Role of Absolute Reticulocyte Count in Evaluation of Pancytopenia-A Hospital Based Study
Poorana Priya P1, Subhashree A.R.2
1 Postgraduate, Department of Pathology, Sree Balaji Medical College & Hospital, Bharath University, Chrompet, Chennai, India.
2 Professor, Department of Pathology, Sree Balaji Medical College & Hospital, Bharath University, Chrompet, Chennai, India.
NAME, ADDRESS, E-MAIL ID OF THE CORRESPONDING AUTHOR: Dr. Poorana Priya. P, No:7, Sree Balaji Medical College & Hospital, C.L.C Works Road, New Colony, Chrompet, Chennai-600044, India. Phone : 8148486849, E-mail : poorna.priya86@gmail.com
Background: Pancytopenia is a common hematological entity encountered in our laboratory practice. Evaluating the causes of pancytopenia is essential for the diagnostic as well as therapeutic management of the patients. Absolute Reticulocyte count (ARC) plays a pivotal role in identifying the cause of pancytopenia in most of the cases but it has grossly been overlooked. Hence, we attempted to identify the significance of ARC as a deciding parameter in evaluating the causes of pancytopenia.
Materials and Methods: The study was conducted in a tertiary health care hospital, Chennai, India. A cross-sectional descriptive study was conducted over a period of two years (2011-2013). Patients who satisfied the criteria for pancytopenia were evaluated with clinical details. Pancytopenia work-up including Peripheral blood picture, Complete blood counts, Reticulocyte count, Serum Ferritin, B12, Folate and Bone marrow aspirate was carried out. ARC was calculated and an algorithm to approach the cases of pancytopenia was derived considering ARC as the key factor.
Results: A total of 429 cases of pancytopenia were evaluated and based on our algorithm results were tabulated. ARC was found to be <25x10^9/L for cases of Aplastic anaemia; 25-50x10^9/L for Nutritional anaemia; and, >100x10^9/L in Marrow infiltrative disorders and in cases of sepsis and malaria.
Conclusion: We found that ARC plays an important role in differentiating various causes of pancytopenia and hence should be routinely included in pancytopenia work up in order to avoid unnecessary bone marrow aspirations in pancytopenic patients.
Aplastic anaemia, Absolute reticulocyte count, Bone marrow aspiration, Mixed nutritional anaemias, Pancytopenia, Reticulocyte percentage
Introduction
Bone marrow aspiration is considered of primary importance in evaluating the cases of Pancytopenia [1–3]. Absolute reticulocyte count (ARC) is a calculated index derived from the product of two parameters namely Reticulocyte count percentage and RBC count [4,5]. It is a marker of red cell production and helps in distinguishing hypo and hyper proliferative anaemias [4,5]. The normal reticulocyte count is 0.5-2.5% and the normal absolute reticulocyte count is 50-100X109/L [4–6]. ARC may be very helpful in initial evaluation of pancytopenia but its utility value is often underestimated. Hence in our study we calculated the ARC of patients with pancytopenia, formed an algorithm based on these counts and classified them.
Materials and Methods
The study was approved by our Institutional ethical committee. The study was conducted for a period of two years (2011-2013) in the hematology department of a tertiary care hospital. A total of 429 patients attending to the In-patient Department of General Medicine of the same hospital, who satisfied the criteria for pancytopenia with hemoglobin <9g/dl, WBC<4000/μl, Platelets <1,00,000/μl [4,5] were included in our study. Sufficient clinical details were obtained from these patients. Two ml of EDTA sample and 3ml of whole blood sample were collected. Complete hemogram, peripheral blood film and reticulocyte count were performed. Serum B12, Folate and Ferritin assays were done for all the cases and QBC was done in selected cases to R/O Malaria. Bone marrow study was performed for all cases. Based on the final diagnosis an algorithm was derived considering ARC as an important evaluating parameter to approach the cases of pancytopenia.
Statistical Analysis
Done using SPSS Version 15.0.Mean and Standard deviation values were calculated for the hematological parameters in all cases.
Results
A total of 429 cases of pancy to penia were tabulated 75.29% of our cases were males. [Table/Fig-1] shows the baseline characteristics of the cases. Megaloblastic anaemia was the commonest cause of pancytopenia (36.36%). RBC count and Hb was found to be the lowest with Aplastic anaemia. MCV was higher in Megaloblastic anaemia RDW (Red cell Distribution width) was high in Megaloblastic anaemia compared to Mixed Nutritional anaemias.
Baseline characteristics of pancytopenic cases in our study
| S. No | Causes | No of cases | RBC | HB(g/dl) | MCV(fl) | RDW(%) |
|---|
| Mean | SD | Mean | SD | Mean | SD | Mean | SD |
|---|
| 1. | Aplastic anemia | 72 | 2.215 | 0.2019 | 4.667 | 1.1868 | 86.264 | 5.0435 | 13.854 | 1.0747 |
| 2 | Megaloblastic Anemia | 156 | 3.105 | 0.3404 | 6.372 | 1.2609 | 119.994 | 5.5001 | 17.884 | 1.9290 |
| 3 | Mixed anemia | 93 | 3.109 | 0.1926 | 5.849 | 1.1224 | 87.935 | 7.5308 | 15.039 | 1.3876 |
| 4 | Myelodysplastic Syndrome | 2 | 3.350 | 0.2121 | 7.500 | 0.7071 | 84.500 | 2.1213 | 13.500 | 0.7071 |
| 5 | Leukemia | 13 | 3.638 | 0.2725 | 6.846 | 1.1435 | 87.000 | 2.9155 | 12.438 | 0.5824 |
| 6 | Lymphoid Neoplasms | 12 | 3.808 | 0.2843 | 7.167 | 0.9374 | 87.667 | 2.6054 | 11.958 | 0.8107 |
| 7. | Metastasis | 10 | 4.090 | 0.3900 | 6.000 | 0.8165 | 86.100 | 3.9285 | 10.400 | 1.0750 |
| 8. | Malaria | 20 | 3.755 | 0.2625 | 6.950 | 0.8870 | 87.700 | 2.3864 | 11.695 | 0.9047 |
| 9. | Sepsis | 51 | 3.859 | 0.3430 | 6.882 | 1.0516 | 86.196 | 3.1114 | 10.353 | 1.0163 |
| Total | 429 | 3.136 | 0.5883 | 6.093 | 1.3674 | 94.664 | 21.133 | 14.881 | 3.0737 |
[Table/Fig-2] shows, Reticulocyte percentage and ARC of the patients. ARC was very much decreased in Aplastic anaemia with mean value of (22.19x109/L). Nutritional anaemias and Myelodysplastic syndrome showed moderate decrease in ARC values yet, the Mean Reticulocyte percentage was found to be the same in all the above mentioned cases (0.1%). All the Marrow infiltrative disorders and systemic infections presented with very high ARC.
Descriptive statistics of reticulocyte percentage & ARC
| S.No | Causes | Reticulocyte count (%) | Absolute reticulocyte Count (x109/L |
|---|
| Mean | SD | Mean | SD |
|---|
| 1 | Aplastic Anemia | 0.100 | 0.000 | 22.194 | 2.0045 |
| 2 | Megaloblastic Anemia | 0.100 | 0.000 | 30.849 | 4.0423 |
| 3 | Mixed Anemia | 0.100 | 0.000 | 31.086 | 1.9261 |
| 4 | Myelodysplastic Syndrome | 0.100 | 0.000 | 33.500 | 2.1213 |
| 5 | Leukemia | 3.615 | 0.5064 | 131.308 | 19.6103 |
| 6 | Lymphoid Neoplasms | 4.000 | 0.0000 | 152.333 | 11.3725 |
| 7 | Metastasis | 4.600 | 0.5164 | 187.100 | 19.0056 |
| 8 | Sepsis | 5.510 | 0.6441 | 215.863 | 27.6058 |
| 9 | Malaria | 6.300 | 1.0809 | 232.800 | 43.8149 |
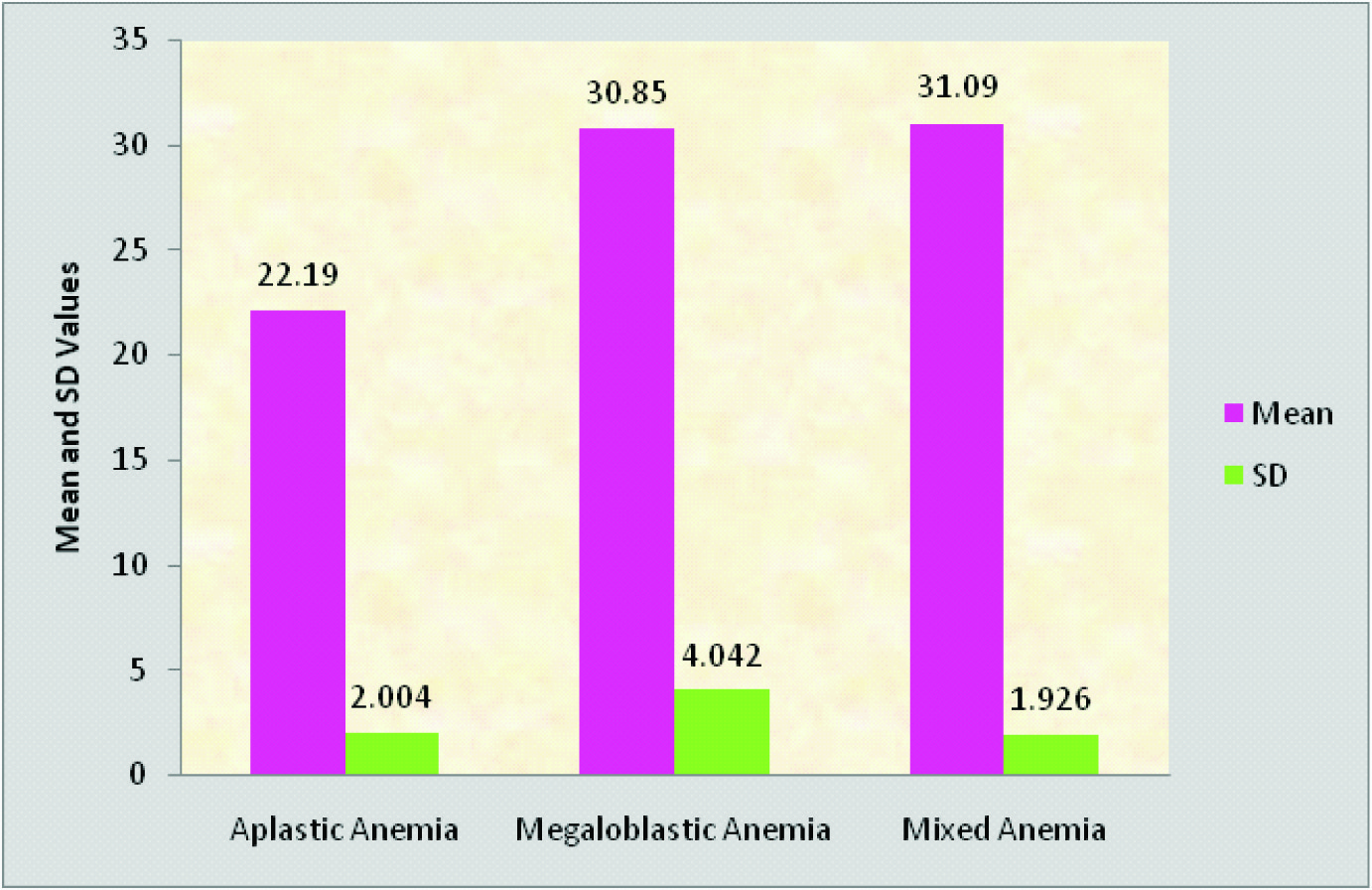
[Table/Fig-3] highlights the comparison of ARC values in all the three hypo proliferative anaemias in our study.
Comparison between aplastic anemia, megaloblastic anemia and mixed anemia in arc values
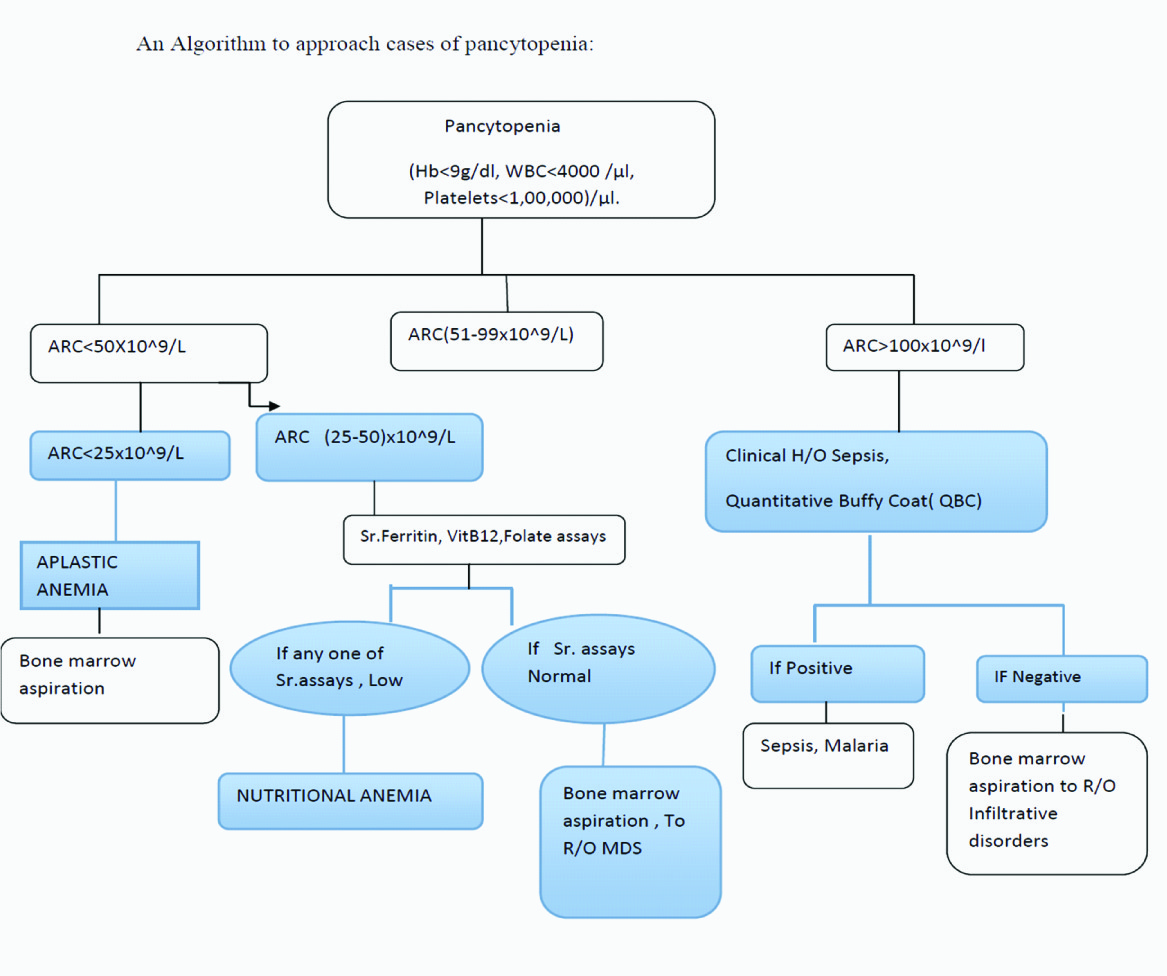
[Table/Fig-4] shows the algorithm to approach the cases of Pancytopenia using ARC as a key parameter.
An Algorithm to approach cases of pancytopenia
Discussion
Our study showed a male preponderance similar to the studies carried out by Khunger et al., [7]. Megaloblastic anaemia was the commonest cause of Pancytopenia [Table/Fig-1] which is consistent with other studies [7,8]. RBC count was found to be very low with Aplastic anaemia compared to other causes of pancytopenia [Table/Fig-1]. This may be the reason why ARC is very low [Table/Fig-2] with Aplastic anaemia [9,10] compared to other hypo proliferative disorders such as Megaloblastic anaemia and Mixed Nutritional anaemias. It is essential to mention here that the Reticulocyte counts were more or less equal (Mean = 0.1%) in all the three conditions.
A very high MCV of >110f l is seen in all cases of Megaloblastic anaemias [11,12] which could be used as an adjunct in the diagnosis.
RDW was found to be higher in nutritional anemias which could be explained by marked anisocytosis as expected in these conditions [11–13].
In all the cases of pancytopenia, Reticulocyte counts and ARC should be done on day one along with CBC in order to avoid therapy related changes in reticulocyte count, particularly with Nutritional anaemias.
[Table/Fig-3] shows the comparison of ARC values in cases of Aplastic anaemia, Megaloblastic anaemia and Mixed nutritional deficiency anaemia and found to be the lowest with Aplastic anaemia.
[Table/Fig-4] shows an approach to the cases of pancytopenia using ARC.
ARC was stratified in to < 50x 109/L(low), 51-99x109/L (Normal) and >100 x109/L(High) [4,5]. All cases of Aplastic anaemia had an ARC of <25x109/L, which can be taken as an indication for bone marrow aspiration. ARC of 25-50x109/L has to be evaluated with Serum B12, Folate and Ferritin assays and if these assays are found to be low it rules out the need for a bone marrow aspiration. None of our cases of pancytopenia had a normal ARC of 51-99x109/L. All cases of pancytopenia with high ARC should be evaluated with a Bone marrow aspiration unless there is a history of Sepsis or Malaria. This algorithm stresses the importance of calculating absolute reticulocyte count for all cases of pancytopenia.
Conclusion
Our study highlighted that systematic approach in cases of pancytopenia is essential to avoid unnecessary invasive procedures like bone marrow aspiration. We found ARC to be superior than routine reticulocyte count in differentiating aplastic anaemia from other hypo proliferative anemias and hence, ARC could be incorporated routinely in the diagnostic protocol of all pancytopenic patients.
[1]. Prchal JT, Production of Erythrocytes. In: Lichtman MA, Kipps TJ, Seligsohn U, Kaushansky K, Prchal JT, edsWilliams Hematology 2010 8th edNew YorkMcGraw-HillChapter 31 [Google Scholar]
[2]. Knodke K, Marwah S, Buxi G, Vadav RB, Chaturvedi NK, Bone marrow examination in cases of pancytopeniaJ Academy Clin Med 2001 2:55-9. [Google Scholar]
[3]. Jha A, Sayami G, Adhikari RC, Panta AD, Jha R, Bonemarrow examination in cases of pancytopeniaJ Nepal Med Assoc 2008 47:12-7. [Google Scholar]
[4]. Piva E, Brugnara C, Chiandetti L, Plebani M, Automated reticulocyte counting: state of the art and clinical applications in the evaluation of erythropoiesisClin Chem Lab Med 2010 48(10):1369-80. [Google Scholar]
[5]. Kumar R, Kalra SP, Kumar H, Anand AC, Madan M, Pancytopenia-A six year studyJ Assoc Physicians India 2001 49:1079-81. [Google Scholar]
[6]. Ryan DH, Examination of Blood Cells. In: Lichtman MA, Kipps TJ, Seligsohn U, Kaushansky K, Prchal JT, edsWilliams Hematology 2010 8th edNew YorkMcGraw-HillJanuary 15, 2012:Chapter 2. http://www.access medicine.com/content.aspx?aID=6106433. Accessed [Google Scholar]
[7]. Khunger JM, Arculselvi S, Sharma U, Ranga S, Talib VH, Pancytopenia-A Clinico-hematological study of 200 casesIndian J Pathol Microbiol 2002 45:375-79. [Google Scholar]
[8]. Gayathri BN, Rao KS, Pancytopenia: A clinicohematological studyJ Lab Physicians 2011 3:15-20. [Google Scholar]
[9]. Guinan EC, Shimamura A, Acquired and inherited aplastic anaemia syndromes In: Greer JP, Foerster J, Lukens JN, Rodgers GM, Paraskevas F, Glader B, editorsWintrobe’s Clinical Hematology 2004 11th edPhiladelphiaLippincott Williams and Wilkins:1397-419. [Google Scholar]
[10]. Buttarello M, Bulian P, Farina G, Petris MG, Temporin V, Toffolo L, Five fully automated methods for performing immature reticulocyte fraction: comparison in diagnosis of bone marrow aplasiaAmerican Journal of Clinical Pathology 2002 117:871-79. [Google Scholar]
[11]. Bessman JD, Gilmer PR, Gardner FH, Improved classification of anaemias by MCV and RDWAm J Clin Pathol 1983 80:322-26. [Google Scholar]
[12]. Unnikrishnan V, Dutta TK, Badhe BA, Bobby Z, Panigrahi AK, Clinico-aetiologic profile of macrocytic anaemias with special reference to megaloblastic anaemiaIndian Journal of Hematology and Blood Transfusion 2008 24(4):155-65. [Google Scholar]
[13]. Subhashree AR, Parameaswari PJ, Shanthi B, Revathy C, Parijatham BO, The Reference Intervals for the Haematological Parameters in Healthy Adult Population of ChennaiSouthern India. J Clin Diagn Res 2012 6(10):1675-80. [Google Scholar]