Chronic hepatitis is defined as symptomatic, biochemical or serologic evidence of continuing or relapsing hepatic disease for more than six months, with histological documentation of inflammation and necrosis.
In the forty years since the publication of the initial classification there has been an impressive progress in the understanding of chronic hepatitis, including the recognition of various causes of chronic hepatitis which are viral, auto-immune or drugs associated. Concurrent to that, progress has been made in the therapy of the chronic hepatitis with novel approaches in the treatment. Both these facts have led to description and classification of the entity under three components i.e. aetiology, grading and staging. Presently there are five established systems of scoring the liver biopsies for chronic hepatitis. These are the Knodell HAI [5], the Scheuer scoring system [6], Ishak’s system [7], Metavir system [8] and Ishak modified HAI [9]. With all their merits, demerits and limitations these five scoring system are routinely used by various hepato pathologists. This histological activity and staging is important for the patient and the clinician because it provides a measure of severity of the hepatitis at the time of biopsy and also helps in assessing effect of the treatment which does not always correlate to abnormal liver function tests [10–12].
In earlier reports authors have tried to compare two or more scoring systems or parameters in assessing the necroinflammatory activity and fibrosis in liver biopsies from patients with chronic hepatitis [9,13–16]. To the best of our knowledge there is no previous study in which five scoring systems have been compared on the same liver biopsy. This study was undertaken to compare the five scoring systems in assessing grading and staging of chronic liver diseases due to hepatitis B or C and their problems and pitfalls.
Materials and Methods
The present study included liver biopsies from 25 patients with chronic viral hepatitis. Out of these 18 were positive for hepatitis B and 7 were for hepatitis C markers. Liver biopsies that were at least 1.5cm in length and had 3-5 portal tracts were included in the study. Three to four micron thick sections from paraffin blocks were stained with Haematoxylin and Eosin, Reticulin and Masson’s Trichrome stain. Other stains like Von Gieson, Perl’s and Shikata’s Orcein were used where ever applicable. Coded histological sections of liver biopsies were scored independently by three different histopathologists using the Knodell HAI, the Scheuer scoring system, Ishak’s system, Metavir system and Ishak modified HAI. A consensus score was calculated after discussion on the points of differences for comparison of various classification and statistical calculations [Table/Fig-1]. For statistical calculations and comparison descriptive terms like mild, moderate and severe in classification like Scheuer [6] and Ishak’s 1994 [7] were taken as 1, 2 and 3 respectively.
Scores of grading and staging of liver biopsies from chronic hepatitis patients by various scoring systems
| SN | KNODELL SCORE | SCHEUER SYSTEM | ISHAK’S SYSTEM | METAVIR SYSTEM | ISHAK MODIFIED HAI |
|---|
| Necroinfla-mmatory Activity (Grading) | Fibrosis (Staging) | Necro-inflammatory Activity (Grading) | Fibrosis(Staging) | Necro-inflammatory Activity (Grading) | Fibrosis (Staging) | Necro-inflammatory Activity (Grading) | Fibrosis (Staging) | Necro-inflammatory Activity (Grading) | Fibrosis (Staging) |
|---|
| 1 | 11/18 | 4/4 | 8/8 | 4/4 | Very Marked | Marked | 3/3 | 4/4 | 15/18 | 5/6 |
| 2 | 9/18 | 1/4 | 5/8 | 1/4 | Moderate | Mild | 2/3 | 1/4 | 12/18 | 2/6 |
| 3 | 12/18 | 3/4 | 7/8 | 3/4 | Moderate | Marked | 3/3 | 3/4 | 14/18 | 4/6 |
| 4 | 13/18 | 3/4 | 8/8 | 3/4 | Moderate | Marked | 3/3 | 3/4 | 15/18 | 5/6 |
| 5 | 14/18 | 4/4 | 8/8 | 4/4 | Very Marked | Very Marked | 3/3 | 4/4 | 17/18 | 6/6 |
| 6 | 14/18 | 4/4 | 8/8 | 4/4 | Very Marked | Very Marked | 3/3 | 4/4 | 17/18 | 6/6 |
| 7 | 9/18 | 3/4 | 7/8 | 3/4 | Moderate | Marked | 2/3 | 3/4 | 11/18 | 5/6 |
| 8 | 5/18 | 1/4 | 3/8 | 1/4 | Mild | Marked | 1/3 | 1/4 | 3/18 | 2/6 |
| 9 | 6/18 | 1/4 | 3/8 | 1/4 | Mild | Mild | 1/3 | 1/4 | 4/18 | 1/6 |
| 10 | 1/18 | 0/4 | 1/8 | 0/4 | Mild | Mild | 0/3 | 0/4 | 1/18 | 0/6 |
| 11 | 1/18 | 0/4 | 1/8 | 0/4 | Mild | Mild | 0/3 | 0/4 | 1/18 | 0/6 |
| 12 | 4/18 | 1/4 | 3/8 | 1/4 | Mild | Moderate | 2/3 | 1/4 | 4/18 | 2/6 |
| 13 | 9/18 | 3/4 | 6/8 | 3/4 | Moderate | Marked | 2/3 | 3/4 | 10/18 | 4/6 |
| 14 | 13/18 | 3/4 | 8/8 | 3/4 | Moderate | Marked | 3/3 | 3/4 | 15/18 | 5/6 |
| 15 | 8/18 | 2/4 | 6/8 | 2/4 | Moderate | Marked | 2/3 | 3/4 | 10/18 | 4/6 |
| 16 | 11/18 | 4/4 | 8/8 | 4/4 | Very Marked | Marked | 3/3 | 4/4 | 15/18 | 5/6 |
| 17 | 9/18 | 2/4 | 5/8 | 1/4 | Moderate | Mild | 2/3 | 1/4 | 12/18 | 2/6 |
| 18 | 12/18 | 3/4 | 7/8 | 3/4 | Marked | Marked | 3/3 | 3/4 | 14/18 | 4/6 |
| 19 | 9/18 | 3/4 | 7/8 | 3/4 | Moderate | Marked | 2/3 | 3/4 | 11/18 | 5/6 |
| 20 | 5/18 | 2/4 | 3/8 | 1/4 | Mild | Moderate | 1/3 | 1/4 | 3/18 | 2/6 |
| 21 | 14/18 | 4/4 | 8/8 | 4/4 | Very Marked | Very Marked | 3/3 | 4/4 | 17/18 | 6/6 |
| 22 | 14/18 | 4/4 | 8/8 | 4/4 | Very Marked | Very Marked | 3/3 | 4/4 | 17/18 | 6/6 |
| 23 | 13/18 | 3/4 | 8/8 | 3/4 | Marked | Marked | 3/3 | 3/4 | 15/18 | 5/6 |
| 24 | 6/18 | 2/4 | 3/8 | 1/4 | Mild | Mild | 1/3 | /41 | 4/18 | 1/6 |
| 25 | 1/18 | 0/4 | 1/8 | 0/4 | Mild | Mild | 0/3 | 0/4 | 1/18 | 0/6 |
Statistics - The kappa test (K) was used to find the significance of agreement among various scoring systems for grading and staging of chronic hepatitis. P-values of ≤ 0.5 were taken as critical level of significance.
Results
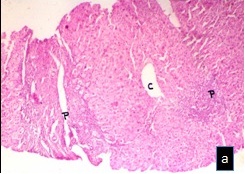
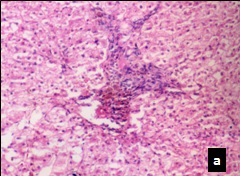
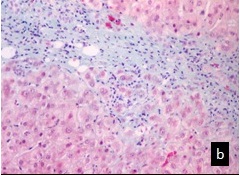
Twenty five patients were included in the study. There were 15 males and 10 females (Male: Female ratio = 3: 2). Their mean age was 51.24 years (range= 32 years to 69 years). On histological examination, hepatocytes showed degenerative changes with varying grades of necrosis (spotty and confluent) [Table/Fig-2a,b,candd,3a,b,dandd]. Widening of portal tracts with varying severity of mononuclear inflammatory infiltrate and interface hepatitis was observed [Table/Fig-4a,bandd,5a,b,candd,6a–d]. Fibrosis appeared as periportal, portal-portal and portal-central septa [Table/Fig-5a–d,6a–d]. Grading of necroinflammatory activity and staging of fibrosis was carried out in these cases according to the different scoring systems [5–9] [Table/Fig-1].
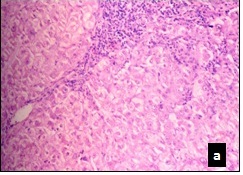
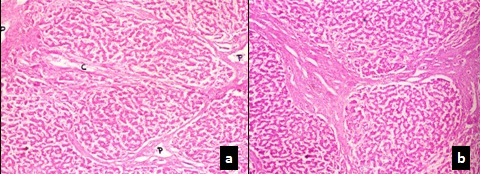
Liver biopsy showing distorted liver architecture with bridging necrosis and fibrosis. C-Central vein and P- Portal tract (H & E X 40)
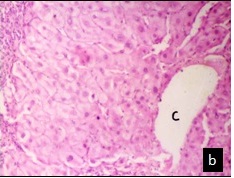
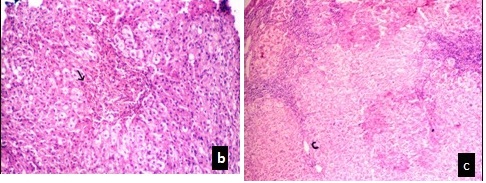
Higher magnification showing ground glass appearance of hepatocytes with interface hepatitis (H & E X 100)
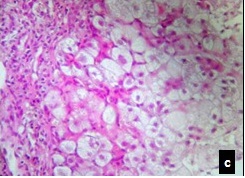
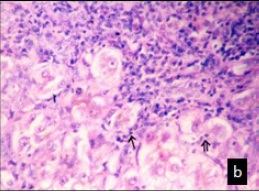
Higher magnification showing mainly interface hepatitis (H & E X400)
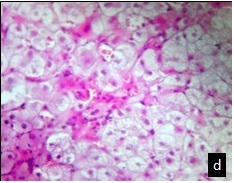
Lobular inflammation with spotty necrosis. (H & E X 400)
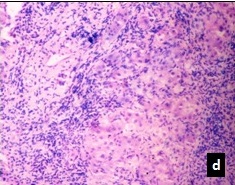
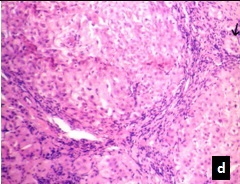
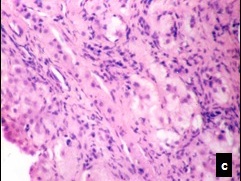
Portal tract with mild interface hepatitis. (H & E X40)
Moderate interface hepatitis with lobular inflammation. (H & E X40)
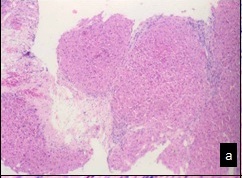
Interface hepatitis with bridging necrosis, lobular inflammation and spotty necrosis. (H & E X40)
Moderate bridging necrosis with pseudo-lobular pattern (H & E X 40)
Porto-caval bridging necrosis (H & E X100)
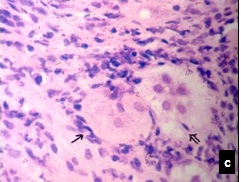
Entrapped hepatocytes showing peripolesis (↑) and emperipolesis (←) (H & E X 400)
Severe interface hepatitis with marked lobular inflammation (H & E X 100)
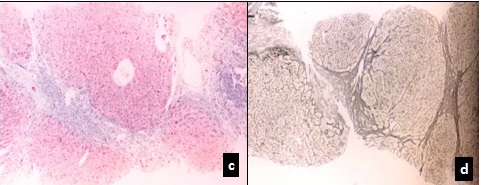
Marked bridging necrosis with early fibrosis highlighted by Mason trichrome stain (MT X 40)
Higher magnification of 5 A detailing increased fibrosis and interface hepatitis (MT X 100)
Early fibrosis with entrapped hepatocytes. (H & E X 100)
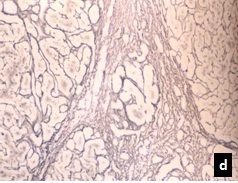
Loss of architecture highlighted by reticulin stain (X 100)
Incomplete bridging fibrosis- grade-5. C-Central vein and P- Portal tract (H & E X 40)
Fibrosis and micro-nodule formation by Masson trichrome and reticulin staining respectively (X 40)
The relative comparisons of all the biopsies according to the different scoring system have been tabulated [Table/Fig-1]. The results of the various scoring systems were compared with each other and a significant agreement was found by kappa statistics for both grading (p < 0.001) as well as staging (p < 0.001).No significant intraobserver difference was observed. Lobular activity was the only parameter that showed some discrepancy.
Discussion
Chronic hepatitis is defined as symptomatic, biochemical or serological evidence of continuing or relapsing hepatic disease for more that six months with histologically documented inflammation, necrosis and fibrosis [10]. The morphological pattern of injury to the liver tissue may vary for each case. It was observed by pioneers in the field of hepatopathology that not all cases of chronic hepatitis showed a steady downhill course [17]. The fact which was utilized by de Grote and his fellow researchers in 1968, to divide the entity into chronic persistent and chronic aggressive hepatitis [1]. However, in the last two decades; after the discovery of various aetiological agents it was finally agreed to classify it under three primary components of etiology, grading and staging. Common causes leading to chronic hepatitis are viral, auto-immune, alcoholic, drug induced and cryptogenic.
The Knodell histology activity index (HAI) published in 1981 was the first system of its type and widely regarded as the benchmark for objective, semi-quantitative, reproducible description of the various morphological lesions of chronic hepatitis [5]. Most frequently cited criticism for this system were use of discontinuous value scale in all four categories, reason for which has not been explained in the original paper itself and the sum of necroinflammatory (interface hepatitis) and fibrosis scores that does not distinguish ongoing hepatitis from the parenchymal remodeling and fibrosis. These problems were also encountered in the present study. Many experts such as Desmet et al., have proposed that only first three components of Knodell’s scoring system should be included for scoring the histological activity whereas the fourth component which is fibrosis should be used for staging the disease [18]. In the present study separation of necroinflammatory activity score from the stage of fibrosis in Knodell’s scoring system was done in order to compare it with other scoring systems.
Scoring system given by Scheuer in 1991 was given for chronic viral hepatitis but like Knodell, it is universally applied for non viral hepatitis cases as well [6]. The main advantages of this system are that it is less complicated than the HAI scoring system, there is use of a continuous scale, plus it gives the portal and lobular components equal weightage and groups the periportal and portal lesions into a single category. But the main problem with this system was that it produced a narrower range of potential scores for necroinflammatory activity. This limits its usefulness in the context of monitoring response to the treatment in the clinical trials [19].
Scoring system introduced in 1994 by Ishak, promoted the use of descriptive terminology for activity and fibrosis, rating the different elements of activity as either present or absent; when present; a degree of severity is stated. Seven various investigators have employed this particular scoring system to assess HAI in chronic Hepatitis-B asymptomatic carriers with good results [13,14,19].
The French Metavir co-operation study group in 1996 proposed a comprehensive but complex system for histological evaluation of hepatitis-C associated chronic liver disease [7]. The final score in this system reflects the combined rating for focal lobular necrosis, portal inflammation, piecemeal necrosis and bridging necrosis.
A recent modification of the Knodell’s HAI, commonly referred as Ishak’s modified HAI introduced in 1995 provides consecutive scores for well defined lesions within four separate categories that are added together for the activity grade [8]. Two main problems encountered with this system were use of 10X objective for the evaluation of necroinflammatory foci leading to a problem concern of reproducibility as the size of the field may vary among microscopes.
There were some problems that were identified in this study regarding the usage of various scoring systems in case of chronic hepatitis. First problem observed with use of histological scoring systems was in assigning scores for lobular activity. As in Knodell scoring system, lobular activity is assigned in the form of ballooning degeneration [5], whereas in Ishak’s system lobular activity is graded in the form of spotty necrosis [7]. This caused disparity in comparing this parameter as in most of our biopsies of chronic hepatitis, degeneration of hepatocytes was seen throughout the lobules that gave a higher score in the Knodell scoring but there was no associated spotty necrosis or focal inflammation that in turn gave a lower score in Ishak’s scoring system.
In chronic hepatitis C infection, portal inflammation is usually more marked as compared to the lobular activity. Marked portal inflammation in the absence of bridging necrosis caused difficulty in assigning a category according to the Ishak’s scoring system in all such cases of chronic hepatitis in this study [20]. Besides,the numbers generated do not represent measurements of a continuous variable. Instead, they represent different categories of severity. An exclusive focus on the global or summary score for a biopsy may lead one to overlook the contribution of the individual components with clinical significance [19].
The second problem, was of observer variation, though statistically insignificant in obtaining reproducible results even when scoring systems were applied by the experts. These findings were similar to earlier reports [21,22]. It was found that in general, that fibrosis scoring has better conformity rather than the necroinflammatory scoring. However, this problem was rectified in present study by a prior discussion in details regarding how to apply the scoring systems before embarking upon the study. The current study found that a healthy discussion even during the study over the contentious areas in the histological slides which were giving disparity and frequent clinicopathological meetings and interactive sessions helped to instill conformity of a particular scoring system. Earlier studies reported that intraobserver error could be reduced if the individual case slides are reviewed by more than one hepato-pathologist [21, 22].
The third problem in the scoring of liver biopsies was of sampling errors. This variation can affect both the parameters in the scoring sheet as small areas of necrosis can be present in otherwise relatively quiescent cirrhosis and different degree of fibrosis can be present in different areas in primary biliary cirrhosis and primary sclerosing cholangitis [19]. This however can be minimized by the discussion between the gastroenterologist /physician in charge and the reviewing hepato-pathologists before the biopsy has been taken.
The various scoring systems have their advantages and disadvantages [17,20,21]. There is none at present, which employs all clinical, aetiological, and histological information available. The diagnosis statement should be an aetiological diagnosis which takes into consideration all the serological and immunohistochemical data available. A verbal approximation of the necroinflammatory activity and fibrosis stage (minimal, mild, moderate, or severe) should be applied to the aetiological diagnosis. The present study also emphasizes the need to assess individual components of the inflammatory activity rather than concentrating on overall score by over enthusiastic pathologists and physician commenting upon the overall outcome and prognosis of the patient. Therefore, a detailed report encompassing these approaches may lead to a better understanding, approach and consequently better application of therapeutic intervention by the physician in charge.
According to Hubscher, the system that is most appropriate for clinical practice may not be most informative for investigative work. The choice of systems depends to a large measure on whether it would be used for routine clinical work or for research purposes [19]. The more detailed systems like Knodell HAI and Ishak Modified HAI better suited for research purposes. For routine clinical work, these systems are cumbersome and more liable to generate inter and intra-observer differences [16,22] especially among pathologists who are not exposed to large number of liver biopsy specimens in routine practice. The results of this study shows good correlation among all these scoring systems, the simpler systems like the METAVIR, Scheuer System could be used for routine reporting and still be useful to the clinician for follow-up of patient.
Conclusion
It can be concluded that all the scoring systems are almost equally good for grading and staging in the hands of an experienced hepatopathologists and in order to obtain meaningful, reproducible results; hepatopathologists and the hepatologists should work in conjunction with each other. Despite advances in other diagnostic techniques, liver biopsies with their traditional descriptive reports (especially specific comments relating to the etiology, necroinflammatory activity and fibrosis) remains the basis to assess for the prognosis and treatment of the patients. If scoring has been employed a concerted effort should always be done to indicate clearly how the scores have been achieved by means of detailed descriptions.