The Sciatic Nerve (SN) is formed in the pelvis by joining of the ventral rami of L4-S3 SN roots. It is 2 cm wide, leaves the pelvis through the greater sciatic foramen below the piriformis and descends between the greater trochanter and Ischial tuberosity in the gluteal region. The nerve divides subsequently into two terminal branches Common Peroneal Nerve (CPN) and Tibial Nerve (TN) usually at the superior angle of popliteal fossa. It is a mixed nerve contains both motor and sensory fibers. The motor branches supply the posterior compartment of thigh muscles as well as hip and knee joint, however sensory branches supply the whole tibial and foot areas with the exception of the anteromedial tibial region and medial margin of the foot.
SN presents significant variations concerning its topography and division. Higher level of division of SN is a relatively frequent phenomenon, where it may divide into its terminal branches, anywhere in the thigh or in the pelvis. In the latter case, its branches or even the whole nerve may emerge either below, above or through the piriformis. High division of SN may be unilateral or bilateral mostly leading to compression of nerve resulting in piriformis syndrome.
Variant course of SN may lead to inadvertent injury during operative procedures in the gluteal region, coccygodynia etc. Inadvertent injury or compression of SN causes paralysis or paresis of the thigh muscles and adequate sensory disturbances. Each anatomical variation reflects a different and case specific presentation which requires a detailed description of various forms of anatomical variations. Hence, present study is undertaken to know the level of division, exit, course, relationship to piriformis and variations in the branching pattern of sciatic nerve.
Materials and Methods
During routine dissection for 1st year MBBS students in the Department of Anatomy, JJM Medical College, Davangere, Karnataka, India in about 25 cadavers (50 lower limbs) the course and division of the SN were evaluated for any possible variations. The study was conducted at JJM Medical College, Davangere over a period of four years from 2009-2013. The gluteal region, back of the thigh and popliteal fossa were exposed by dissection. The gluteus maximus muscle was cut from it insertion and reflected towards its origin. The biceps femoris muscle was retracted and the nerve was then exposed in popliteal fossa. The exit of the nerve from pelvis, its relation to piriformis and level of division of the nerve were recorded. The level of SN division was described topographically with respect to the region where the division took place. The entire course of the nerve was delineated and looked for any possible variations.
Observation and Results
In the present study of 25 cadavers, total of 50 gluteal regions were examined for the variation in the course and division of the SN. Among them 46 specimens (92%) the SN had a normal course after its exit below the piriformis and divided into TN and CPN at the superior angle of popliteal fossa, while in 4 specimens (8%) there was high division of SN within the pelvis. While in two limbs trifurcation of SN was observed with an additional muscular branch to soleus. In one limb the SN divided above the piriformis into TN & CPN later reunited at the back of thigh and re-split normally at the superior angle of the popliteal fossa thus having a varied course.
In a male cadaver, aged around 60 years on right side there was high division of SN in the pelvis. TN passed below the piriformis and CPN passed above the piriformis to enter into the gluteal region. Both the nerve had independent course in the upper one third of the thigh. Later both the components fused in the middle one third of the back of thigh and subsequently re-split normally at the superior angle of the popliteal fossa into TN and CPN respectively. On the left side in the same cadaver, SN emerged as a single trunk, passed beneath piriformis and had a normal course in the back of thigh but it trifurcated distally into TN, CPN, and additional muscular branch to Soleus [Table/Fig-1]. While on the left side in the same cadaver SN passed normally beneath the piriformis muscle while distally it trifurcated into TN, CPN & Nerve to soleus [Table/Fig-2].
Showing higher division of SN on the right side into TN & CPN which later united in the middle third of thigh and further showing trifurcation of SN in its terminal part in to TN nerve, CPN and nerve to soleus on the right side
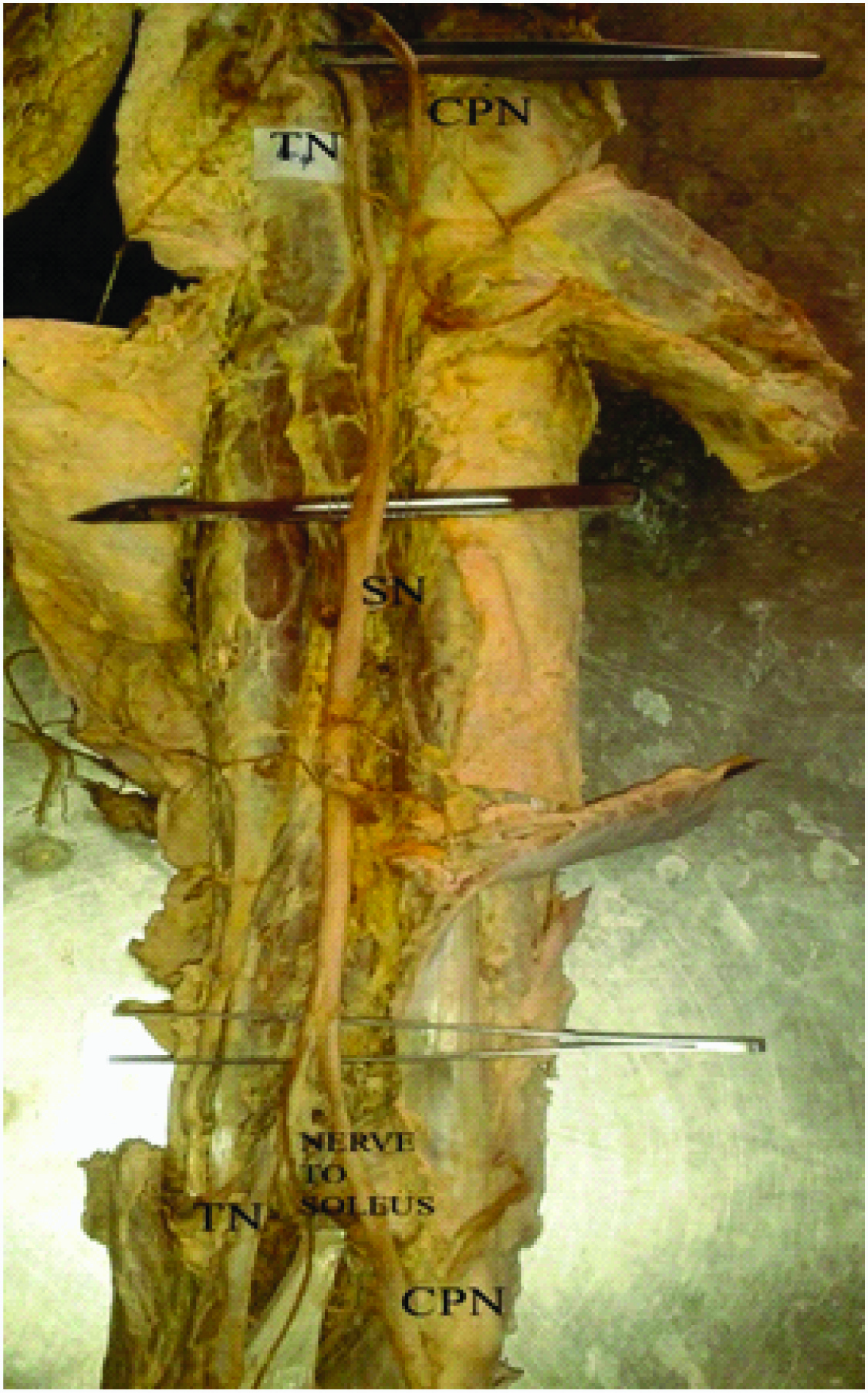
Showing trifurcation of SN into TN nerve, CPN and nerve to soleus on the left side

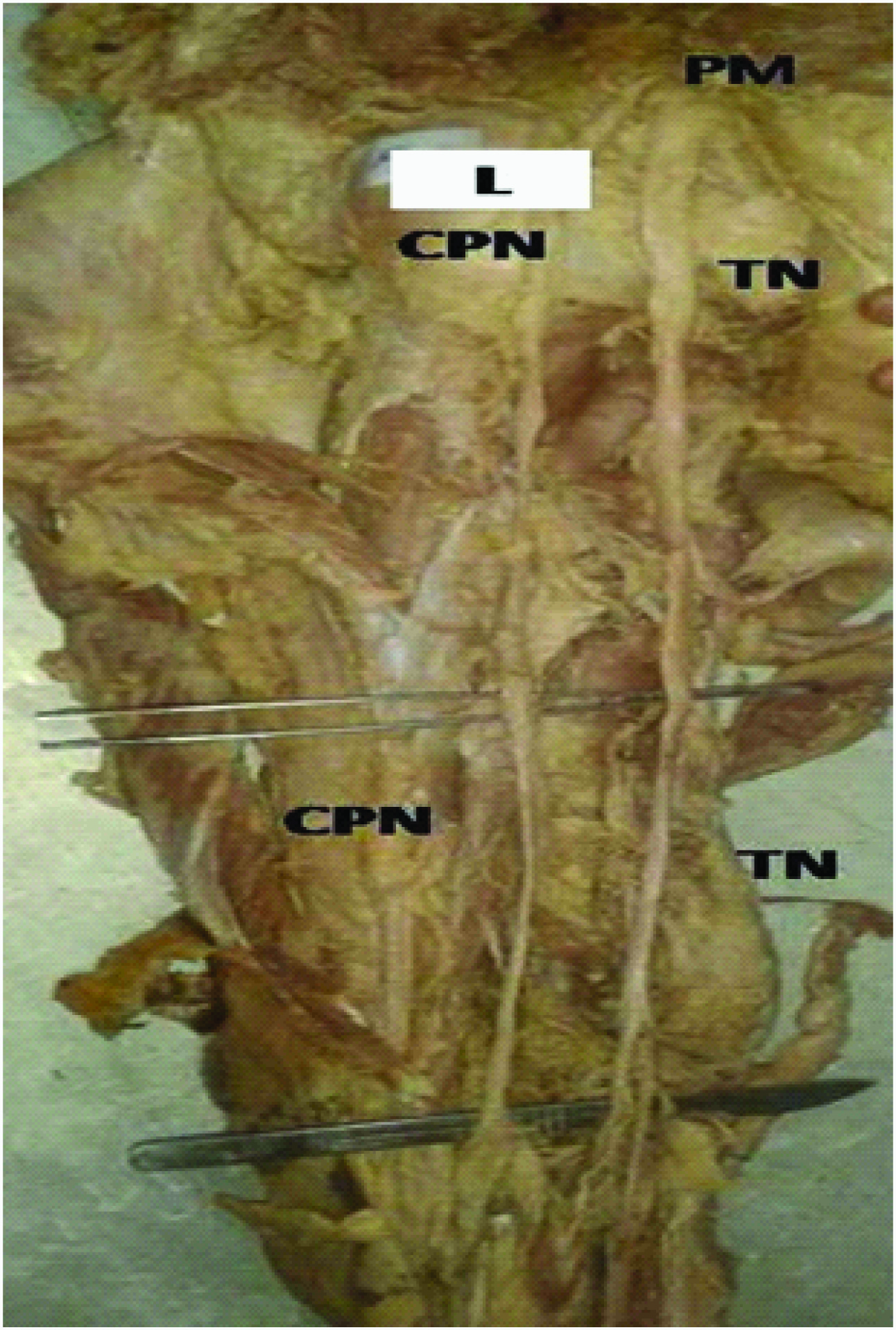
In another male cadaver aged around 50 years, the SN after emerging as a single trunk below the piriformis and later divided at the lower border of piriformis muscle into TN, and CPN. The two nerves passed along the back of thigh respectively along the medial and lateral side of thigh giving no additional branches. CPN later winded around neck of fibula in the lower part of popliteal fossa [Table/Fig-3]. While on the right side in the same cadaver, there was high division of SN in the pelvis and CPN pierced the piriformis muscle and the TN passed below the piriformis, both the nerves had independent course in back of thigh, rest of the course of the nerve was normal [Table/Fig-4].
Showing undivided left sided sciatic nerve emerging beneath lower border of piriformis muscle later dividing beneath the lower border of muscle in the back of thigh into TN nerve & CPN respectively
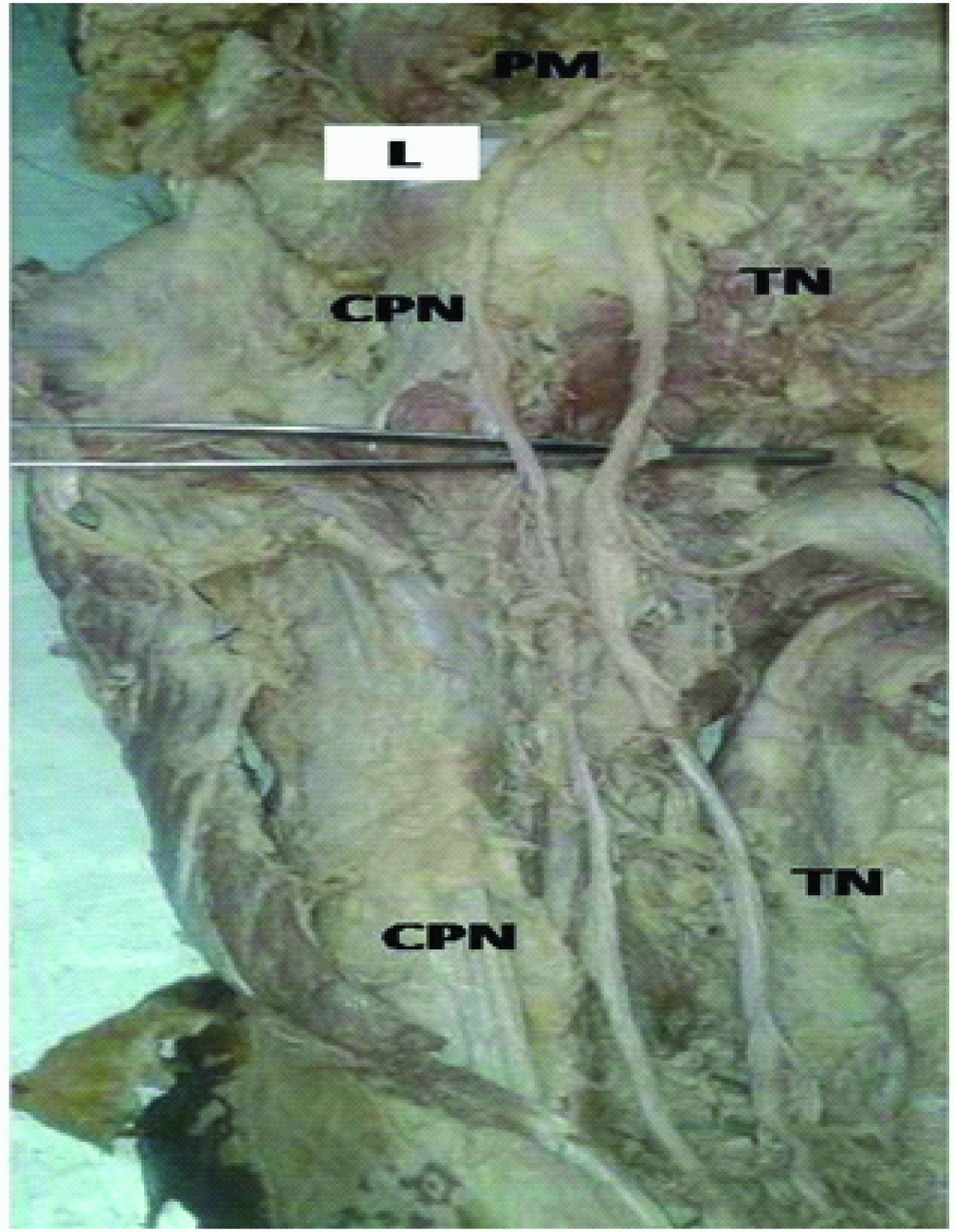
Showing higher division of SN into TN nerve which passes below while CPN nerve passes through piriformis on the right side
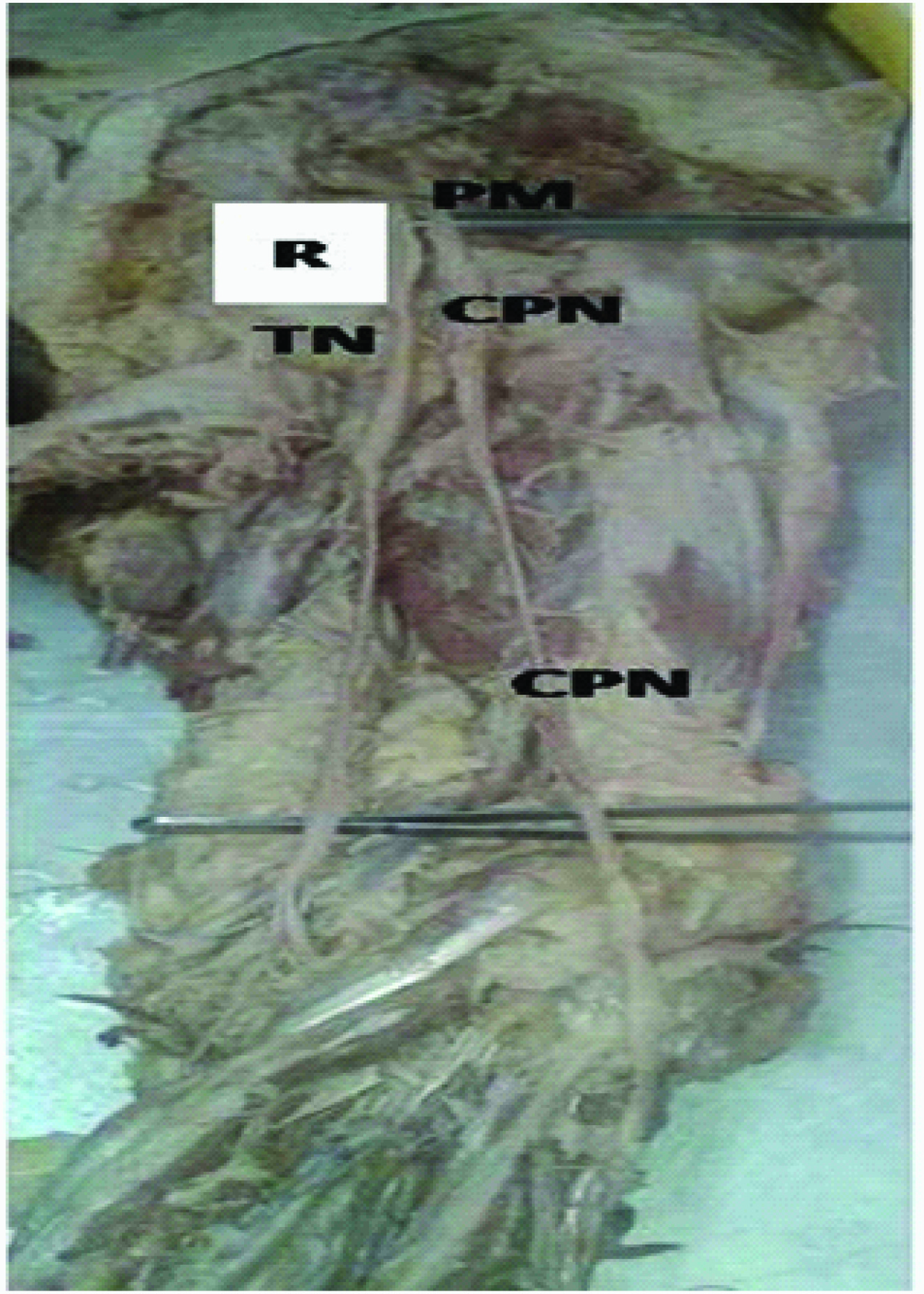
In another specimen there was high division of SN into TN & CPN on the left side however both nerves passed along the back of thigh without giving any additional branches in the region [Table/Fig-5].
Showing higher division of SN into TN nerve passing below while CPN nerve passing above piriformis on the left side
However in the remaining 45 specimens, the sciatic nerve passed normally beneath piriformis and divided into TN and CPN at the superior angle of popliteal fossa. There were no associated variations pertaining to its branches and course.
In our study on 25 cadavers (50 lower limbs) we have observed sciatic nerve emerged as a single trunk below the piriformis in 46 specimens (92%). High division of SN in the back of thigh was noted in one specimen (2%) and high division of SN in the pelvis was noted in 3 specimens (6%). In cases of pelvic division, the tibial nerve was always infrapiriformic, while the common peroneal nerve passed above piriformis in 1(2%) cases, pierced the piriformis in 1(2%).Trifurcation of the distal part sciatic nerve was also noted in two specimens where an additional muscular branch to soleus was seen arising in both specimens (4%).
Discussion
SN usually divides in the upper angle of popliteal fossa to CPN & TN [1–3]. In the current study, only 92 % of the SN confirmed to this standard textbook description. High division of SN in the back of thigh was noted in one specimen (2%) and high division of sciatic nerve in the pelvis was noted in 3 specimens (6%) which suggest that the frequency of variant anatomy of SN. Each of the anatomical variations may reflect a different and case-specific clinical presentation of sciatic neuropathy. A large number of variations in the course and distribution in the SN have been reported earlier in the literature [Table/Fig-6]. The nerve may divide into two major divisions, CPN and TN at varied levels extending from sacral plexus till the lower part of the thigh [Table/Fig-7].
Depicting the level of division of sciatic nerve in comparison with the earlier studies
| Author | No. of specimens | Level of division in % |
|---|
| Before exiting pelvis | After exiting pelvis |
|---|
| Gabrielli et al., 1997 [2] | 40 | 13.7 | 86.3 |
| Ugrenovic et al., 2005 [5] | 100 | 4.0 | 96.0 |
| Pokorny et al., 2006 [5] | 91 | 20.9 | 79.1 |
| Prakash et al., 2010 [4] | 43 | 16.3 | 83.7 |
| Guvencer et al., 2010 [6] | 25 | 48 | 52 |
| J.A. Ogeng’o., 2011 [5] | 164 | 20.1 | 79.9 |
| Present study | 50 | 8.0 | 92.0 |
Depicting the level of division of sciatic nerve in the present study
| Level of division | Normally at sup. Angle of popliteal fossa | % | High division within pelvis | % | High division in the back of thigh | % | Total no of specimen/limbs | % |
|---|
| No of specimen/limbs | 46 | 92 | 3 | 6 | 1 | 2 | 50 | 100 |
Many authors have given classification for high division. But according to Beatons and Ansons classification, the classification of SN division is as follows:
Type 1: Undivided nerve below undivided muscle.
Type 2: Division of nerve between and below undivided muscle.
Type 3: Division above and below undivided muscle.
Type 4: Undivided nerve between heads.
Type 5: Division between and above heads.
Type 6: Undivided nerve above undivided muscle [3].
In the present study we have encountered Type 1, Type 3, and in one case CPN passed through the piriformis while TN passed beneath the muscle. In one case, after emerging normally beneath undivided muscle, the nerve split into CPN and TN which had usual course later in the back of thigh and in two cases there was trifurcation of the nerve at the superior angle of popliteal fossa giving additional muscular branch to soleus.
In one specimen there was high division of SN later the CPN and TN reunited and then again split at superior angle of popliteal fossa into CPN and TN. Such incidences have been reported in 4.9% in Kenyan population [5].
High division of SN has been reported earlier with an incidence of 48% [6]. The probable basis for this pelvic division is the separate existence of the nerves during embryonic development. The level of division of the SN influences the extent of neurological deficit in sciatic neuropathy. For instance, division in the gluteal region or proximal to the popliteal fossa may result in involvement of only one of the two divisions during popliteal fossa injuries. It may account for failure of SN block when performing popliteal block anesthesia.
In the present study we also observed specimens with trifurcation of SN into CPN, TN and muscular branch to Soleus. Such cases of trifurcation have been earlier reported with different branches by S P Sawant [7], Satheesh Nayak [8].
Piriformis syndrome is caused by an entrapment of SN as it exits the greater sciatic notch. There are two normal variations in the exit of SN in the first case the SN passes inferior to the piriformis muscle and superior to the gemellus superior muscle or may split in to TN and CPN which have varied relations to piriformis muscle. Entrapment in this area is likely due to a myospasm or contracture of either of these muscles [9,10].
In present study one case with high division of SN in pelvis & the TN passing beneath the muscle and CPN passed through the piriformis muscle was noted (2%), such variations has been termed as Beaton and Anson type 7 [6,11]. Similar variations were earlier reported by Beaton L E et al., with an incidence of 11.7% in 2250 lower limbs , Lee et al., with an incidence 19.6% in 168 lower limbs [12]. Mustafa Guvencer [6,11] et al., in16% of cases, Prathiba K [12] et al., in 3 % and Gabrielli [2] et al., in 11.2%, Ewa Okrazeweska et al., [13] in 2% Chiba et al., [14] in 34%.
Beaton LE [15], et al., Gabrielli [2], et al., Ewa Okraszweska [13], et al., Mustafa Guvencer [6,11], et al., and Prathibha K [12] et al., reported that the CPN passed above the piriformis and the TN below the piriformis after dividing in the pelvis, in 3.3% ,2.5%, 5.5%,8%, 4% respectively. In the present study the incidence of such variation is 6%.
Reunion of CPN and TN in the back of thigh, after dividing in the pelvis as seen in the present study may cause confusion in the evaluation and interpretation of sciatic, common peroneal, tibial neuropathy and nerve block. Furthermore, it may be important in explaining the reduced severity of the presentation of the sciatic neuropathy. It may also provide the anatomical basis for spontaneous reinnervation of muscles following nerve injury [4]. Hence such type of variations must be kept in mind during various operative procedures in the gluteal region.
Conclusion
High division of SN was noted in 8% cases in the present study, of which 2% cases presented high division in the back of thigh, while 6% cases showed high division within the pelvis and Trifurcation of the SN was also noted in 4% of cases. Knowledge regarding the variation in the level of division of the SN and how it leaves the pelvis is of utmost importance in order to prevent inadvertent injury to the nerve during various surgical procedures in the gluteal region. Variations such as high division and trifurcation of nerve can lead to nerve injury during deep intramuscular injections, failure of sciatic nerve block anesthesia during various surgical procedures, piriformis syndrome or inadvertent damage to SN during varicose vein stripping. Variations in the course of SN may complicate surgery and in the interpretation of sciatic neuropathy. Hence preoperative nerve imaging and extra operative diligence are recommended during various surgical interventions of the gluteal regions.