Hirayama Disease: Imaging Profile of Three Cases Emphasizing the Role of Flexion MRI
Radha Sarawagi1, Sathya Narayanan2, Prakash Manikka Lakshmanan3, Sunitha Vellathussery Chakkalakkoombil4
1Associate Professor, Department of Radiodiagnosis, Mahatma Gandhi Medical College & Research Institute, Pillaiyarkuppam, Pondicherry, India.
2Post Graduate Trainee, Department of Radiodiagnosis, Mahatma Gandhi Medical College & Research Institute, Pillaiyarkuppam, Pondicherry, India.
3Professor & Head of Department, Department of Radiodiagnosis, Mahatma Gandhi Medical College & Research Institute, Pillaiyarkuppam, Pondicherry, India.
4Associate Professor, Department of Radiodiagnosis, Mahatma Gandhi Medical College & Research Institute, Pillaiyarkuppam, Pondicherry, India.
NAME, ADDRESS, E-MAIL ID OF THE CORRESPONDING AUTHOR: Dr. Radha Sarawagi, Department of Radiodiagnosis, Mahatma Gandhi Medical College and Research Institute, Pillaiyarkuppam, Pondicherry-607402, India. Phone : +917639656801,
E-mail: radhasanjeevgupta@gmail.com
We report three cases of Hirayama disease, cervical flexion myelopathy presenting as unilateral or bilateral asymmetric muscular atrophy of forearm and hand involving C7 - T1 myotomes in young males. MRI revealed asymmetric cord atrophy, altered signal intensity of cord, posterior dural detachment and enlarged posterior epidural space with multiple flow voids. This article emphasizes the role of Flexion MRI in diagnosing Hirayama disease.
Cord atrophy, Dural detachment, Flexion MRI, Hirayama disease
Case Report
Case 1
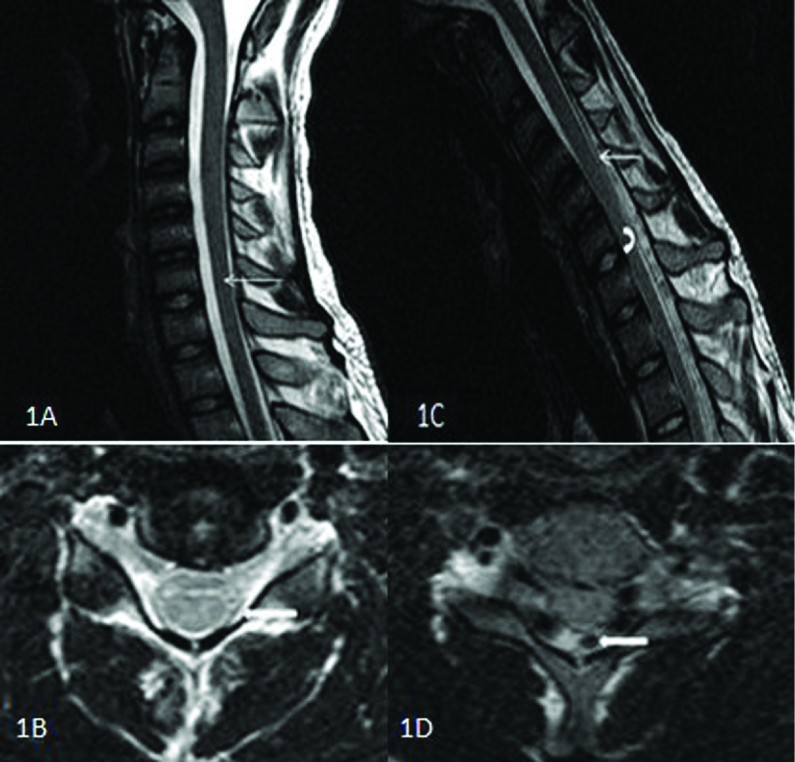
A 30-year-old male presented with weakness of both the upper limbs. On examination, there was wasting and reduced power of both forearms and small muscles of hand with more severe involvement of the left upper limb. There was no sensory system involvement. Routine MRI of the cervical spine was unremarkable except for subtle cord atrophy at C6 to C7 vertebral levels and posterior dural detachment of more than 33% from the lamina [Table/Fig-1a,b]. Considering the clinical features and imaging findings, possibility of Hirayama disease was suspected. Flexion MRI was performed which showed extensive detachment of posterior dura from lamina, its anterior displacement causing enlarged posterior epidural space and engorged epidural veins. The spinal cord was compressed against the posterior margin of vertebral body [Table/Fig-1c,d].
Case 2
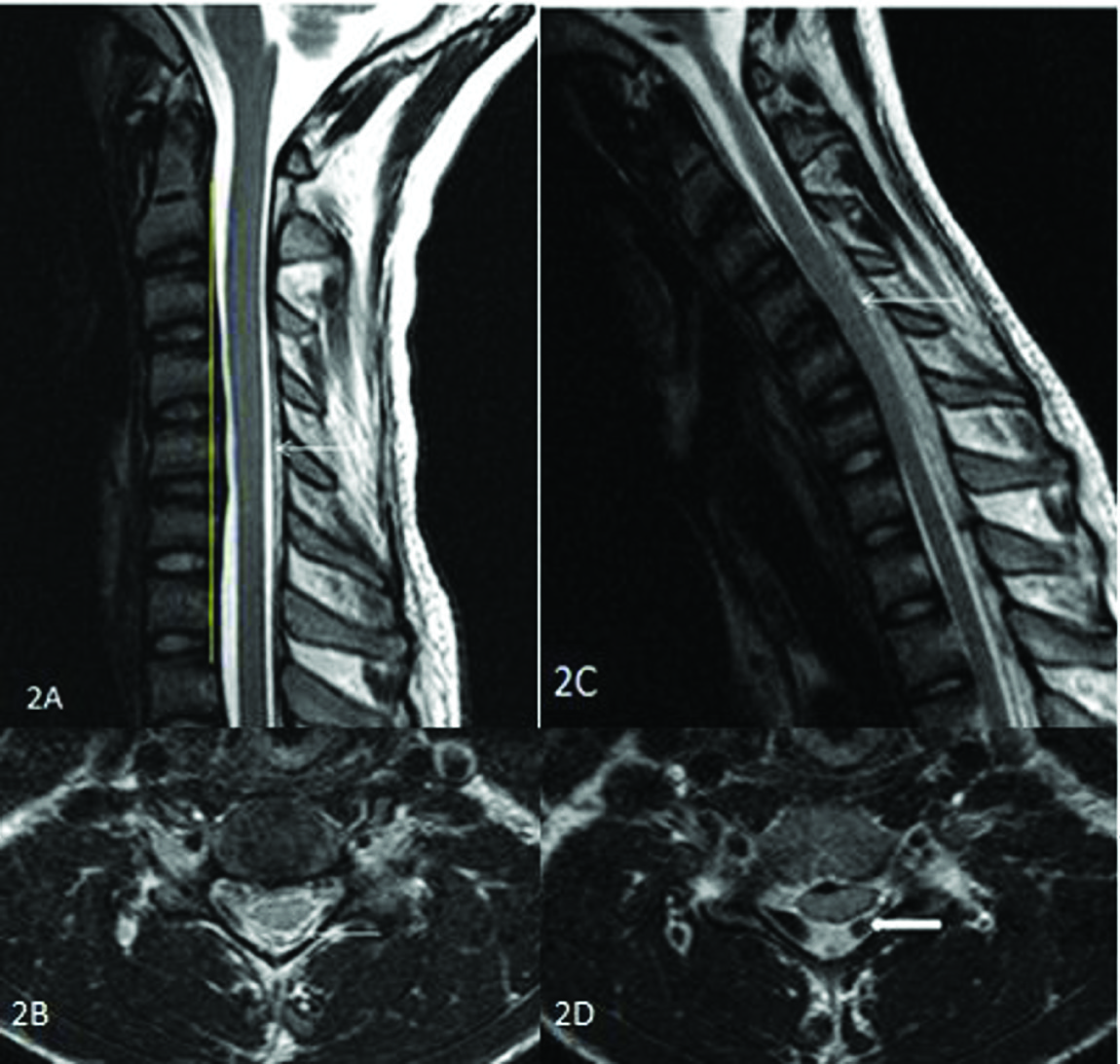
A 25-year-old male presented with reduced bulk of left hand muscles for six months associated with resting tremor and reduced grip. On examination, there was wasting and reduced power of small muscles of hand. No sensory system involvement was noted. Routine MRI of the cervical spine showed mild kyphosis of cervical spine, mild asymmetric cord flattening and atrophy. There was evidence of mild Sectionposterior dural detachment from the lamina extending from C4 to C6 vertebral levels [Table/Fig-2a,b]. Flexion MRI revealed anterior displacement of the cord with obliteration of anterior subarachnoid space, enlarged posterior epidural space with engorged epidural veins and compression of spinal cord against vertebral body [Table/Fig-2c,d].
Case
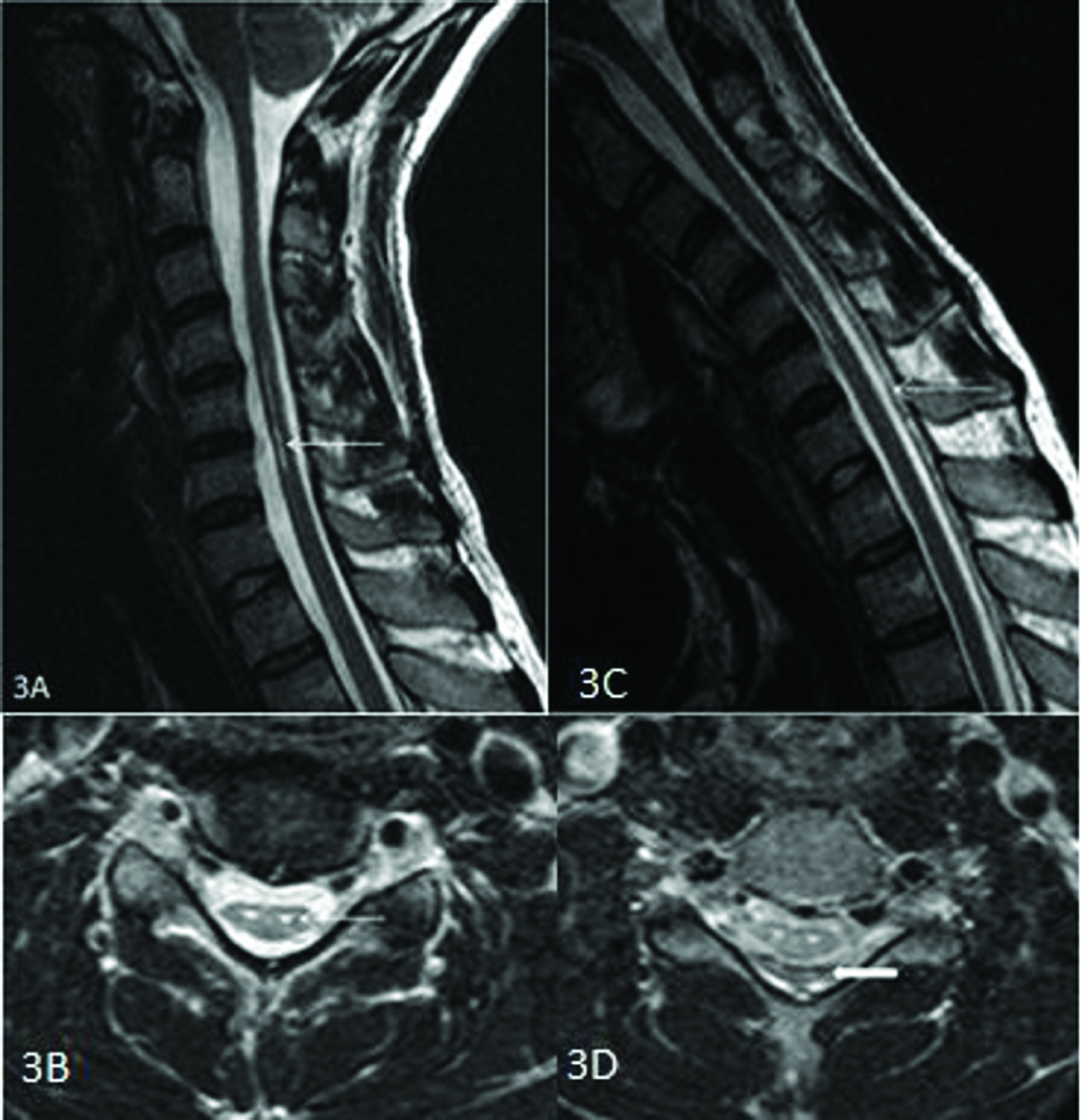
A 28-year-old male referred as anterior spinal muscular atrophy presented with weakness of right forearm and hand for five years. He had history of recent onset of weakness of left upper limb. His weakness was accentuated on exposure to cold. No evidence of sensory loss was noted. Routine MRI of cervical spine showed kyphotic curvature of spine, cord atrophy from C4 to C7 vertebral levels and linear hyperintensities of the cord in the region of anterior horn cells on T2 weighted images which appeared as an Owl’s eye in axial section [Table/Fig-3a,b]. Considering the age, pattern of involvement and anterior horn cell involvement flexion MRI was performed to rule out Hirayama disease. Flexion MRI revealed detachment of posterior dura from the lamina compressing the spinal cord against vertebral body, enlarged posterior epidural space with engorged epidural veins [Table/Fig-3c,d].
30-year-old male with Hirayama disease [Case 1] T2 w Sagittal (A) and axial (B) section in neutral position MRI shows mild cord atrophy at C6 and C7 levels (thin arrow) and posterior dural detachment in the lateral 2/3rd of lamina bilaterally (block arrow). T2 w Sagittal (C) and axial (D) section in flexion MRI shows posterior dural detachment (thin arrow), compression of cord against vertebral body (curved arrow) and enlarged posterior epidural space with engorged epidural veins (block arrow)
28-year-old male with hirayama disease [Case 2] T2w Sagittal (A) section in neutral position MRI shows altered curvature of spine (yellow line), mild cord atrophy at C5 and C6 vertebral levels, mild posterior dural detachment (thin arrow).T2w Axial (B) section in neutral MRI shows asymmetric cord flattening, complete detachment of posterior dura from lamina with prominent epidural vein [thin arrow]. T2w Sagittal (C) and axial (D) section in flexion MRI shows anterior displacement of posterior dura (thin arrow), compression of spinal cord against vertebral body and enlarged posterior epidural space with engorged epidural veins (block arrow)
25-year-old male with Hirayama disease [Case 3] T2w Sagittal (A) section in neutral position MRI shows kyphotic curvature of spine, mild cord atrophy,linear intramedullary hyperintensities from C4 to C7 vertebral levels (thin arrow). T2w Axial (B) section in neutral MRI shows, asymmetric cord flattening and owl’s eye appearance (thin arrow). T2w Sagittal (C) and axial (D) section in flexion MRI shows anteriorly displaced dura (thin arrow) with enlarged posterior epidural space, compression of spinal cord against vertebral body and enlarged posterior epidural space with engorged epidural veins (block arrow)
Discussion
Hirayama disease is named after Hirayama who had reported this disease in 1959[1]. It is a benign motor neuron disorder that typically affects the distal upper extremity from the C7 to T1 myotomes although C4 to C6 myotomes can also be involved [2]. The pattern of involvement is unilateral in most cases although bilateral asymmetric involvement is not uncommon. Bilateral symmetric involvement is rare [3]. Young males in their second or third decade are predominantly affected [4]. The disease typically spares brachioradialis and hence it is called oblique amyotrophy. Characteristically, the weakness gets accentuated on exposure to cold [5]. The disease has a progressive stage which lasts for three to five years and then it reaches a stationary stage.
Pathogenesis is constantly debated. Cervical dura is normally slack and consists of numerous transverse folds when neck is in extension. On flexion of neck the length of the cervical canal increases 5cm in posterior wall and the increased length is compensated by these transverse dural folds by becoming stretched [6]. In patients with Hirayama disease, there is disproportionate growth between vertebral column and dura mater. Therefore, when these patients flex their neck, the increased cervical spinal canal length is not compensated by the dura due to lack of these transverse folds. The dura becomes taut and detaches itself from the lamina.The detached dura shifts anteriorly and causes compression of cord against vertebral body [5]. When this cord compression is prolonged, microcirculatory disturbance occur in anterior horn cells region leading to ischemia and finally necrosis. In chronic disease, cord atrophy will occur [7].
It has been described in literature that a few findings in routine MRI of cervical spine should raise the suspicion of Hirayama disease in proper clinical setting [7]. They are abnormal cervical curvature, cord atrophy, asymmetric spinal cord flattening, intramedullary T2 hyperintensity and posterior dural detachment from lamina. Guigui et al., described the method of assessing cervical spine curvature. Normally the posterior aspects of C3 to C7 vertebral body do not cross the line drawn vertically along the dorsal aspects of C2 vertebral body through to C7 vertebral body. If the dorsal aspects of C3 to C6 vertebral bodies seem to touch or cross this vertical line, there is alteration in the cervical spine curvature [8].
Flexion MRI of cervical spine reveals posterior dural detachment from lamina with anterior shift causing spinal cord compression, enlarged posterior epidural space with engorged epidural veins.The posterior epidural space is a crescent shaped space which appears isointense in T1 weighted and hyperintense in T2 weighted images. Uniform enhancement of the space on postcontrast has been described [9].
Dural displacement was found to be more prominent in younger patient with progressive disease. The displacement may gradually decrease with increasing age and may not be present in patients who have reached a stable chronic stage [10].
Treatment of Hirayama disease is usually conservative. Neck flexion is avoided during progressive stage by application of a soft cervical collar and it has shown to arrest progression. Surgical intervention like cervical decompression and fusion with or without duraplasty may be advocated in selected patients [11].
Conclusion
Hirayama disease is a frequently undiagnosed condition with simple and inexpensive treatment. Clinicians must have a high index of suspicion of Hirayama disease when a young male presents with distal upper extremity weakness. Dynamic flexion MRI is the investigation modality of choice which reveals the typical features of the disease and clinches the diagnosis.
[1]. M Raval, R Kumari, AA Dung-Dung, B Guglani, N Gupta, R Gupta, MRI findings in Hirayama diseaseNeuroradiology. 2010 20:245-49. [Google Scholar]
[2]. KM Hassan, S Hirdesh, J Atul, Clinical and radiological profile of Hirayama disease: A flexion myelopathy due to tight cervical dural canal amenable to collar therapy.Ann Indian Acad Neurol. 2012 15(2):106-12. [Google Scholar]
[3]. B Yin, L Liu, DY Geng, Features of Hirayama disease on fully flexed position MRI.J Int Med Res 2011 39(1):222-28. [Google Scholar]
[4]. T Shruti, RG Sood, J Anupam, S Dinesh, M Sushma, A Neeti, Hirayama disease in unilateral and bilateral forms-3 case reports:The Egyptian Journal of Radiology and Nuclear Medicine 2013 44:291-95. [Google Scholar]
[5]. K Hirayama, Juvenile muscular atrophy of distal upper extremity (Hirayama disease): Focal cervical ischemic poliomyelopathyNeuropathology. 2000 20:91-4. [Google Scholar]
[6]. CJ Chen, CM Chen, CL Wu, LS Ro, ST Chen, TH Lee, Hirayama Disease: MR DiagnosisAJNR Am J Neuroradiol 1998 19:365-68. [Google Scholar]
[7]. CJ Chen, HL Hsu, YC Tseng, RK Lyu, CM Chen, YC Huang, Hirayama Flexion Myelopathy: Neutral-Position MR Imaging Findings—Importance of Loss of AttachmentRadiology. 2004 231(1):39-44. [Google Scholar]
[8]. P Guigui, M Benoist, A DeburgeDeburge, Spinal deformity and instability after multilevel cervical laminectomy for spondylotic myelopathySpine. 1998 23:440-47. [Google Scholar]
[9]. D Gandhi, M Goyal, PR Bourque, R Jain, Case 68: Hirayama DiseaseRadiology. 2004 230:692-96. [Google Scholar]
[10]. MS Lin, WM Kung, WT Chiu, RK Lyu, CJ Chen, TY Chen, Hirayama diseaseJ Neurosurg Spine 2010 12(6):629-34. [Google Scholar]
[11]. S Chiba, K Yonekura, M Nonaka, T Imai, H Matumoto, T Wada, Advanced Hirayama Disease with Successful Improvement of Activities of Daily Living by Operative Reconstruction.Internal Medicine 2004 43:79-81. [Google Scholar]