Introduction: The present study aims to assess different morphometric parameters of condylar and intercondylar surface of tibia and to compile the results, analyze and formulate a baseline data for future studies with relevance to Indian population and also to compare the current data with accessible literature for pertinent surgical utilities. Morphometric parameters of upper end of tibia can be used to guide treatment and monitor outcome of total knee replacement surgeries. Information regarding morphometry of upper end of the tibia is vital as it provides reliable method of assessing knee deformity.
Materials and Methods: The study group comprised of 50 male and 50 female adult human tibiae. Morphometric measurements of medial condyle, lateral condyle and intercondylar area of tibiae were meticulously recorded with digital Vernier calipers with a least count of 0.01 mm. Student’s t-test was used with significant level of p-value < 0.05 and 95% confidence interval.
Results: All measurements were found to be statistically significant when compared between the two sexes on both sides (p-value<0.05). Anteroposterior measurements were found to be greater than transverse measurements for both medial and lateral condyles. Furthermore, both anteroposterior and transverse measurements were greater in medial condyle than in lateral condyle on both sides and sexes.
Conclusion: The present study is an endeavor to provide a base line data pertaining to morphometric details of upper end of tibia with reference to unicompartmental and total knee arthroplasty in Indian population. The results of the study assume special importance in view of the technical advancements in reconstructive surgical procedures in orthopedic practice.
Introduction
The lower limb is primarily adapted for weight bearing and locomotion. This functional need alongwith together with the attainment of a habitual erect bipedal posture has resulted in a change in both the functional and mechanical requirements of all skeletal structures. Therefore greater strength and stability is required for the lower limb as compared with the upper limb [1].
In man weight bearing is related mainly to extended knee positions. The relationship between the different weight bearing situations and the anteroposterior and medio-lateral dimensions of diaphysis and epiphysis of the tibia is well established [2]. Information regarding morphometry of upper end of the tibia is vital as it provides reliable method of assessing knee deformity. Morphometric parameters of upper end of tibia can be used to guide treatment and monitor outcome of total knee replacement surgeries. An accurate and repeatable tibial measurement system aids in definition of tibial deformity and improvement of tibial prosthesis design [3]. Knee joint surgeries are technically demanding and rapidly evolving procedures; hence an elaborate anatomical study of this relevant surgical field would serve in planning required interventions in numerous pathological and degenerative conditions of the knee joint.
Materials and Methods
The material for the present study comprised of one hundred adult human tibia bones of known sex and side. The study group comprised of 50 male and 50 female bones with equal number of right and left sided bones [Table/Fig-1]. All measurements were recorded with the help of Vernier calipers with a least count of 0.01 mm.
Following metric parameters were noted:
1. Anteroposterior measurements of superior articular surface of medial condyle: The maximum distance between anterior and posterior borders of superior articular surface of medial condyle [AB in Table/Fig-2].
2. Transverse measurements of superior articular surface of medial condyle: The maximum transverse diameter of superior articular surface of medial condyle [CD in Table/Fig-2].
3. Anteroposterior measurements of superior articular surface of lateral condyle: The maximum distance between anterior and posterior borders of superior articular surface of lateral condyle [EF in Table/Fig-2].
4. Transverse measurements of superior articular surface of lateral condyle: The maximum transverse diameter of superior articular surface of lateral condyle [GH in Table/Fig-2].
5. Anteroposterior measurements of intercondylar area: The maximum distance between anterior and posterior borders [IJ in Table/Fig-2].
6. Transverse measurements of intercondylar area: The maximum transverse diameter at following three levels:
a) anterior end [KL in Table/Fig-2] .
b) middle narrow part – (at the level of intercondylar eminence) [DG in Table/Fig-2].
c) posterior end [MN in Table/Fig-2].
7. Anteroposterior measurements of anterior intercondylar area: The maximum distance between anterior border of intercondylar area to a line joining intercondylar eminence [OP in Table/Fig-2].
8. Anteroposterior measurements of posterior interco- ndylar area: The maximum distance between a line joining intercondylar eminence and posterior border [QR in Table/Fig-2].
The data thus obtained was expressed as means + standard deviation (SD) followed by application of student’s t-test on both right and left sided bones of two sexes and p-value < 0.05 was considered significant for analysis. All the statistical tests were performed by using SPSS software (version 12.0).The results were scrutinized and were discussed in the light of available literature.
Table depicting the description of the study group (n=100)
| Sex/Side | Right Tibiae | Left Tibiae | Total |
| Males | 25 | 25 | 50 |
| Females | 25 | 25 | 50 |
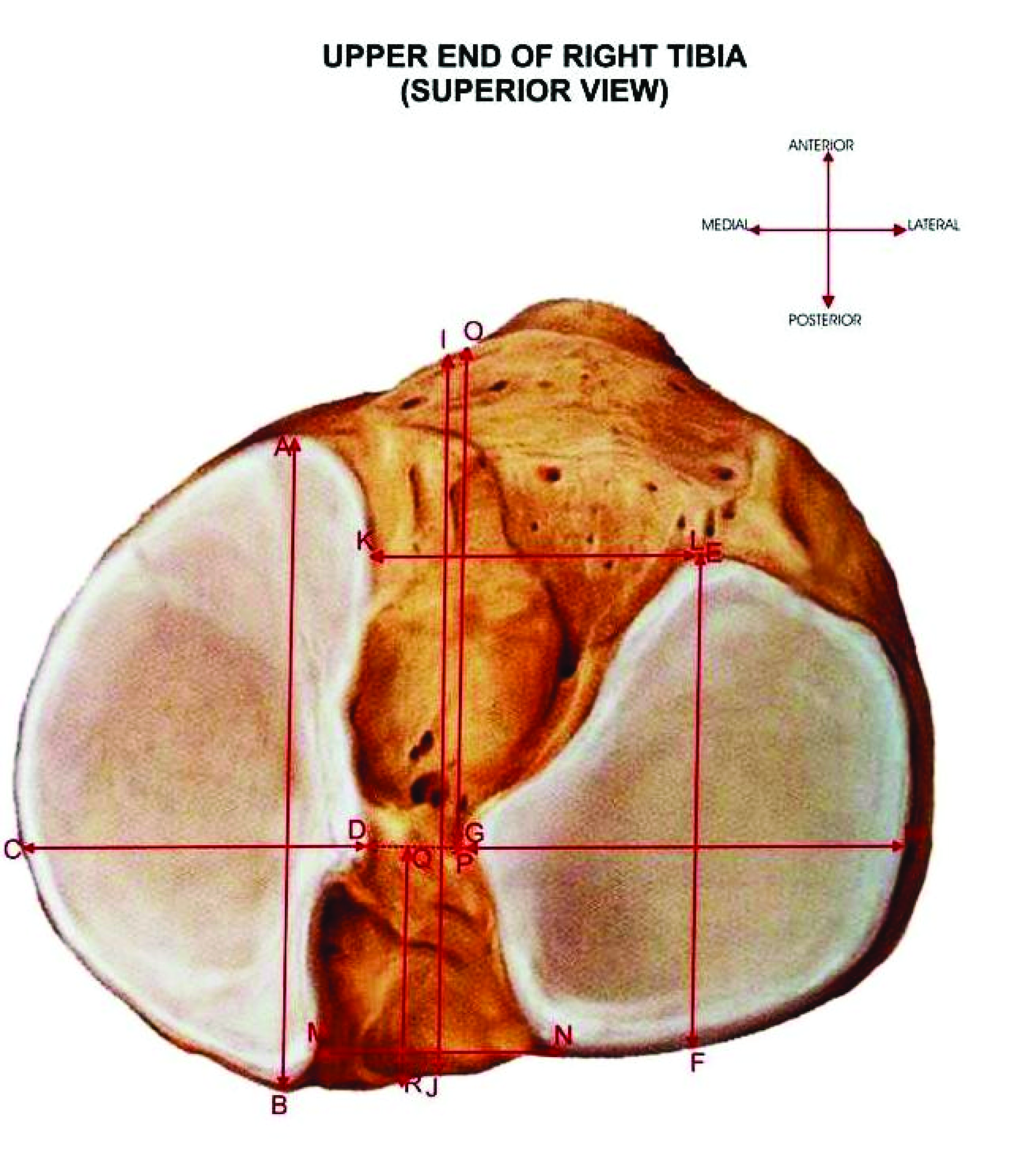
Showing measurements of different parameters of upper end of right tibia
AB and CD- Anteroposterior and Transverse measurements of superior articular surface of medial condyle
EF and GH- Anteroposterior and Transverse measurements of superior articular surface of lateral condyle
IJ – Anteroposterior measurement of intercondylar area
KL- Transverse measurement of intercondylar area at anterior end
DG- Transverse measurement of intercondylar area at middle narrow part
MN- Transverse measurement of intercondylar area at posterior end
OP and QR- Anteroposterior measurements of anterior and posterior intercondylar area
Comparison of anteroposterior and transverse measurements of medial condyle *Significant
| Authors | Race | Diameters(mm) | Side | Sex | Mean+S.D (n) | p-value |
| Servien et al., [4] | French | Anteroposterior | - | - | 50.8+3.3(37) | - |
| Present Study | North Indians | Anterop-osterior | Right | Male | 48.45+4.14(25) | <0.001* |
| Female | 42.39+4.19(25) |
| Left | Male | 47.73+4.37(25) | <0.001* |
| Female | 42.36+4.65(25) |
| Transverse | Right | Male | 30.18+2.83(25) | <0.001* |
| Female | 27.25+3.05(25) |
| Left | Male | 29.38+3.14(25) | 0.003 |
| Female | 26.96+2.18(25) |
Comparison of anteroposterior and transverse measurements of lateral condyle *Significant
| Diameters(mm) | Side | Sex | Mean+S.D (n) | p-value |
| Anteroposterior | Right | Male | 40.86+3.79(25) | <0.001* |
| Female | 36.78+3.03(25) |
| Left | Male | 40.69+4.13(25) | 0.004 |
| Female | 37.30+3.81(25) |
| Transverse | Right | Male | 28.62+3.10(25) | 0.003 |
| Female | 26.14+2.51(25) |
| Left | Male | 28.82+3.12(25) | 0.002 |
| Female | 26.00+3.06(25) |
Comparison of measurements of intercondylar area
| Diameters (mm) | Authors (year) | Race | Mean + S.D (mm) (n) |
| | | | Right (n) | Left (n) |
| | | Male | Female | Male | Female |
| Antero Posterior | Kwak et al.,[5] | Korean | 47.3+3.8(200) |
| Present Study | North Indians | 47.19+ 2.93(25) | 43.09+ 3.62(25) | 49.11+ 3.97(25) | 44.64+ 3.94(25) |
| Transverse (anterior end) | Jacobsen [6] | Danish | 35(13) Range=26-43 |
| Present Study | North Indians | 24.82+ 3.22(25) | 22.33+ 3.48(25) | 25.40+ 4.20(25) | 22.61+ 2.41(25) |
| Transverse (middle narrow part) | Jacobsen [6] | Danish | 11(13) Range=7-14 |
| Present Study | North Indians | 7.18+ 1.14(25) | 6.72+ 1.06(25) | 7.41+ 0.95(25) | 6.38+ 0.79(25) |
| Transverse (posterior end) | Jacobsen [6] | Danish | 16(13) Range=12-22 |
| Present Study | North Indians | 7.18+ 1.14(25) | 6.72+ 1.06(25) | 7.41+ 0.95(25) | 6.38+ 0.79(25) |
Showing anteroposterior measurements of anterior/posterior intercondylar area
| Diameters(mm) | Side | Sex | Mean+S.D (n) | Range | p-value |
| Anteroposterior (anterior I/C area) | Right | Male | 23.84+2.90(25) | 18.69-31.22 | 0.034 |
| Female | 25.48+2.38(25) | 20.08-31.21 |
| Left | Male | 21.96+6.76(25) | 12.26-33.16 | 0.049 |
| Female | 25.04+3.48(25) | 18.18-31.24 |
| Anteroposterior (posterior I/C area) | Right | Male | 17.86+2.98(25) | 12.97-27.09 | <0.001 |
| Female | 21.84+2.64(25) | 14.71-26.42 |
| Left | Male | 23.22+2.55(25) | 16.19-27.21 | 0.272 |
| Female | 22.38+2.84(25) | 16.07-26.92 |
Results
This morphometric study conducted on adult human tibiae of Indian population revealed the under-mentioned important observations.
The mean values of anteroposterior measurement of medial condyle as observed on the two sides in both male and female bones of the present study are depicted in [Table/Fig-3]. The difference between the two sexes on both the sides was highly significant statistically (p-value <0.001 on both right and left sides). However, when compared between the two sides though the measurement was greater on right side in both the sexes, the difference was statistically insignificant (p-value 0.551 in males & 0.980 in females). The transverse measurement of the medial condyle of two sides in both the sexes is also stated in [Table/Fig-3]. When compared between the two sexes, the difference was statistically significant on both the sides (p-value on right side <0.001 & on left side 0.003). However, when compared between the two sides, the difference was statistically insignificant though the measurement was more on right side in both the sexes (p-value 0.351 in males and 0.695 in females). On the other hand when anteroposterior and transverse measurements of medial condyle were compared, the anteroposterior measurement was greater than transverse measurement in both the sexes and on both the sides.
On comparing the two condyles [Table/Fig-3,Table/Fig-4] it was seen that both anteroposterior and transverse measurement were greater in medial condyle on both sides and sexes.
The anteroposterior measurement of intercondylar area as seen in the present study are highlighted in [Table/Fig-5] . When compared between the two sexes it was more in males, the difference being statistically significant on both sides (p-value <0.001 on both the sides). However when compared between the two sides, the measurement was more on left side in both the sexes but the difference was statistically insignificant (p-value 0.058 in males and 0.152 in females).
Transverse measurement of intercondylar area was measured at the levels of anterior end, middle narrow part and at posterior end of intercondylar area. The observations for the same on two sides of males and females are given in the [Table/Fig-5]. When the measurements at anterior end were compared between the two sexes on both the sides, it was more in males and the difference was statistically significant on both the sides (p-value on right side 0.011 & on left side 0.006). However, when compared between the two sides, the values were slightly more towards left side in both the sexes, though the difference was statistically insignificant (p-value 0.586 & 0.745 in males and females respectively). Transverse measurement at middle narrow part of intercondylar area was more in males as compared to females on both the sides, the difference being statistically significant on left side but insignificant on right side (p-value <0.001 on left side and 0.145 on right side). On the other hand, when compared between two sides in both sexes, the difference was statistically insignificant (p-value 0.444 < 0.206 in males and females respectively).Transverse measurement at posterior end of intercondylar area was more in males on both the sides but the difference was statistically insignificant (p-value 0.314 on right side and 0.406 on left side). Similarly when compared between two sides, the measurement was more on right side in both the sexes, but the difference was statistically insignificant (p-value 0.611 in males and 0.824 in females).
The mean values and range for the anteroposterior measurement of anterior intercondylar area on both sides in males and females are depicted in [Table/Fig-6]. When compared between two sexes on both sides, the measurement was more in females, the difference being statistically significant (p-value=0.034 on right side and 0.049 on left side). On comparison between the two sides, though it was more on right side both in males and females, the difference was statistically insignificant (p-value=0.208 in males & 0.605 in females).
As it is evident from [Table/Fig-6] the anteroposterior measurement of posterior intercondylar area was more in females on right side but on left side, it was more in males. On statistical evaluation, the difference was statistically highly significant on right side but insignificant on left side (p-value <0.001 on right side and 0.272 on left side). As far as the sides were concerned, though it was more towards the left side in both the sexes, the differences were statistically significant only in males but insignificant in females (p-value <0.001 in males & 0.493 in females).
Discussion
The current study establishes the morphometric attributes of upper end of tibia in Indian population. It is lamentable that literature in clinical sciences contains relatively little information regarding morphometry of upper end of tibia. Data obtained in the present study would presumably provide a basis for designing the optimal tibial component for unilateral and total knee arthroplasty for Indian population. Earlier only Servien et al., [4] had measured anteroposterior measurements of medial and lateral condyle in French population and found it to be 50.8+3.3mm and 47.2+3.3mm respectively; the study however was independent of sex and side [Table/Fig-2]. Furthermore, Kwak et al., [5] had measured anteroposterior measurement of intercondylar area in Korean population but irrespective of side and sex. Their values were found to be 47.3+3.8mm which are quite close to our oobservations in males [Table/Fig-4] . Jacobsen [6] had measured transverse measurements of intercondylar area at different levels in Danish population [Table/Fig-4]irrespective of sex and side. A statistical comparison of measurements between Danish and present study in the Indian population showed that the transverse measurements of intercondylar area at anterior and middle parts were more in Danish population (35mm and 11mm respectively) but that at posterior end the values were almost the same (16mm). Recognising the importance of anatomical description of the intercondylar area for the accurate identification of skeletal structures and soft tissue insertions in radiographs, Jacobsen [6] emphasized that the shape of posterior contours of the tuberculum mediale and laterale can be used for the identification of the posterior contours of the two tibial condyles and the posterior contour of the condylus lateralis tibiae may be identified by tracing the posterior curved part of the tuberculum laterale. According to him, the latter contour was most useful as a landmark in measuring the “drawer sign” in the knee joint by the radiological method of Kennedy and Fowler [7]. Designing of prosthesis, considering the gender difference have been advocated in Chinese population by cheng et al., [8] . Geoffrey [9] suggested that asymmetrical smaller lateral condylar surface produces better outcome compared to the symmetrically constructed prosthesis. As the metric parameters of medial and lateral plateau symmetrically differs with reference to each other, it may complicate the medial unicompartmental knee arthroplasty owing to unrequired mediolateral overhanging while attempting optimal anteroposterior coverage of articular surface[4]. Hopefully, the morphometric analysis of the proximal articular surface of tibia performed in the current investigation should prove to be beneficial in designing appropriate knee prosthesis for unicompartmental and total knee arthroplasty in Indian population.
Knee osteoarthritis is one of the most common causes of disability in adults. The damage results from a complex interplay of joint integrity, biochemical processes, genetics and mechanical forces. Osteoarthritis is the most common indication for total knee arthroplasty. Total and unicompartmental joint replacements have become the gold standard for treatment of osteoarthritis and other degenerative disorders of knee [10]. Total knee replacement is a resurfacing and realignment procedure which produces a pain free stable knee that ensures better motion and performance. In total knee arthroplasty, less than half an inch (9mm) of the tibial and femoral articular surfaces are removed from the ends of the bones and replaced with metal and plastic caps[11]. The current challenges in knee prosthetic design are centered on attempting to produce normal kinematics, reducing wear and tear and hence achieving greater longeivity. In lieu of meager information on the anthropometry of the proximal articular surface of the tibia, our study will provide key information in designing appropriate size-matched unicompartmental and total knee prosthesis in Indian scenario. Proper designing of the prosthesis is essential for correction of varus and valgus deformities of the knee during knee arthroplasty [12].
Thus the present study could provide the basis for designing the optimal tibial prosthesis in total knee arthroplasty for Indian population taking the ‘sex factor’ into consideration as a small sized prosthesis may show mediolateral undersizing and larger sized prosthesis may show mediolateral overhang. The purpose of this study is to analyse the dimensions of each tibial plateau for planning of unicompartmental knee arthroplasty and to compare the morphometric data with other studies in different populations.
Conclusion
We as anatomists humbly submit that the results of this study will be extremely beneficial in designing appropriate size matched components of knee prosthesis for Indian population.
[1]. S Standring, H Ellis, D Johnson, JC Healy, A Williams, Gray’s Anatomy. In Pelvic Girdle and Lower Limb. Newell RLM. Edr.Teratology 2005 39th EditionEdinburg, London,Churchill Livingstone:p1399 [Google Scholar]
[2]. AE Ljunggren, The Tuberositas Tibiae and Extension in the knee joint.Acta Morphol Neerl Scand. 1976 14:215-39. [Google Scholar]
[3]. DG Mark, Consistency and accuracy of measurement of lower limb amputee anthropometrics.JRRD 2005 42:131-40. [Google Scholar]
[4]. E Servien, M Saffarini, S Lustig, S Chomel, P Nevret, Lateral versus medial tibial plateau: morphometric analysis and adaptability with current tibial component design.J Knee Surg. 2008 16:1141-45. [Google Scholar]
[5]. DS Kwak, S Surendran, YH Pengatteeri, SE Park, KN Choi, P Gopinathan, Morphometry of the proximal tibia to design the tibial component of total knee arthroplasty for the Korean population.Knee. 2007 14:295-300. [Google Scholar]
[6]. K Jacobsen, S Mehta, R Kalra, Area intercondylaris tibiae: osseous surface structure and its relation to soft tissue structures and applications to radiography.J Anat. 1974 117:605-18. [Google Scholar]
[7]. JC Kennedy, PJ Fowler, Medial and anterior instability of the knee. An anatomical and clinical study using stress machines.J Bone Joint Surg. 1971 53A:1257-70. [Google Scholar]
[8]. FB Cheng, XF Ji, Y Lai, JC Feng, WX Zheng, YF Sun, Three dimensional morphometry of the knee to design the total knee arthroplasty for Chinese population.Knee. 2009 16:341-47. [Google Scholar]
[9]. GH Westrich, SB Haas, JN Insall, A Frachie, Resection specimen analysis of proximal tibial anatomy based on 100 total knee arthroplasty specimens.J Arthroplasty. 1995 10:47-51. [Google Scholar]
[10]. S Zanasi, Innovations in total knee replacement: new trends in operative treatment and changes in peri-operative management.Eur Orthop Traumatol. 2011 2:21-31. [Google Scholar]
[11]. http://www.tour2india4health.com/total-knee-replacement-india-low-costbenefits.html [Google Scholar]
[12]. JM Cuckler, Correcting extra-articular deformity of the knee: Acting in tandem.Orthopedics. 2007 30:774-76. [Google Scholar]