Introduction
Bronchial asthma affects 100-150 million people worldwide and approximately 180,000 deaths annually are attributed to asthma [1]. According to WHO, India is home to 15-20 million asthmatics. Asthma is a chronic inflammatory disorder of the airways characterized by recurrent episodes of wheezing, breathlessness, chest tightness and coughing due to reversible airway obstruction, cellular inflammation, mucus hypersecretion, airway remodeling, blood vessel proliferation and mucous gland hyperplasia and hypersecretion. The broncho-constrictor and inflammatory mediators of asthma include cytokines, chemokines, cysteinyl leukotrines, histamine, nitric oxide, PGD2 adhesion molecules, enzymes and kinases which are mostly regulated by NF-kB pathway. This pathway has now been recognized to be involved in asthma and mediates the complex inflammatory response in the airways therefore the agents that downregulates NF-kB pathway could have a potential efficacy against the disease [2].
The diagnosis of asthma is established by demonstrating reversible airway obstruction. Pulmonary Function Test (PFT) is the gold standard for evaluating airway obstruction and/or restriction. The FEVl/FVC ratio, also called Tiffeneau index, whose normal values are approximately 80%. This ratio is reduced in obstructive while normal in restrictive lung diseases. Reversibility is traditionally defined as a 15% or greater increase in FEV1 after two puffs of a b2 adrenergic agonist.
Medications to treat asthma can be classified as controllers or relievers. Controller drugs like corticosteroids keep asthma under clinical control by inhibiting airway inflammation by modulating cytokine and chemokine production, inhibiting eicosanoid synthesis, markedly inhibiting cellular infiltration in lung tissues and decreasing the vascular permeability [3], but its use is limited by the risk of local and systemic adverse effects. Relievers are medications used on an as-needed basis that act quickly to reverse bronchoconstriction and relieve its symptoms. They include rapid-acting inhaled and oral β2-agonists, inhaled anticholinergics, leukotriene modifiers, cromones and short-acting theophylline [3]. Immunotherapy by IgE antibody Omalizumab reduces exacerbations in patient with severe asthma and may improve bronchial hyper-reactivity helping in asthma control.
Bronchial thermoplasty is a treatment for severe asthma approved by the FDA in 2010 that involves the delivery of controlled therapeutic radiofrequency energy to the airway wall, thus heating the tissue leading to acute epithelial destruction and reducing the amount of oedema in the airway wall [4]. Non-pharmacologic alternative treatments including hypnosis, acupuncture, chiropraxy, breathing control, yoga and speleotherapy may be popular with some patients. However, placebo-controlled studies have shown that each of these treatments lacks efficacy and cannot be recommended. However, they are not detrimental and may be used as long as conventional pharmacologic therapy is continued.
In spite of voluminous literature on the subject, the treatment of bronchial asthma continues to be far from satisfactory. The available treatment options for bronchial asthma have major limitations due to low efficacy, associated adverse events, lack of disease modifying property and compliance issues. Therefore, there is a need to explore for new anti-asthmatic agents with extended pulmonary efficacy and minimal systemic side effects.
WHO has recognized herbal medicines as an essential building block for primary health care in developing countries like India. It has been reported in the past that 11-40% asthma patients use herbal medicines [5].
In recent years, turmeric, a spice used in Asian countries, has attracted the attention of researchers due to its reported effectiveness in inflammatory and other disorders. Curcumin, a natural product from the rhizomes of Curcuma longa (Turmeric), has a wide range of beneficial properties including anti-inflammatory, anti-oxidant, anti-rheumatic, anti-carcinogenic, anti-coagulant, anti-fertility, anti-diabetic, anti-bacterial, anti-protozoal, anti-viral, anti-fibrotic, hypolipidemic and hypoglycemic activities [6]. Curcumin modulates the inflammatory response by down-regulating intercellular signaling proteins, such as protein kinase C [7], modulating the activity of transcription factors like activating protein-1 (AP-1) and inhibiting NF-KB pathway which is involved in regulation of inflammation, cellular proliferation, transformation and tumourogenesis. Curcumin is thought to suppress NF-kB activation and proinflammatory gene expression by blocking phosphorylation of inhibitory factor l-kappa B kinase (I-rcB) [8], thereby subsequently suppressing cyclooxygenases, lipoxygenase pathways and iNOS expression. All these activities inhibit the production of the inflammatory cytokines, tumor necrosis factor-alpha (TNF-a), interleukins (IL-1,2,6,8,12) monocyte chemoattractant protein (MCP) and migration inhibitory protein. It also inhibits transcription factor products such as signal transducer and activator of transcription (STAT), PPAR-g and down-regulates Janus kinases [9].
Our study focuses on one of its best explored actions, the anti-inflammatory effects. There were only a few studies to explore the action of curcumin in asthma but all were with different methodologies and end points. Based on the anti-inflammatory properties, we hypothesized that curcumin could have an effective role in the treatment of asthma. Hence, the present comparative study has been designed to investigate the efficacy and safety of curcumin as an add-on therapy in mild-to-moderate bronchial asthma patients.
Materials and Methods
The present study was an open labelled, randomized, single centre study assessing the efficacy of orally administered curcumin capsules in addition to the normally prescribed medication for the treatment of asthma. Approval of Institutional Ethical Committee was obtained. Written informed consent was taken from all patients.
Human studies have showed that curcumin at doses ranging from 0.9 to 3.6 g/day for 1-4 months has been classified as ‘generally recognized as safe’ (GRAS) by the National cancer Institute and Food and Drug Administration but exhibited some adverse effects [10] . Thus, we selected a safe dose of 1gm i.e. 1000mg given in two divided doses [7,11].
Selection of the Patients
Inclusion Criteria
Bronchial asthma patients in the age group of 18 to 55 y of either sex who had a documented positive bronchodilator reversibility test with ≥15% improvement in FEV1 from 15 to 30 minutes after inhalation of at least 200 μg of salbutamol, patients who had never smoked/had left smoking since past three months; with prebronchodilator FEV1 values in range of 60-80%; with normal serum glutamic pyruvic transaminase (SGPT) and normal serum creatinine levels were included in the study.
Exclusion Criteria
Children, bronchial asthma patients who were currently smoking were excluded from the study. Patients with severe asthma, chest infections, bile duct obstruction (or history of gallstones), abnormal SGPT levels & serum creatinine values, those on warfarin or anti-platelet drugs were not included in the study. Pregnant females, patients having chronic bronchitis and/or emphysema, or patients suffering from concurent systemic diseases like cardiopulmonary, tuberculosis, pulmonary eosinophilia, bronchiectasis, cancer, congestive heart failure, hepatic dysfunction, neurological disorders and diarrheal disorders or having a hemoglobin level less than 10 g/dl were also excluded from the study.
Shows the demographic data i.e Mean age in years, the Male and Female population, Mean height in cms and Mean weight in kgs in each group which are comparable in both the groups
| Characteristics | Group A (Standard therapy for asthma) [n=30] | Group B (Standard therapy for asthma + Curcumin) [n=30] |
| Mean age±SD (years) | 31.73±2.18 | 31.46±1.94 |
| Female (%) | 16 (53.30%) | 14 (46.70%) |
| Male (%) | 14 (46.70%) | 16 (53.30%) |
| Mean height±SD (cm) | 163.23±6.81 | 162.36±8.32 |
| Mean weight±SD (kg) | 58.96±10.65 | 58.23±10.75 |
Compares the reduction in severity of asthma symptoms like dyspnea, wheezing, cough, chest tightness, nocturnal symptoms and total score in both the groups by one way ANOVA
| Group A(n=30) | Group B(n=30) | p value |
| Reduction in Dyspnoea (Mean±SD) |
| 0 visit to 1st visit | 0.63±0.55 | 0.53±0.50 | 0.444 |
| 0 visit to 2nd visit | 0.40±0.49 | 0.50±0.73 | 0.570 |
| 0 visit to 3rd visit | 0.23±0.43 | 0.23±0.43 | 1.00 |
| F= (3.22, 2.67), R squared = 0.03 |
| Reduction in Wheezing (Mean±SD) |
| 0 visit to 1st visit | 0.10±0.30 | 0.15±0.37 | 0.480 |
| 0 visit to 2nd visit | 0.00±0.00 | 0.10±0.30 | 0.080 |
| 0 visit to 3rd visit | 0.00±0.00 | 0.00±0.00 | 0.200 |
| F= (3.22, 2.67), R squared = 0.03 |
| Reduction in Cough (Mean±SD) |
| 0 visit to 1st visit | 0.56±062 | 0.40±0.56 | 0.250 |
| 0 visit to 2nd visit | 0.40±0.62 | 0.23±0.43 | 0.780 |
| 0 visit to 3rd visit | 0.23±0.43 | 0.20±0.40 | 1.00 |
| F= (3.02, 2.49), R squared = 0.27 |
| Reduction in tightness (Mean±SD) |
| 0 visit to 1st visit | 0.10±0.30 | 0.10±0.30 | 1.00 |
| 0 visit to 2nd visit | 0.10±0.30 | 0.10±0.30 | 1.00 |
| 0 visit to 3rd visit | 0.03±0.18 | 0.03±0.18 | 1.00 |
| F= (0.60, 0.60), R squared = 0.73 |
| Reduction in symptoms (Mean±SD) |
| 0 visit to 1st visit | 0.10±0.30 | 0.10±0.30 | 1.00 |
| 0 visit to 2nd visit | 0.06±0.25 | 2.01±0.82 | 0.160 |
| 0 visit to 3rd visit | 0.00±0.00 | 0.03±0.18 | 0.320 |
| F= (1.48, 1.84), R squared = 0.52 |
| Reduction in Total symptom score (Mean±SD) |
| 0 visit to 1st visit | 1.50±1.19 | 1.23±1.00 | 0.290 |
| 0 visit to 2nd visit | 0.86±0.89 | 0.93±0.94 | 0.770 |
| 0 visit to 3rd visit | 0.50±0.62 | 0.05±0.62 | 1.00 |
| F= (8.73, 5.31), R squared = 0.87 |
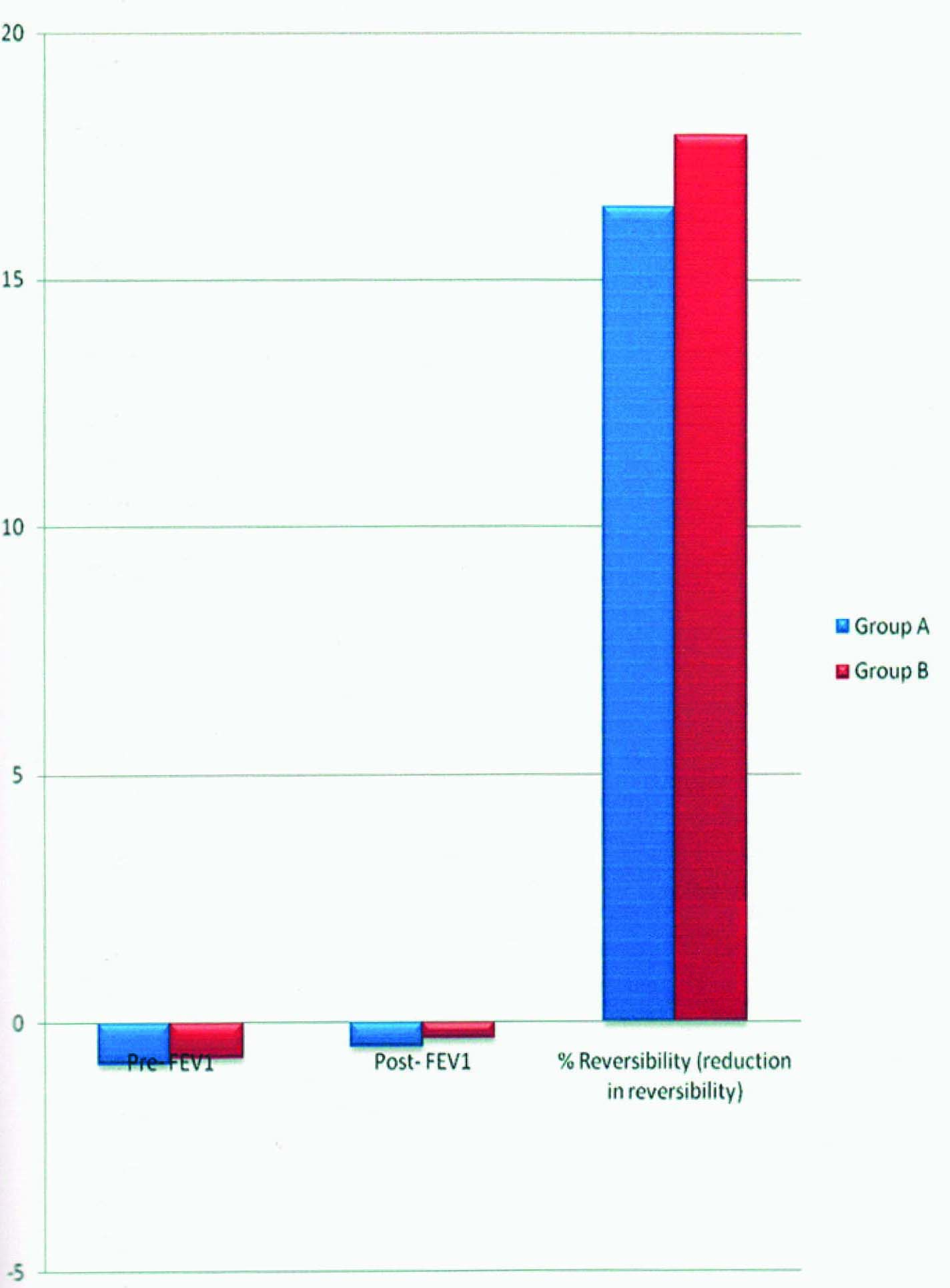
Compares the Pre-bronchodilator FEV1, Post-bronchodilator FEV1 and % reduction in Reversibility in both the groups by Paired ‘t’ test. All values are expressed as Mean±SD
* p< 0.05 indicates significant values
| Group A(n=30) | Group B(n=30) | p value |
| Pre-bronchodilator FEV1 (Mean±SD) |
| 0 visit to 1st visit | -0.18±0.32 | -0.10±0.36 | 0.040* |
| 0 visit to 2nd visit | -0.43±0.37 | -0.29±0.53 | 0.060 |
| 0 visit to 3rd visit | -0.83±0.63 | -0.72±0.69 | <0.001* |
| Pre-bronchodilator FEV1 (Mean±SD) |
| 0 visit to 1st visit | 0.96±0.38 | 0.25±0.50 | 0.010* |
| 0 visit to 2nd visit | -0.08±0.40 | 0.08±03.65 | 0.170 |
| 0 visit to 3rd visit | -0.50±0.66 | -0.33±0.76 | <0.001* |
| % reduction in Reversibility (Mean±SD) |
| 0 visit to 1st visit | 14.63±7.21 | 15.46±6.94 | <0.001* |
| 0 visit to 2nd visit | 16.16±5.18 | 16.26±8.21 | <0.001* |
| 0 visit to 3rd visit | 16.46±7.22 | 17.93±8.00 | <0.001* |
Comparing improvement of Hematological Parameters in both the groups (0 visit to 3rd visit)
* p< 0.05 indicates significant values
| Parameters | Group A (n=30) | Group B (n=30) | p value |
| Total leukocyte count (/mm3) | 906.66±1357.59 | 982.33±1974.89 | 0.010* |
| Neutrophils (%) | 6.83±7.19 | 4.23±7.29 | 0.020 |
| Lymphocytes (%) | 5.10±6.95 | 2.73±6.96 | 0.040 |
| Eosinophils (%) | 1.46±1.71 | 1.53±1.73 | 0.000* |
| ESR (mm/hr) | 6.33±6.38 | 6.73±4.59 | 0.000* |
Shows the incidence of adverse effects in both the groups in number and %
| ADR | Group A (n=30) | Group B (n=30) |
| Weight loss | 0(0%) | 0(0%) |
| Weight gain | 0(0%) | 3(10%) |
| Diarrhoea | 0(0%) | 0(0%) |
| Nausea | 0(0%) | 0(0%) |
| Decrease appetite | 1(3.33%) | 0(0%) |
| Headache | 1(3.33%) | 1(3.33%) |
| Back pain | 0(0%) | 0(0%) |
| Tremor | 0(0%) | 0(0%) |
| Insomnia | 2(6.66%) | 1(3.33%) |
| Hypertension | 0(0%) | 0(0%) |
| Other | 0(0%) | 0(0%) |
Shows the improvement in FEV1 values at 3rd visit i.e. on 30th day- Pre-bronchodilator FEV1, Post-bronchodilator FEV1 and % reduction in reversibility
Methodology
At initial visit, a comprehensive assessment comprising detailed medical history, a thorough clinical examination with special emphasis on respiratory system examination, hematological test (haemoglobin, TLC, DLC, ESR, C-reactive protein), biochemical test (SGPT, serum creatinine), urine analysis, chest x-ray and pulmonary function test (FEV1) were performed.
After a medical examination 77 subjects satisfying the inclusion criteria were recruited in the study and written informed consent was obtained from each of the patient. All the selected patients were randomized by a computer generated random number in either of the two groups:
Group A – Receiving standard therapy for bronchial asthma- Formonide Resicaps BD German Remedies (Zydus Cadila HealthcareLtd) [Budesonide 100 mcg, formoterol 6 mcg], Cap ABflo BD Lupin Laboratories Ltd [Acebrophylline 100 mg], Tab Montek LC hs Sun Pharmaceutical Industries Ltd (Montelukast 10 mg, levocetirizine 5mg) for 30d;
Group B – Receiving standard therapy for bronchial asthma as above + Cap Curcumin 500 mg BD daily for 30d.
The curcumin capsules were dispensed to patients by the prescribing doctor while other medications were purchased from the chemist. The curcumin capsules CUR- 500 (Curcumin 500 mg) were purchased by us from authorized manufacturer (M/s Indsaff & Charak International Private Limited, O/s Pahari Gate, Batala, Punjab -143505, India) and were provided free of cost to the study participants.
All the patients were followed up every tenth day for a period of one month. At each visit clinical symptoms like dyspnoea, wheezing, cough, chest tightness and nocturnal symptoms were assessed. Pulmonary function test (Spirometry): FEV1, blood Pressure, temperature, hematological test like Hb, TLC, DLC, ESR, C-Reactive Protein (CRP), biochemical tests like Serum Glutamic Pyruvic Transaminase (SGPT), serum creatinine and anthropometric measurements like height and weight were recorded from which Basal Metabolic Index (BMI) was calculated.
Spirometry - FEV1 was measured by a computerized spirometer RMS Medspiror (Platfurm Win 98, Version 1.0). It was performed by the same technician on all patients and with the same instrument to avoid bias. Spirometry is best performed with the patient seated. Patients who were anxious about the tests were reassured and counseled before starting the procedure. The pre bronchodilator FEV1 value was taken after careful explanation of the test accompanied by a demonstration. The best of three reproducible measurements was taken for analysis. The post-bronchodilator FEV1 value was assessed at 20 min after the inhalation of 200 μg salbutamol using a metered dose inhaler with a spacer device. The percentage of predicted values and the percent of difference between the pre-bronchodilator and post-bronchodilator values were calculated.
Hematological tests- Hb, TLC, DLC was analysed using autoanalyser MS-9, ESR was analysed using Westergren method and CRP was analysed using either latex agglutination or turbidimetry method.
The predefined primary endpoints were rapid symptomatic control clinically assessed by dyspnoea, wheezing, cough, chest tightness and nocturnal symptoms, change in the pre-bronchodilator FEV1 during the treatment and hematological improvement. The secondary end points were change in the post-bronchodilator FEV1 (change from baseline during the treatment) and C - reactive protein (CRP) concentration.
All adverse events either reported or observed by patients were recorded in CDSCO forms. Patients were allowed to voluntarily withdraw from the study but efforts were made to ascertain the reason for dropout. Subjects were asked to maintain a daily diary regarding use of all medications and were asked to bring back the curcumin bottles to monitor medication compliance.
Statistical Analysis
The data was analysed using SPSS 17.0 software. The two groups were compared with each other for changes in various parameters either by one-way ANOVA (comparing reduction in severity of asthma symptoms) or paired t-test (comparing improvement in FEV1 values and improvement in hematological parameters). The level of significance was fixed at p<0.05.
Results
Seventy-seven patients, meeting the inclusion criteria were recruited in the study. Out of 77 enrolled patients, 17 patients were lost to follow-up (10 patients in Group A and 07 patients in Group B) and the remaining 60 patient’s data was analysed.
Group A: Receiving standard therapy for asthma (n=30)
Group B: Receiving standard therapy for asthma + Curcumin (n=30)
Demographic data: The mean age of the study population in years, the distribution of female and male patients, the mean height in cms and mean weight in kgs was comparable in both group A and group B patients [Table/Fig-1].
Clinical symptoms: The severities of clinical symptoms were analysed individually for both Group A and Group B, and the mean baseline (0 visit), 10th day (1st visit), 20th day (2nd visit) and 30th day (3rd visit) values were calculated. The reductions in symptoms of dyspnea, wheezing, cough, chest tightness, nocturnal symptoms and the total symptom score were compared in both the groups by one way ANOVA. All the values were found to be insignificant [Table/Fig-2].
Pulmonary Function Tests: FEV1 values were analysed individually for both Group A and Group B, on day 0, 10th, 20th and 30th day. Also, the improvements in FEV1 values in both the groups were compared to evaluate the efficacy of curcumin as an ‘add-on’ therapy. Analyzing improvement in FEV1 values of both the groups by using paired‘t’ test it was revealed that Group B patients showed significant improvement in FEV1 values as compared to Group A patients [Table/Fig-3].
Hematological values: Hematological parameters were analysed individually for both Group A and Group B, and the mean baseline (0 visit) and 30th day (3rd visit) values were calculated. On comparing the improvement of hematological values in both the groups by paired t-test it was noted that decrease in total leukocyte count was more in Group B patients as compared to Group A patients, p < 0.05 (significant); increase in neutrophils was more in Group A patients as compared to Group B patients; decrease in lymphocytes was more in Group A patients as compared to Group B patients;decrease in eosinophils and decrease in ESR was more in Group B as compared to Group A, p< 0.05 (significant) [Table/Fig-4].
Adverse events: Although the Group B patients recorded less number of adverse events in comparison with the Group A patients, the comparison is statistically insignificant. While headache and insomnia was recorded in both the study groups; weight gain was observed only in Group B and decrease in appetite was reported with Group A only. There were no clinically significant reported or observed adverse events [Table/Fig-5].
Discussion
Bronchial asthma, a chronic bronchial inflammatory disorder, is characterized by bronchoconstriction, increased mucus production and airway hyper-responsiveness. The increased inflammatory infiltrate, tenacious plugs of exudates and mucus and enlargement of bronchial smooth muscle particularly in medium sized bronchi leads to the resultant symptomatology of wheezing, coughing and dyspnea. Bronchodilators and inhaled/systemic corticosteroids are commonly used as the first-line treatment for symptomatic management but their use is limited due to long-term adverse effects. Prophylactic therapy is essential in asthma but they do not prevent recurrent episodes.
Despite major advances in treating asthma, until now disease-modifying efficacy has not been demonstrated for any of the existing drugs, therefore there is an essential need to develop new drugs that might be of additional benefit in clinical settings. Since herbal medicines offer a positive beneficial effect in most chronic diseases, we aimed to investigate this aspect in our study. Over the years, there has been increasing evidence that curcumin, a phytochemical present in Curcuma longa (Turmeric or haldi), has a wide spectrum of therapeutic properties including modulation of inflammation and oxidative stress. Various studies have clearly established it’s anti-inflammatory effect both in vitro and in vivo by inhibiting iNOS production and scavenging the free radicals, inhibiting the activation of NF-kappaB and activating protein 1 (AP 1) and suppressing the production of proinflammatory cytokines [2]. Studies have also demonstrated that curcumin decreases the level of iNOS-induced by IFN-γ in lung tissue and expression of cytokines such as IL-2,IL-5 and GM-GSF by acting as a histone deacetylases (HDAC) activator and inhibits histamine release from mast cells. It has been proved that curcumin can also restore HDAC activity, thereby restoring corticosteroid function [12]. Previous data from various studies have demonstrated the efficacy of curcumin in animal models of asthma, but there are very few human trials which explored the efficacy of oral curcumin in asthma. Hence, we decided to undertake this study.
Kobayashi T et al., showed that curcumin when added to Dermatophagoides farineae (Der-f)-stimulated lymphocyte cell cultures from allergic asthmatics inhibited Der-f-induced lymphocyte proliferation and production of IL-2, IL-4, IL-5 and GM-CSF thereby proving that curcumin blocks the allergen- triggered release of inflammatory chemicals in white blood cells taken from asthma patients. It also demonstrated that curcumin may have potential effects on controlling allergic diseases through inhibiting the production of cytokines, eosinophil function and IgE synthesis [13].
South et al., investigated the effects of dietary curcumin (1, 20 or 40 mg/kg) for five wks on antibody (IgG) production, delayed-type hypersensitivity and natural killer cell activity in rats. The highest doses of curcumin, significantly enhanced IgG levels. Neither delayed-type hypersensitivity nor natural killer cell activity was different from control values at any dietary concentration of curcumin [14].
Another significant study by Ram A et al., studied the effect of curcumin on airway hyperresponsiveness in sensitized guinea pigs and demonstrated by a constant volume body plethysmograph that curcumin significantly inhibited ovalbumin-induced airway constriction and airway hyperreactivity in guinea pigs [15].
It was shown by Kohli K et al., that curcumin in a dose of 200 mg/kg body weight helps to prevent allergic airway inflammation by inhibiting the actions of an inflammatory protein called NF-κB [16].
Kurup et al., used a murine model of latex allergy to investigate the role of curcumin as an immunomodulator. BALB/c mice were exposed to latex allergens and developed latex allergy with a T helper 2 lymphocycets (Th2) type immune response. These animals were treated with curcumin and the immunologic and inflammatory responses were evaluated. Animals exposed to latex showed enhanced serum IgE, latex-specific IgGl, IL-4, IL-5, IL-13, and eosinophils and inflammation in the lungs. Intragastric treatment of latex-sensitized mice with curcumin demonstrated a diminished Th2 response with a concurrent reduction in lung inflammation. Eosinophilia in curcumin-treated mice was markedly reduced, co-stimulatory molecule expression (CD80 and CD86) on antigen-presenting cells was decreased and expression of MMP-9 and OAT genes was also attenuated. These results suggest that curcumin has potential therapeutic value for arresting and reversing tissue, specifically lung inflammation in mice due to a controlled allergic reaction with exposure to latex [17] .
Moon et al., investigated the anti-inflammatory effect of curcumin in a different model of ovalbumin induced murine asthma and found that pre-treatment with curcumin caused low levels of ovalbumin induced nitric oxide, IL-4, IL-5, IFN-γ and IgE antibodies [18].
In another study by Aggarwal BB et al., curcumin significantly inhibited the activity of NF-κB, thus inhibiting the airway inflammation and cell infiltration in asthma. It also proved that curcumin decreases the expression and release of eotaxin, MCP-1 and MCP-3 from IL-1-stimulated human airway smooth muscle cells [19].
Oh SW et al., proved that curcumin attenuates the allergic airway inflammation and hyper-responsiveness of asthma in mice by inhibiting NF-κB activation [20].
Karaman M et al., demonstrated that curcumin was as effective as the prescription steroid dexamethasone and had equal ability to reverse ovalbumin induced histopathological airway changes due to inflammation [21].
Xin Zeng et al., demonstrated that the proliferation of airway smooth muscle cells is inhibited by curcumin in vitro and in vivo by upregulating the expression of caveolin-1 and blocking the activation of extracellular signal-regulated kinase (ERK) pathway [22].
Antiinflammatory activity of curcumin was demonstrated by various authors. Kang BY et al., demonstrated that curcumin significantly inhibits production of IL-12, reduces the induction of IFN-γ, IL-4 in CD4+ T-cells by macrophages, leading to the inhibition of Th1 cytokine profile [23]. Chainani Wu N showed that curcumin inhibits several agents involved in inflammation including phospholipase, lipoxygenase, cyclooxygenase-2, leukotrienes, thromboxane, prostaglandins, nitric oxide, collagenase, elastase, hyaluronidase, monocyte chemoattractant protein-1, interferon-inducible protein, tumour necrosis factor alpha and interleukin-12 [24]. Hong et al., confirmed that curcumin is a dual inhibitor of arachidonic acid metabolism, inhibiting both the enzymes 5-lipoxygenase and cyclooxygenase [24]. Similarly a study by Jagetia GC et al., proved that curcumin is a potent immunomodulatory agent that can modulate the activation of T cells, B cells, macrophages, neutrophils, natural killer cells and dendritic cells and can also downregulate the expression of various proinflammatory cytokines including TNF-α, IL-1, IL-2, IL-6, IL-8, IL-12, and chemokines [25]. Another important study by Biswas S et al., illustrates that curcumin can down-regulate expression of pro-inflammatory mediators, matrix metalloproteinases, adhesion molecules and growth factor receptor genes and they up-regulate HDAC2 in the lungs. It also showed that curcumin can directly scavenge free radicals such as superoxide anion and nitric oxide and modulate important signaling pathways mediated via NF-B and mitogen-activated protein kinase pathways [26].
There are numerous clinical studies of curcumin in patients of rheumatoid arthritis, chronic anterior uveitis, inflammatory orbital pseudotumor, cancers of oral cavity, breast, skin etc and various other diseases [16]. But there are few published studies which have evaluated the clinical effect of oral curcumin on asthmatics patients. In reference to all the above studies we hypothesized that curcumin being a strong anti-inflammatory agent could prove efficacious as add-on therapy in mild to moderate asthma patients. Therefore, the present study was conducted to compare the effects of 4 weeks of treatment with curcumin capsules as add-on therapy (Group B) on lung function, severity of symptoms, hematological parameters and on treatment related adverse outcomes with that of 4 weeks of standard treatment for patients having mild-to-moderate asthma (Group A).
In our study, the mean age of the population was approximately thirty two years with almost similar gender distribution in both the groups [Table/Fig-1] . Thus the two groups were demographically comparable to each other. This it is in accordance with previous studies stating that occurrence of bronchial asthma is more before the age of forty with equal sex ratio in the adults [27].
When both the groups were analysed individually for reductions in severity of asthma symptoms, it was observed that there was significant reduction (p< 0.05) in the mean scores for cough, dyspnoea, wheezing, chest tightness, nocturnal symptoms and total asthma symptom score in both the groups between baseline and 30th day i.e. 3rd visit. However, when reductions in severity of asthma symptoms in both the groups were compared, the results were found to be insignificant (p>0.05); thus it is unlikely that curcumin has an effect on reduction in severity of asthma symptoms [Table/Fig-2]. Our results differ with the uncontrolled trial conducted in India, where 60% of asthma patients administered plain or ghee-fried turmeric powder showed a relief in their symptoms [28]; but since they have used turmeric, it cannot be ascertained whether reduction in severity of asthma symptoms was due to curcumin or due to some other component of turmeric. In our study curcumin does not have any effect on asthma symptoms may be because patients were recruited from the community with mild to moderate asthma and the symptomatic impairment may have been severe enough not to get cured with either the studied dose or duration of curcumin administered.
When both the groups were analysed individually for improvement in FEV1 values, it was observed that there was a significant reduction (p < 0.05) in the mean improvement of FEV1 values, between baseline (0 visits) and 30th day (3rd visit) in both the groups. Further, when improvements in FEV1 values in both the groups were compared, the results revealed that Group B patients showed significant (p < 0.05) improvement in Pre-FEV1, Post FEV1 and % reversibility values as compared to Group A patients groups [Table/Fig-3,Table/Fig-6]. Thus, it is suggested that curcumin causes improvement in FEV1 values. Our results are in consistence with the study of Ng TP et al., indicating an improvement in FEV1 values and FEV1/FVC values indicating a significant decrease in airway constriction and inflammation [29].
When both the groups were analysed individually for reduction in hematological parameters (TLC, DLC, ESR), it was observed that there was significant reduction (p < 0.05) in the mean scores for hematological parameters between baseline (0 visit) and 30th day (3rd visit) in both the groups. Further, when improvement of hematological parameters in both the groups were compared, the results revealed that Group B patients showed significant improvement (p<0.05) in the hematological parameters as compared to Group A patients [Table/Fig-4]. These results are in agreement with the studies of Kurup et al., [17] Jagetia GC et al., [25] and Vachharajini V et al.,[30] all of which showed improvement in haematological profile with curcumin. This modulation of hematological parameters probably emphasizes on the anti-inflammatory properties of curcumin.
No safety concerns emerged over the use of curcumin during the study; neither of the group showed any significant drug-related adverse events [Table/Fig-5]. Hepatic and renal functioning was assessed both at the beginning and end of the study. All the known adverse effects of curcumin were monitored vigorously on regular basis, making sure that no ADR went unnoticed. This is supported by the review of the previous literature stating that curcumin does not cause significant short-term toxicity at doses up to 8 g/day [7].
Overall, our study demonstrated efficacious FEV1 control and significant improvement in the hematological parameters at the end of the treatment compared to their baseline values in group B patients. The significance can be attributed to the use of curcumin capsules as an add-on therapy in bronchial asthma patients. Thus, our study proved the beneficial role of curcumin as an add-on therapy in asthma.
There is no effect of curcumin add-on therapy on improvement of asthma symptoms. This may be because the number of the study subjects were only 60, who completed the study, which may be insufficient numbers to provide a statistically significant result in the patient centered outcome measures (like asthma symptoms). Besides the dose and duration of curcumin administered may not be sufficient enough to produce clinically beneficial effect. Moreover the severity of clinical symptoms were assessed by an individual (as absent, mild, moderate and severe with scores of 0, 1, 2 and 3) thus were not much reliable. A further study with large subjects and modified dose is now required to investigate the effects of curcumin on symptomatic control. In addition, the study only explored the use of curcumin as an add-on therapy, and no information can be inferred on the use of this agent as monotherapy or as a steroidsparing agent. These areas need further exploration.
Conclusion
This study evaluated the clinical efficacy and safety of curcumin capsules as an add on therapy in patients of mild to moderate asthma and proved therapeutic improvement in FEV1 values along with improvement in concerned hematological parameters. This corroborates the fact that there is a definite improvement in lung function due to the anti-inflammatory effect of curcumin though there is no visible clinical efficacy. Therefore a further clinical evaluation is needed with more number of subjects, a higher tolerated dose and for a longer duration. Absence of any clinically significant adverse events indicates dependable safety profile of curcumin. Therefore, it is concluded that curcumin is effective and safe as an add-on therapy for the treatment of bronchial asthma.
[1]. Bronchial asthmahttp://www.who.int/mediacentre/factsheets/fs206/en/ accessed on 2014 Feb 4 [Google Scholar]
[2]. PJ Barnes, Cytokine modulators as novel therapies for asthma.Annu Rev Pharmacol Toxicol. 2002 42:81-98. [Google Scholar]
[3]. PJ Barnes, Pulmonary pharmacotogy. In: Brunton LL editor. Goodman & Gilman’s The pharmacological basis of therapeutics.J Oral Med 2011 12th EditionNew YorkMcGraw-Hill:1031-65. [Google Scholar]
[4]. W Mitzner, RO Cooley, NH Olsen, JJ Hefferren, Bronchial thermoplasty in asthma.Allergology International. 2006 55:225-34. [Google Scholar]
[5]. PD Blanc, L Trupin, G Earnest, PP Katz, EH Yelin, MD Eisner, Alternative therapies among adults with a reported diagnosis of asthma or rhinosinusitis: a data from a population based survey.Chest. 2001 120:1461-67. [Google Scholar]
[6]. H Itokawa, Q Shi, T Akiyama, SL Morris-Natschke, KH Lee, Recent advances in the investigation of Curcuminoids.Chin Med. 2008 :3-11. [Google Scholar]
[7]. JS Jurenka, Anti-inflammatory properties of Curcumin, a major constituent of Curcuma longa: A review of preclinical and clinical research.Alternative medicine review. 2009 l4:141-53. [Google Scholar]
[8]. C Jobin, CA Bradham, MP Russo, B Juma, AS Narula, DA Brenner, Curcumin blocks cytokine-mediated NF-kappaB activation and pro-inflammatory gene expression by inhibiting inhibitory factor I-kappaB kinase activity.J Immunol. 1999 163:3474-83. [Google Scholar]
[9]. Y Cheng, J Ping, LM Xu, Effects of Curcumin on peroxisome proliferator- activated receptor gamma expression and nuclear translocation/redis- tribution in culture activated rat hepatic stellate cells.Chinese Med J. 2007 120:794-801. [Google Scholar]
[10]. HP Ammon, MA Wahl, Pharmacology of Curcuma longa.Planta Med. 1991 57:1-7. [Google Scholar]
[11]. N Chainani-Wu, Safety and anti-inflammatory activity of Curcumin: A component of turmeric (Curcuma longa).J Altern Complement Med. 2003 9:161-68. [Google Scholar]
[12]. KK Meja, S Rajendrasozhan, D Adenuga, SK Biswas, IK Sundar, G Spooner, Curcumin restores corticosteroid function in monocytes exposed to oxidants by maintaining HDAC2.Am J Respir cell Mol Biol. 2008 39:312-23. [Google Scholar]
[13]. T Kobayashi, S Hashimoto, T Horie, Curcumin inhibition of Dermatophagoides farinea-induced interleukin-5 (IL-5 ) and granulocyte macrophage- colony stimulating factor (GM-CSF) production by lymphocytes from bronchial asthmatics.Biochem Pharmacol. 1997 54:819-24. [Google Scholar]
[14]. EH South, IH Exon, K Hendrix, Dietary Curcumin enhances antibody response in rats.Immunopharmacol Immunotoxicol. 1997 19:105-19. [Google Scholar]
[15]. A Ram, M Das, B Ghosh, Curcumin attenuates allergen-induced airway hyperresponsiveness in sensitized guinea pigs.Biol Pharm Bull. 2003 26:1021-24. [Google Scholar]
[16]. Kohli K, Ali J, Ansari M J, Raheman Z, Curcumin: A natural antiinflammatory agent.Indian J Pharmacol. 2005 37:141-47. [Google Scholar]
[17]. VP Kurup, CS Barrios, R Raju, BD Johnson, MB Levy, JN Fink, Immune response modulation by Curcumin in a latex allergy model.Clin Mol Allergt. 2007 5:1 [Google Scholar]
[18]. DO Moon, MO Kim, HJ Lee, YH Choi, YM Park, MS Heo, Curcumin attenuates ovalbumin-induced airway inflammation by regulating nitric oxide.Biochem Biophys Res Commun. 2008 375:275-79. [Google Scholar]
[19]. BB Aggarwal, KB Harikumar, Potential therapeutic effects of Curcumin, the anti-inflammatory agent, against neurodegenerative, cardiovascular, pulmonary, metabolic, autoimmune and neoplastic diseases.Int J Biochem Cell Biol. 2009 41:40-59. [Google Scholar]
[20]. SW Oh, JY Cha, JE Jung, BC Chang, HJ Kwon, BR Lee, Curcumin attenuates allergic airway inflammation and hyper-responsiveness in mice through NF-κB inhibition.J Ethnopharmacol. 2011 136:414-21. [Google Scholar]
[21]. M Karaman, Z Arikan Ayyildiz, F Firinci, M Kiray, A Bagriyanik, O Yilmaz, Effects of Curcumin on lung histopathology and fungal burden in a mouse model of chronic asthma and oropharyngeal candidiasis.Archives of medical research. 2011 42:79-87. [Google Scholar]
[22]. Zeng Xin, Cheng Ying, Qu Yuejun, Xu Jide, Han Zhiyuan , Zhang Tingting , Curcumin inhibits the proliferation of airway smooth muscle cells in vitro and in vivo. Int J Mol Med. 2013 32:629-36. [Google Scholar]
[23]. Kang BY, Song YJ, Kim KM, Choe YK, Hwang Y, Kim TS, Curcumin inhibits Th1 cytokine profile in CD4+T cells by suppressing interleukin-12 production in macrophages.Br J Pharmacol. 1999 128:380-84. [Google Scholar]
[24]. J Hong, M Bose, J Ju, JH Ryu, X Chen, S Sang, Modulation of arachidonic acid metabolism by Curcumin and related β-diketone derivatives: Effects on cytosolic phospholipase A2, cyclooxygenases and 5 lipoxygenase.Carcinogenesis. 2004 25:1671-79. [Google Scholar]
[25]. GC Jagetia, BB Aggarwal, Spicing up of the immune system by curcumin.J Clin Immunol. 2007 27:19-35. [Google Scholar]
[26]. S Biswas, I Rahman, Modulation of steroid activity in chronic inflammation: a novel anti-inflammatory role for Curcumin.Mol Nutr Food Res.. 2008 52:987-94. [Google Scholar]
[27]. M Schatz, S Clark, CA Camargo Jr, Sex Differences in the presentation and course of asthma hospitalizations.Chest. 2006 129:50-5. [Google Scholar]
[28]. SK Vemula, PR Turapati, RSR Ponugoti, P Garrepally, Asthma: Alternative management approaches. Asian J Pharm Clin Res. 2011 4:1-8. [Google Scholar]
[29]. TP Ng, M Niti, KB Yap, WC Tan, Curcumins-Rich Curry Diet and Pulmonary Function in Asian Older Adults.PLoS ONE. 2012 7(12):e51753 [Google Scholar]
[30]. V Vachharajani, SW Wang, N Mishra, M El-Gazzar, B Yoza, C McCall, Curcumin modulates leukocyte and platelet adhesion in murine sepsis.Microcirculation. 2010 17:407-16. [Google Scholar]