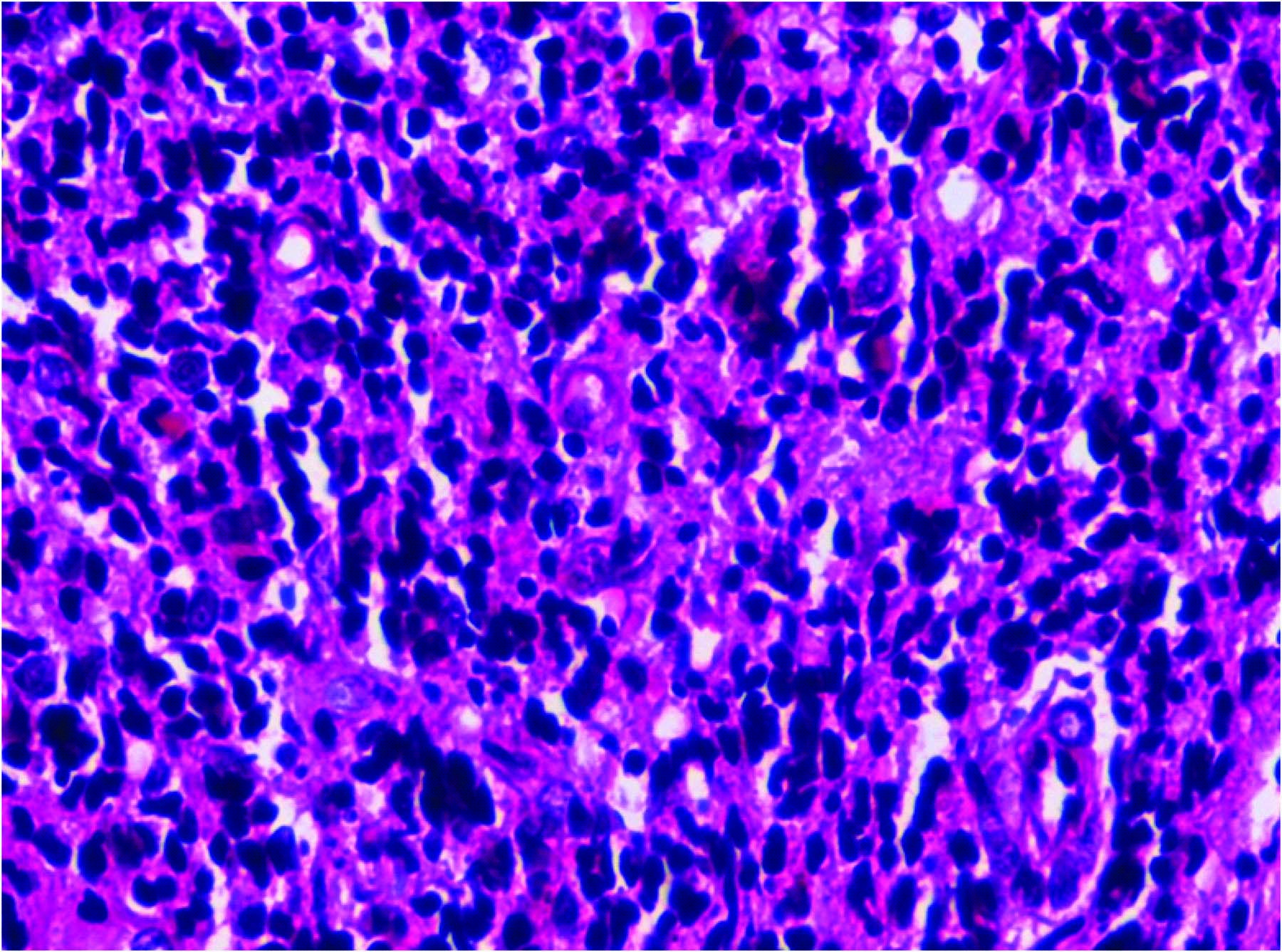
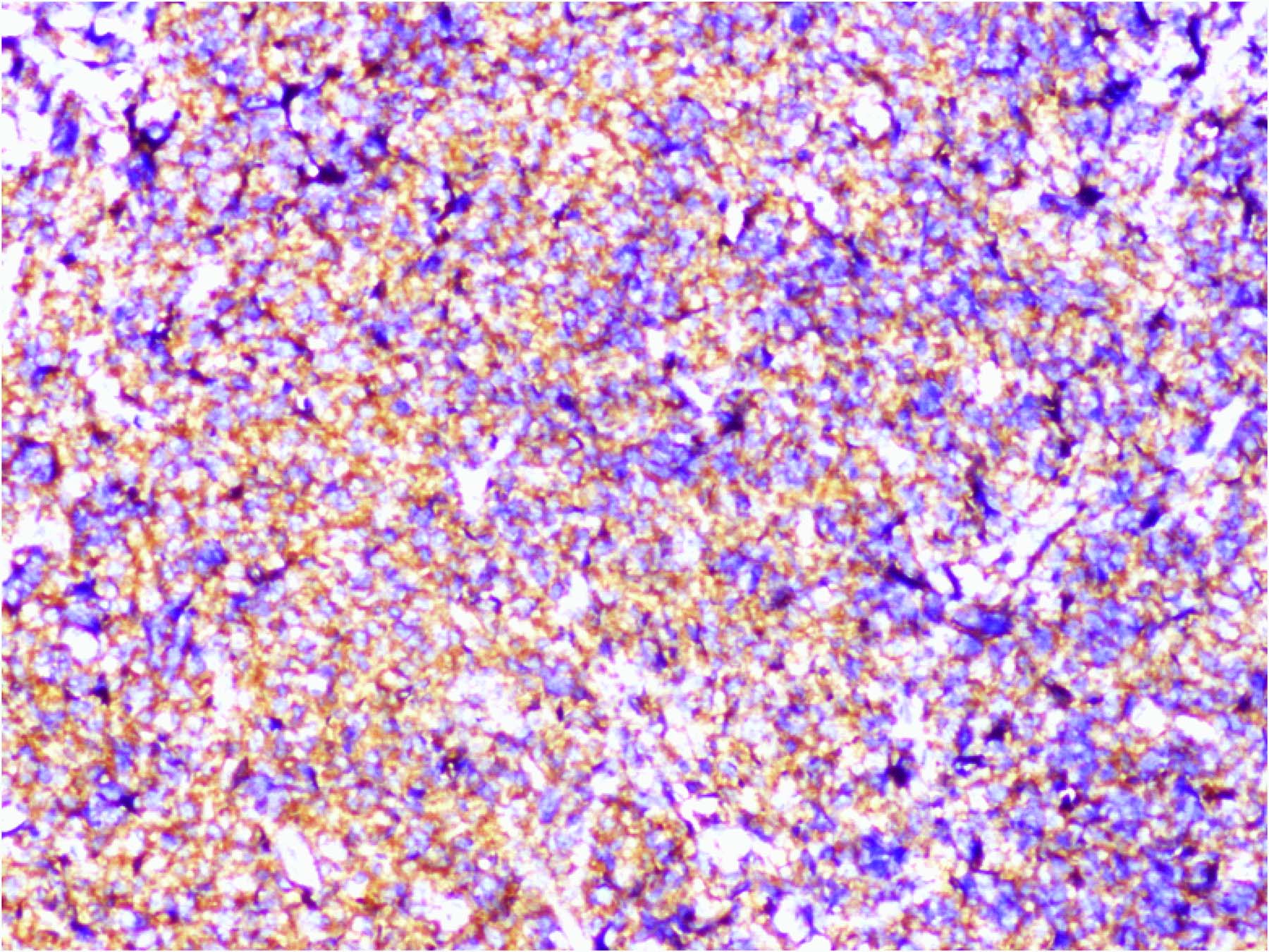
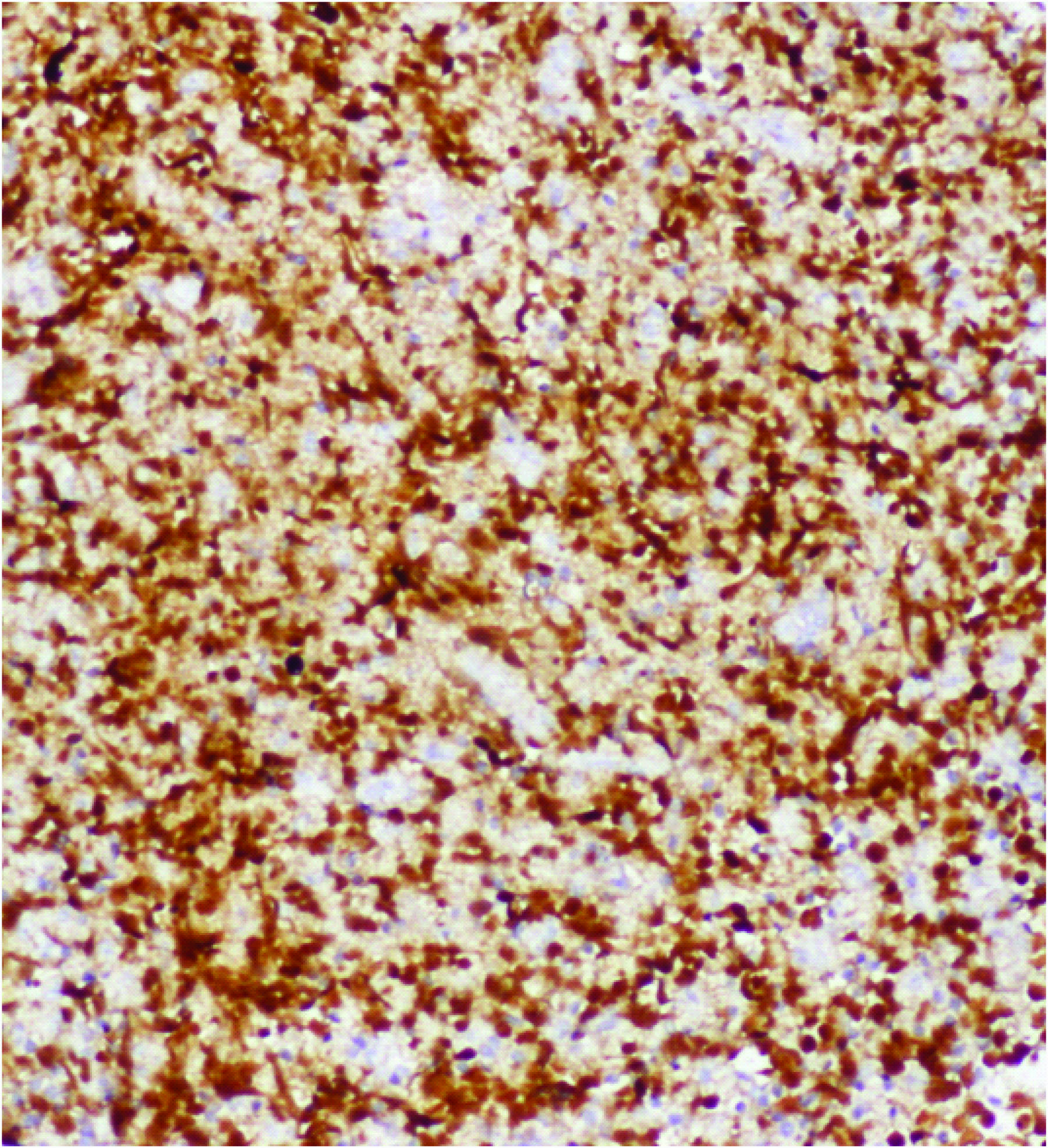
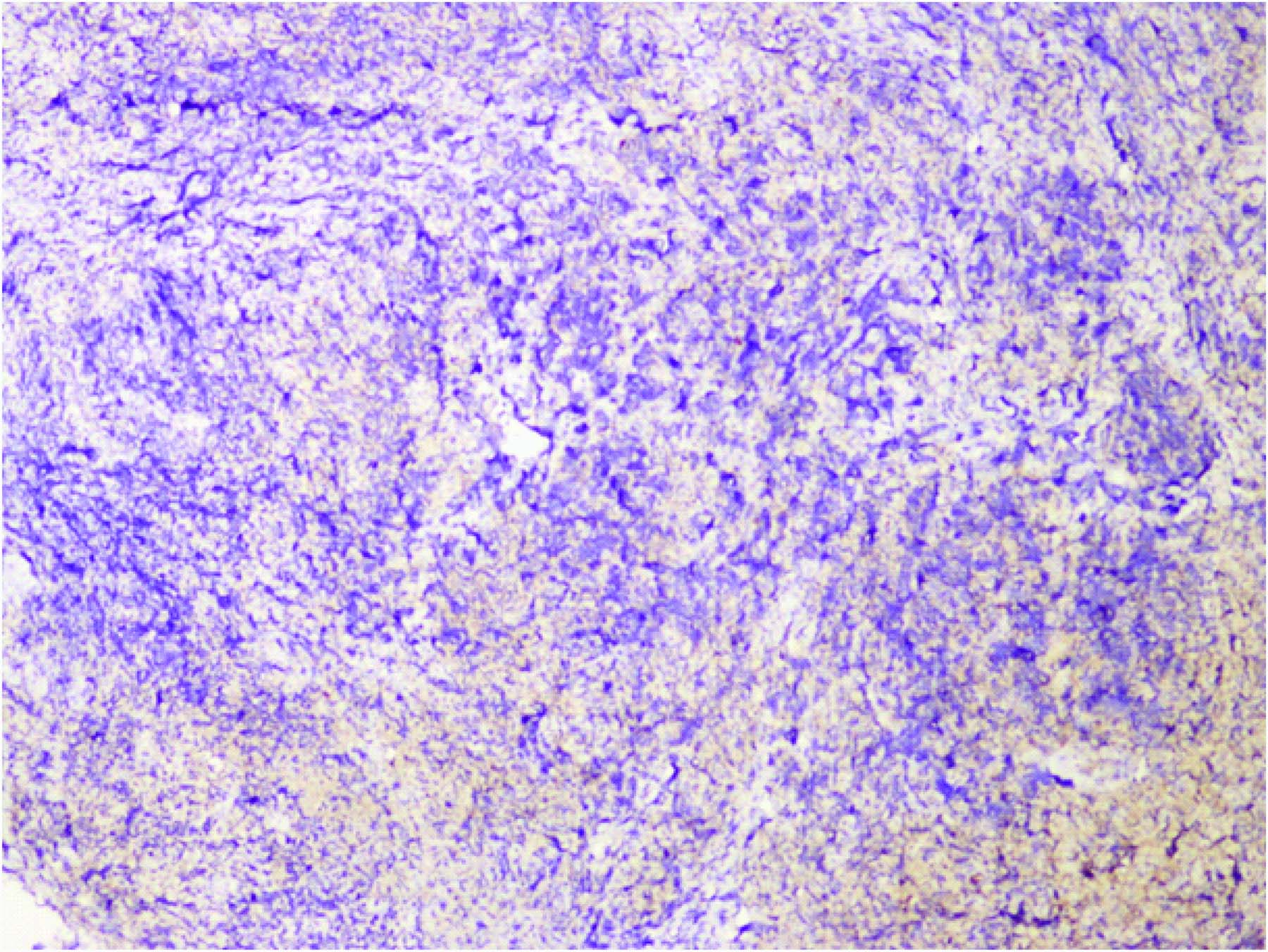
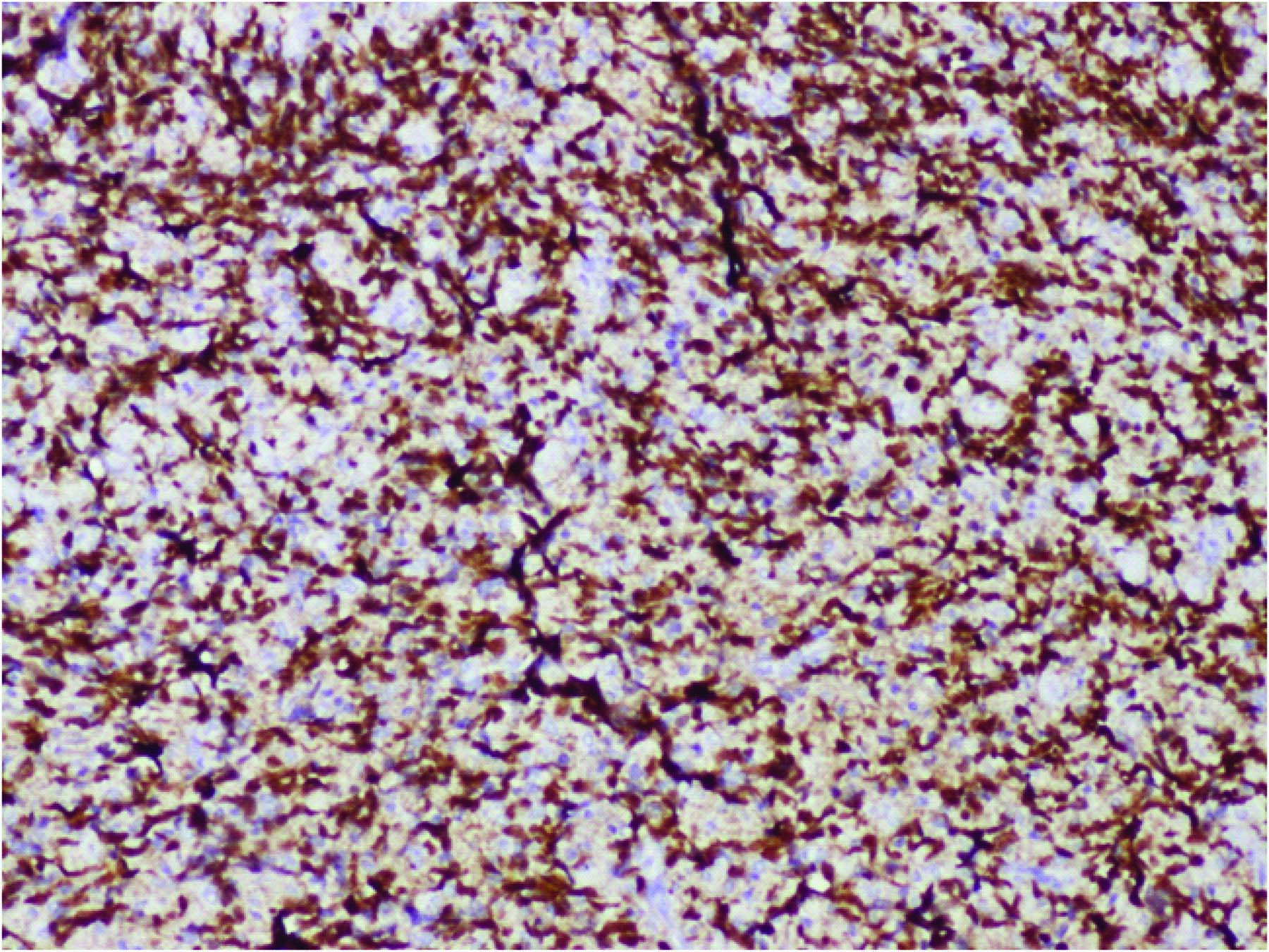
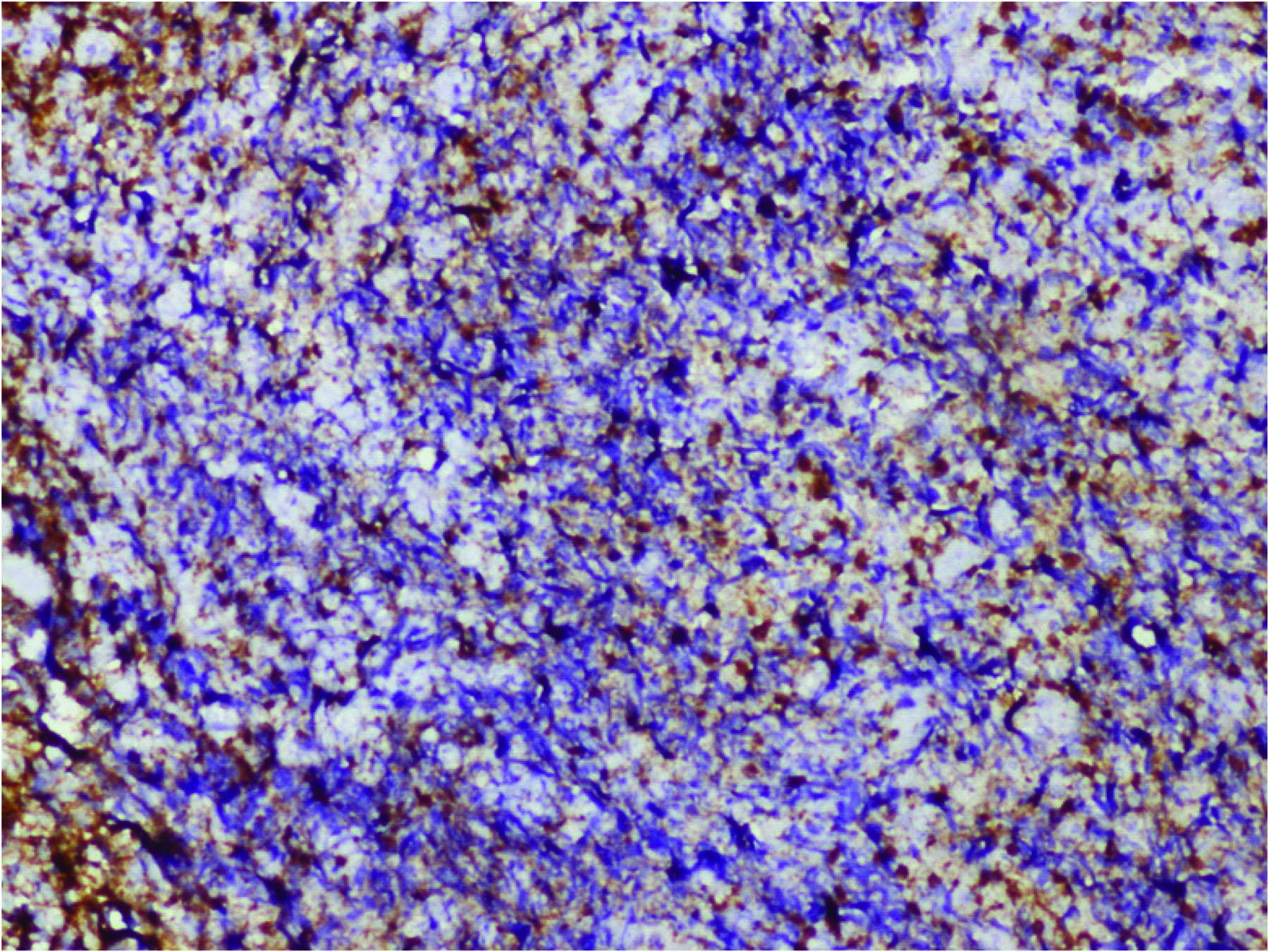
Routine investigations including complete haemogram and blood sugar levels were normal. Serology for human immunodeficiency virus (HIV) was negative. FNAC was done and there was no fluid on aspiration. Incisional biopsy was performed in the left upper buccal vestibular region. Histopathological examination of the biopsy specimen revealed sheets of large diffuse lymphoblastic cells [Table/Fig-2] with ovoid vesicular nuclei and prominent nucleoli with indistinct cell borders [Table/Fig-3]. Tissue was sent for Immunohistochemistry (IHC) and panels of antibodies were performed. IHC revealed large neoplastic cells which were positive for CD20 [Table/Fig-4] PAX5 [Table/Fig-5] and bcl2, demonstrating light chain restriction ( kappa positive, lambda negative [Table/Fig-6]. The Ki-67 index is >80% [Table/Fig-7]. The cells are cyclin D1, CD23, CD5, Tdt and CD138 negative. Background CD3 positive T cells were noted [Table/Fig-8].
H & E (4x) – Revealed sheets of large diffuse lymphoblastic cells
Hx&E (40 x) - Large diffuse lymphoblastic cells with ovoid vesicular nuclei and prominent nucleoli with indistinct cell borders
According to these findings the final diagnosis of Primary high grade non-Hodgkin’s lymphoma of Diffuse Large B cell type was established.
Disscussion
Non-Hodgkin’s Lymphoma occurs within the lymphatic system and can also arise extranodally. When NHL appears extranodally in the oral cavity, it is usually indicative of widely disseminated disease [1]. Among various head and neck sites, Waldeyer’s ring, which is an area encompassed by the nasopharynx, the tonsil and the base of the tongue is most often involved by malignant lymphoma . Involvement of buccal mucosa, tongue, floor of the mouth and lips has been reported quite infrequently with approximately 2% of all extranodal lymphomas [2].
Diffuse Large B cell Lymphoma (DLBCL) variant of Non-Hodgkin’s lymphoma is an aggressive malignancy of mature B lymphocytes and was rare in oral cavity. An increasing number of AIDS related malignant lymphoma of the oral cavity of both B and T cell types have been reported, the former predominant [3]. In the group of HIV-infected individuals, patients with lymphoma are almost all men, who are overall younger individuals. DLBCL was having large diagnostic discrepancies between inter and intra-observer based on morphological features alone [4].
In general it affects the elderly patients of any age, especially over the 6th decade of life with male preponderance [5]. The most common presenting symptoms are local swelling, pain or discomfort [2]. In our case, the male patient aged 50yrs presented with a symptomatic swelling in the left infraorbital region.
The cause of NHL is still unclear. Viruses have been suggested as a potential cause of the disease. An increased rate of lymphoma in patients who are congenitally immunosuppressed and in patients who receive immunosuppressive therapy has been reported [5].
DLBCL is composed of large malignant transformed B cells with immunoblastic features, which may develop in both children and adults. The majority of reported cases have B cell phenotype. T cell phenotype is much more likely to occur in sinonasal than oropharyngeal lymphomas [3].
For high grade lymphomas, the treatment for localized lesion consists of radiation and chemotherapy, while with more advanced and disseminated conditions chemotherapy alone is usually implemented [2]. Our patient was treated with chemotherapy and radiotherapy following excision of the lesion as histopathologically it was diagnosed to be a high grade lymphoma.
Diagnosis of an NHL in the oral cavity is often difficult because it may resemble other conditions such as dental abscesses [6]. A proper clinical, histopathological as well as immunohistochemical evaluation of biopsy specimen may aid in the diagnosis and thus, help in proper management [3]. The survival time is greatly dependent on the extent of disease dissemination and it’s aggressiveness. The literature states that the five year survival rate of head and neck NHL is 65% to 73% [1]. An early biopsy will provide an appropriate diagnosis and avoid disease progression, thus improving the prognosis.
Conclusion
A proper clinical evaluation, in addition to a histopathological as well as immunohistochemical evaluation of the biopsy specimen is necessary for the correct diagnosis and management. Being concluded that NHL involving the oral cavity is uncommon, it should be emphasized and considered as a differential diagnosis of other malignant lesions, because treatment and prognosis may vary for individual lesions.
[1]. Kell Tina, DDS, BSc, Glassman Gary, Primary Non-Hodgkin’s Lymphoma Presentation on the Gingival Mucosa: A Case ReportDDS, FRCD(C) 2008 8:51-54. [Google Scholar]
[2]. Maheshwari Gopal Krishna, Baboo Harshad Acharatlal, Shah Nilesh Manubhai, Primary non-Hodgkin’s lymphoma of the oral tongueTurkish Journal of Cancer 2001 31(3):121-124. [Google Scholar]
[3]. Non-Hodgkin’s Lymphoma of the Tongue Presenting as an Ulcerative Lesion. Negar Azarpira, Mohammad Javad Ashraf, Bijan KhademiMiddle East Journal of Cancer 2011 2(3 & 4):125-28. [Google Scholar]
[4]. Ash A, Alizadeh, Michael B. Eisen, R. Eric Davis, Chi Ma. Distinct types of diffuse large B-cell lymphoma identified by gene expression profilingNature 2000 403:503-11. [Google Scholar]
[5]. Kobler P, Borcic J, Zore I. Filipovic, Nola M, Sertic D, Primary non-Hodgkin’s lymphoma of the oral cavityOral Oncology EXTRA 2005 41:12-14. [Google Scholar]
[6]. Patricia Carla, Ricardo Celso, Benedito Jose, Lombardi Tommaso, Primary extranodal non-Hodgkin lymphoma of the gingival initially misdiagnosed as dental abcessQuintessence International 2009 40(10):805-08. [Google Scholar]