Rehabilitation of Digital Defect with Silicone Finger Prosthesis: A Case Report
Deepesh Saxena1, Sunit Jurel2, Ajay Gupta3, Manu Dhillon4, Divya Tomar5
1 Senior Lecturer, Department of Prosthodontics, D.J. College of Dental Sciences and Research, Modinagar, India.
2 Assistant Professor, Department of Prosthodontics, Faculty of Dental Sciences, King Georges Medical University, Lucknow, India.
3 Professor & Head, Department of Prosthodontics, D.J.College of Dental Sciences and Research, Modinagar, India.
4 Reader, Department of Oral Medicine and Radiology, ITS Centre for Dental Studies and Research, Ghaziabad, India.
5 Senior Lecturer, Department of Pedodontics and Preventive Dentistry, SBB Dental College, Ghaziabad, India.
NAME, ADDRESS, E-MAIL ID OF THE CORRESPONDING AUTHOR: Dr. Manu Dhillon, Reader, Department of Oral Medicine and Radiology, ITS Centre for Dental Sciences and Research, Meerut-Delhi Road, Muradnagar, Ghaziabad, Uttar Pradesh, India.
Phone: 09219510522, E-mail : drmanudhillon@yahoo.co.in, drmanudhillon@gmail.com
Patients with acquired defects often had severe trauma which leads to psychological instability, functional loss and poor aesthetics. Digital defects threaten the integrity of one’s self esteem and also leads to a reduced and compromised function. A well fitted and colour matched finger prosthesis can make a patient feel a capable person and not a handicap. This article describes a technique for fabrication of custom made finger prosthesis with a silicone elastomer. The customization of the prosthesis leads to a better fit and retention. An excellent shade matching is achieved by the use of intrinsic colours. The other advantages of using silicone as a material of choice for prosthesis fabrication are also discussed.
Colour matching, Finger, Prosthesis, Silicone elastomer
Case Report
A 55-year-old male patient came to the Prosthodontic department with a chief complaint of loss of finger. On history, taking it was revealed that the patient is a farmer and was bitten by a snake while working in his farm four months back due to which his finger had to be resected in order to save his life. The patient was very depressed because of the mental and physical trauma that he had undergone due to the loss of his finger [Table/Fig-1].
Amputated finger of right hand

The patient was made aware of the treatment i.e. the fabrication of artificial finger prosthesis. The patient readily accepted the treatment; however he was a little anxious. Counselling of the patient was done so as to make him comfortable during the treatment and was told about the limitations of the prosthesis.
Technique
An alginate impression of the affected hand was made. For making the impression the patient’s hand was lubricated with petroleum jelly and a cardboard box was selected which was bigger than patient’s hand. A thin mix of alginate was poured inside the box and the patient was asked to place the ventral aspect of his hand over the mix to record the impression of the ventral side of his hand. Rest of the mix was then poured over the dorsal surface of the hand and whole of the hand was covered with alginate [Table/Fig-2]. A thick layer of plaster was placed over alginate to give strength to the impression so that it does not tear when the patient removes his hand [Table/Fig-3]. The patient was asked to slowly move his fingers and try to pull his hand outside to obtain the impression [Table/Fig-4]. The impression was poured in dental stone (Kalstone, Kalabhai Dental Pvt Ltd) and a positive replica of the hand was made.
A wax pattern of the resected finger was made. For this purpose “donor technique” was used in which impression of another person whose finger had no congenital or developmental defect and whose size and shape of the hand matched with that of the patient was made and poured in wax (Modeling wax, Dental products of India Ltd) .
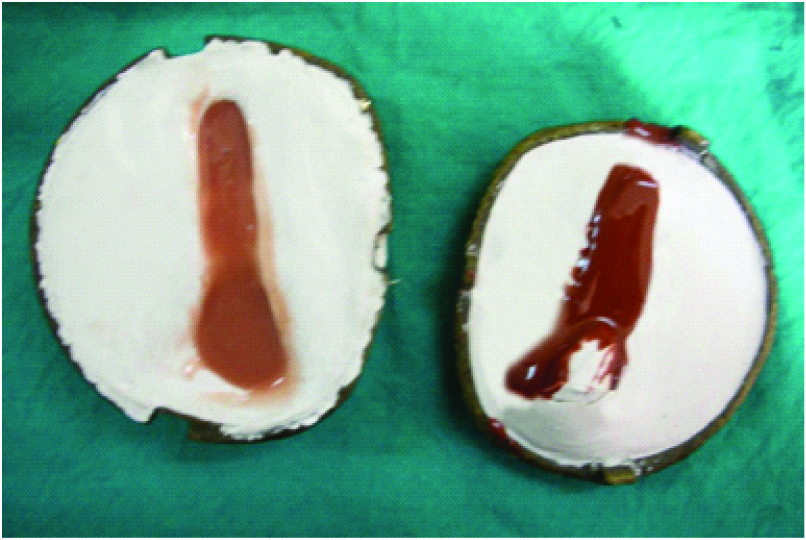
A glove type wax pattern was made from the donor wax model which was then customised according to the patient’s resected finger [Table/Fig-5]. After the fit of the wax pattern was checked, flasking and wax elimination of the wax pattern was done [Table/Fig-6].
On the day of packing, the patient was called and colour matching was done in front of the patient in natural daylight and other artificial light sources. Different shades were selected for characterization of ventral and dorsal surfaces of the hand and intrinsic staining was done [Table/Fig-7,8].
The silicone material (Cosmesil RTV) was packed in two parts so as to obtain different shades for dorsal and ventral surfaces [Table/Fig-9]. The flask was closed and curing was done.
The prosthesis was then retrieved and finished with a sharp blade. Nail was painted on the finger and then inserted on patient’s hand. An acceptable and satisfactory shade matching was achieved.
A ring was placed over the prosthesis which provided an additional retention to the prosthesis as well as it served a decorative purpose [Table/Fig-10]. The patient was happy and satisfied with the prosthesis.
Following home care instructions regarding the prosthesis were given to the patient:-
- Avoid exposure of prosthesis to high temperatures.
- Wash the prosthesis with antibacterial soap and brush.
- Remove the prosthesis during sleep.
Alginate impression of the affected hand

Alginate impression reinforced with a layer of plaster to give strength

Impression surface of the affected hand


Flasking of the wax pattern

Colour matching of the dorsal aspect

Colour matching of the ventral aspect
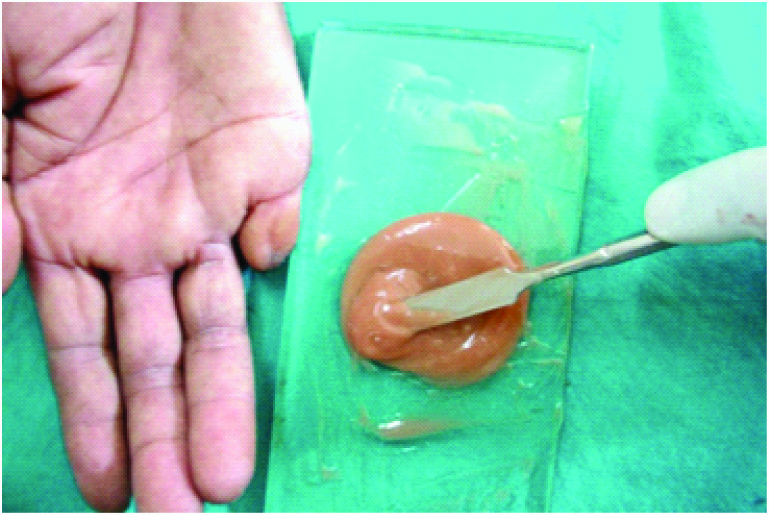
Packing of the silicone into the mould
Finger prosthesis with decorative ring

The patient came to the department after a period of one month and was psychologically very motivated because now he was socially more accepted.
Discussion
Finger and partial finger loss are one of the most commonly encountered hand losses due to trauma or congenital malformations [1]. Some of these losses can be treated by microsurgery where the reimplantation of the lost part is done. However, it is not possible in every case due to cost factor and unwillingness of the patient [2]. Under these circumstances artificial finger prosthesis can be given which can greatly enhance the psychology of the patient [3]. Replacement of a missing individual finger requires great skill and understanding because the expectations of the patient regarding the aesthetics of the prosthesis are quite high. The materials used in fabrication of artificial prosthesis mainly include polyvinyl chloride and silicone elastomers. The poly vinyl chloride is easily discoloured or stained during regular use [4]. In this case the material chosen was a silicone elastomer because of its excellent aesthetics, flexibility, elasticity and life like appearance [5,6]. It improves the hydration of the stratum corneum layer of the skin [7] and also has adequate tear strength. To replace a finger nail, it can be painted on the finger, made with acrylic or artificial nails can be incorporated.
The retention of finger prosthesis is achieved by suction between the stump and the prosthesis. However, if this suction is not sufficient, grooves can be made in the positive model to enhance suction [8]. Also, the use of adhesives is recommended to enhance the retention of the prosthesis The disadvantage of adhesives are skin reactions and improper hygiene of the site where it is applied [Table/Fig-11]. In this case an additional retention was provided by using a decorative ring placed on the artificial finger. Another method of gaining retention is the use of magnets. The two opposite poles of the magnet help to secure the prosthesis, whereas the use of implant retained finger prosthesis provides aesthetics as well as restores the functional activity of the prosthesis.
Advantages and disadvantages of silicone finger prosthesis [2,3,5,6,8]
| Advantages | Disadvantages |
|---|
| Helpful in rehabilitation of the defect where surgery is not possible | Degradation of the prosthesis can occur if exposed to high temperatures |
| It provides with excellent esthetics | Exposure to sunlight (UV light) for long hours should be avoided |
| Easy retention of the prosthesis is achieved | Sometimes skin reactions are seen from adhesives used for retention of prosthesis |
| It has good elastic properties | It is a non functional prosthesis |
| Does not stain with ink and food colorants | It is a removable prosthesis, therefore should be removed during the night |
| It gives an excellent fit | |
| It has a lifelike appearance | |
| It enhances patient’s confidence and his social acceptance | |
Conclusion
Traumatic loss of a finger or partial finger not only effects the form and function but also hurts the self confidence of the patient. It is essential to restore the form and function of the lost finger with an indiscernible prosthesis and to treat the psychological disorders of the patient. With the availability of advanced technology and materials it is possible to make a prosthesis that is made life-like. Well-fabricated finger prosthesis with good aesthetics greatly influences the psychology of the patient.
[1]. Pillet J, The aesthetic hand prosthesisOrthop Clin N Am 1981 12:961-70. [Google Scholar]
[2]. Wilson RL, Carter-Wilson MS, Rehabilitation after amputations in the handOrthop Clin N Am 1983 14:851-72. [Google Scholar]
[3]. Pilley MJ, Quinton DN, Digital prosthesis for single finger amputationJ Hand Surg Br 1999 24(5):539-41. [Google Scholar]
[4]. Michael J, Partial-hand amputation: prosthetic and orthotic management. In: Bowker JH, Michael JW [eds]Atlas of limb prosthetics: surgical, prosthetic and rehabilitation principles 1992 St. LouisCV Mosby:217-26. [Google Scholar]
[5]. Buckner H, Cosmetic hand prostheses- a case reportOrthotics and Prosthetics 1980 34(3):41-45. [Google Scholar]
[6]. Kanter CJ, The use of RTV silicones in maxillofacial prostheticsJ.Prosthet Dent 1970 24(6):646-53. [Google Scholar]
[7]. Burkhardt A, Weitz J, Oncologic applications for silicone gel sheets in soft-tissue contracturesAmer J Occu Ther 1990 45(5):460-62. [Google Scholar]
[8]. Herring HW, Romerdale EH, Prosthetic finger retention: a new approachOrthotics and Prosthetics 1983 37(2):28-30. [Google Scholar]