Ossified Ligamentum Longitudinale Anterius in Adult Human Dry Vertebrae
Kalyan Chakravarthi Kosuri1, Nelluri Venumadhav2, Siddaraju KS3
1 Assistant Professor, Department of Anatomy, Mayo Institute of Medical Sciences, Faizabad Road, Gadia, Barabanki, Uttar Pradesh, India.
2 Senior Grade Lecture, Department of Anatomy, Melaka Manipal Medical College (MMMC), Manipal University, Manipal and Karnataka, India.
3 Lecturer, Department of Anatomy, KMCT Medical College, Manassery, Calicut, Kerala, India.
NAME, ADDRESS, E-MAIL ID OF THE CORRESPONDING AUTHOR: Mr. Kalyan Chakravarthi Kosuri, Assistant Professor, Department of Anatomy, Mayo Institute of Medical Sciences, Faizabad Road, Gadia, Barabanki, Uttar Pradesh, India. Phone : 08142214159, E-mail : kalyankosuric@gmail.com
Background: The ligamentum longitudinale anterius is a broad and strong band of fibrous tissue that runs along the anterior surfaces of the bodies of the vertebrae.
Aim: The study was undertaken to evaluate the incidence of ossified ligamentum longitudinale anterius in adult dry human vertebra.
Materials and Methods: This study was carried out on 95 sets of dry human vertebral columns irrespective of age and sex at Mayo Institute of Medical Sciences- Barabanki,-UP, Melaka Manipal Medical College-Manipal University and Department of Anatomy, KMCT Medical College, Manassery- Calicut, India. All the sets of vertebral columns were macroscopically inspected for the ossified ligamentum longitudinale anterius.
Results: It was observed that out of 95 sets of vertebral columns, 27 (28.42%) vertebral columns showed ossification. Out of 27 vertebral columns, 17 (17.89%) vertebral columns showed segmental type of ossification, 2 (2.11%) vertebral columns showed continuous type of ossification and 8 (8.42%) vertebral columns showed mixed type of ossification at different vertebral level.
Conclusion: Such type of ossification will affect the biomechanics of the spine and may result in stiff neck, low back pain, dysphagia, odynophagia, compression of the brachial plexus, aphonia, immobility or mucosal thickening of larynx. Hence, knowledge of such abnormalities should be kept in mind to minimise serious complications in any surgical intervention or investigative procedures in the region.
Dysphagia, Kyphosis, Odynophagia
Introduction
The major important function of the human vertebral column is stability and weight transmission and it is also adapted to protect the spinal cord. Congenital or acquired anomalies are common in the vertebral column. The ligamentum longitudinale anterius (anterior longitudinal ligament) is a broad and strong band of fibrous tissue that runs along the anterior surfaces of the bodies of the vertebra. It extends from the axis to the upper, pelvic surface of the sacrum. It is thicker in the thoracic than in the cervical and lumbar regions and it acts as a guard against hyperextension of the spine. Disordered ossification or calcification of ligaments or cartilages may compress neurovascular structures and can cause serious implications in any surgical intervention in the region, and may lead to false neurological differential diagnosis [1,2].
Ossification of the ligamentum longitudinale anterius was classified as follows-
Segmental type of ossification (partial or total ossification over a vertebral body without involving the disc space).
Continuous type of ossification (Continuous ossification over many disc spaces as well as the vertebral body).
Mixed type of ossification (combination of the segmental and continuous types).
Ossified anterior longitudinal ligament may alter the biomechanics of the lumbar spine and may results in low back pain, kyphosis, scoliosis and Bechterew’s disease (Ankylosing Spondylitis). Ossification of the anterior longitudinal ligament has not been widely described in the modern medical literature.
Accordingly, in the present study we aimed to evaluate the incidence of ossification of ligamentum longitudinale anterius in adult human vertebra as segmental or complete or incomplete.
Materials and Methods
This study was carried out on 95 sets of dry human vertebral columns (Each set of vertebral column contain 7-Cervical, 12-Thoracic, 5-lumbar and 1-sacrum) irrespective of age and sex at Mayo Institute of Medical Sciences- Barabanki,-UP, Melaka Manipal Medical College-Manipal University and Department of Anatomy, KMCT Medical College, Manassery- Calicut, India and it was recorded whether the incidence of calcification and ossification of ligamentum longitudinale anterius in adult human vertebra was segmental or complete or incomplete. Photographs of the Lumbosacral transitional vertebra were taken for proper documentation.
Results
It was observed that out of 95 sets of dry human vertebral columns, 27 (28.42%) vertebral columns showed ossification of ligamentum longitudinale anterius [Table/Fig-1].
Showing different types ossification of ligamentum longitudinale anterius at different vertebral levels
| Verbrael Level | Segmental type of ossification | Continuous type of ossification | Mixed type of ossification |
|---|
| Cervical (C) | 1. C6 and C7 2. C3 to C5 | _ | 1. C3 to C5 2. C3 to C6 |
| Thoracic (T) | 1. T1 to T3 2. T5 to T12 3. T6 to T8 | 1. T10 to T12 2. T10 and T11 | I. In 2 Vertebral Columns: T4 To T6 Ii.In4vertebral Columns: T3 To T6 Vertebrae |
| Lumbar (L) | I. In 5 Vertebra Columns: L1 To L5. Ii.In4vertebral Columns: L4 And L5 Iii.In3vertebral Columns: L3 To L5 | - | - |
Out of 27 vertebral columns the following types of ossification of ligamentum longitudinale anterius were noted- [Table/Fig-1].
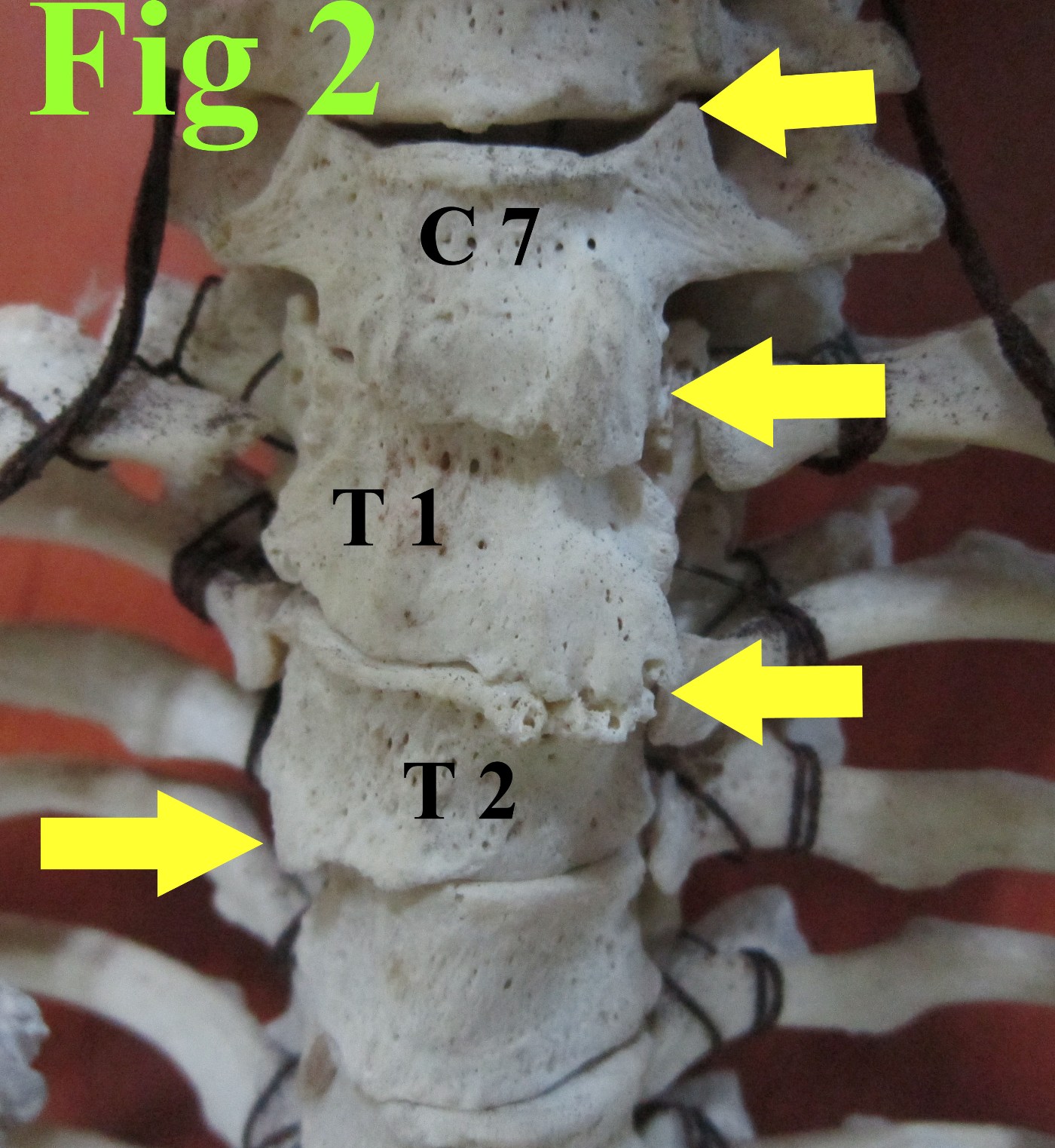
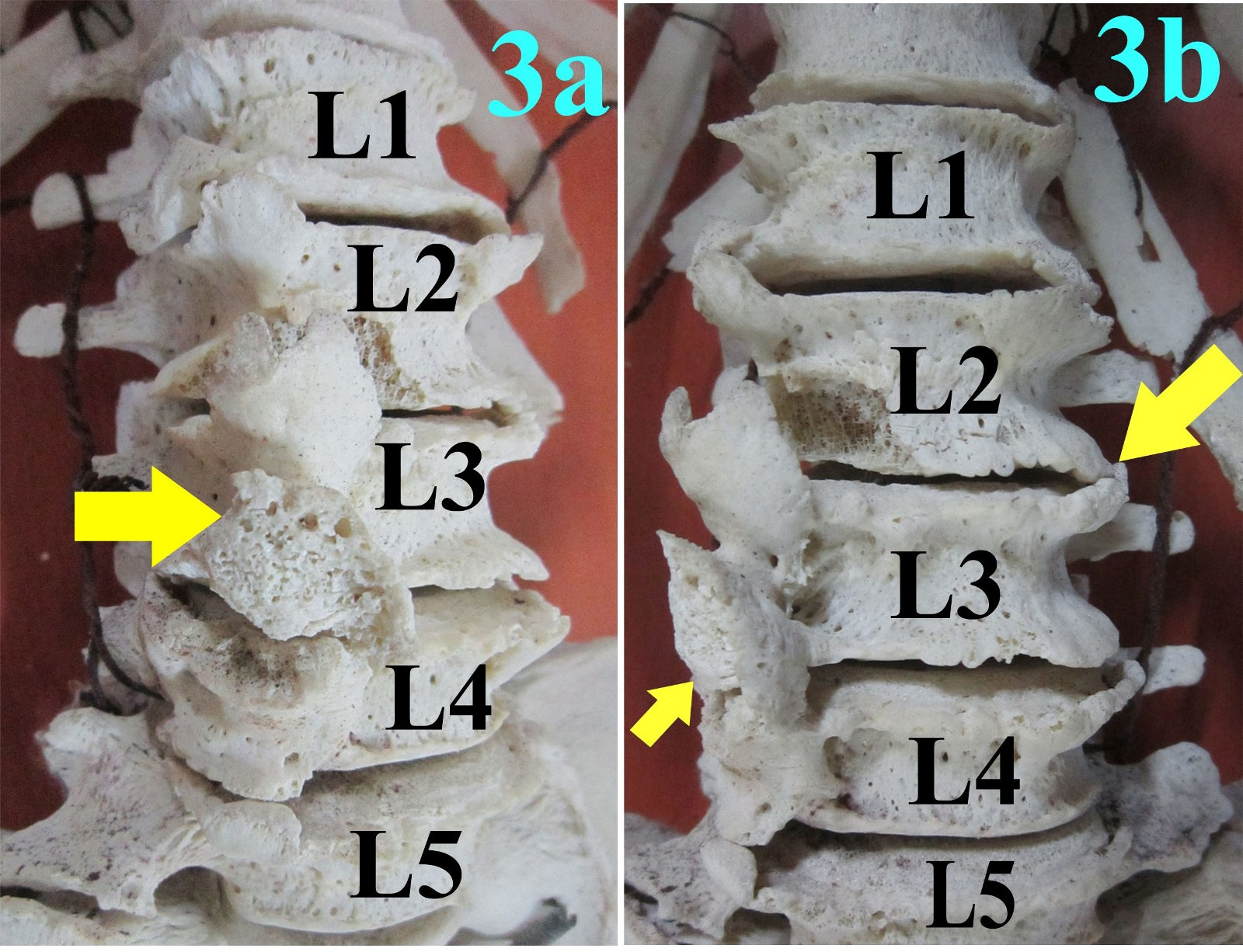
Segmental type of ossification {17 (17.89%)}: [Table/Fig-2,3a,3b].
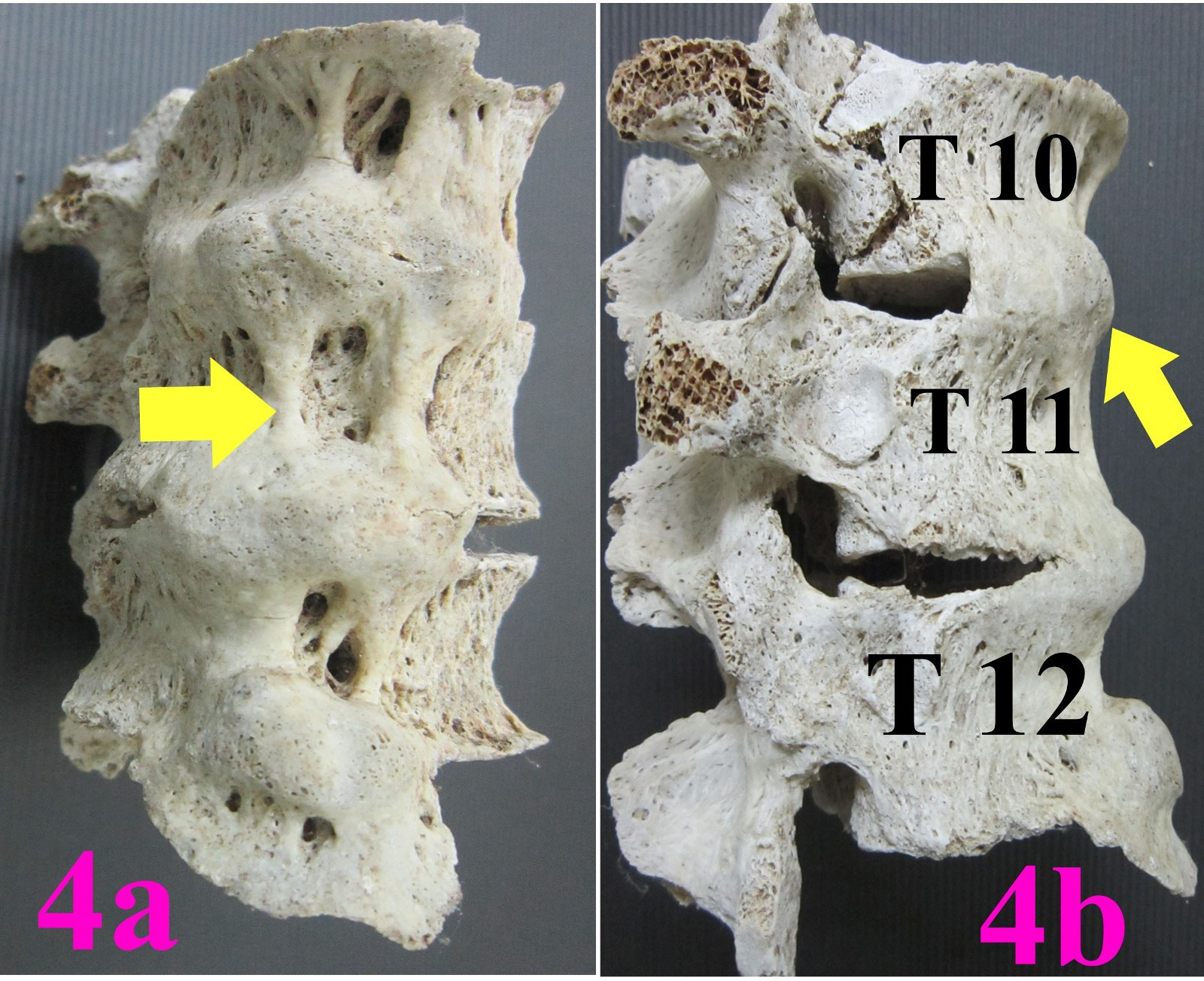
Continuous type of ossification {2 (2.11%)}: [Table/Fig-4a,4b].
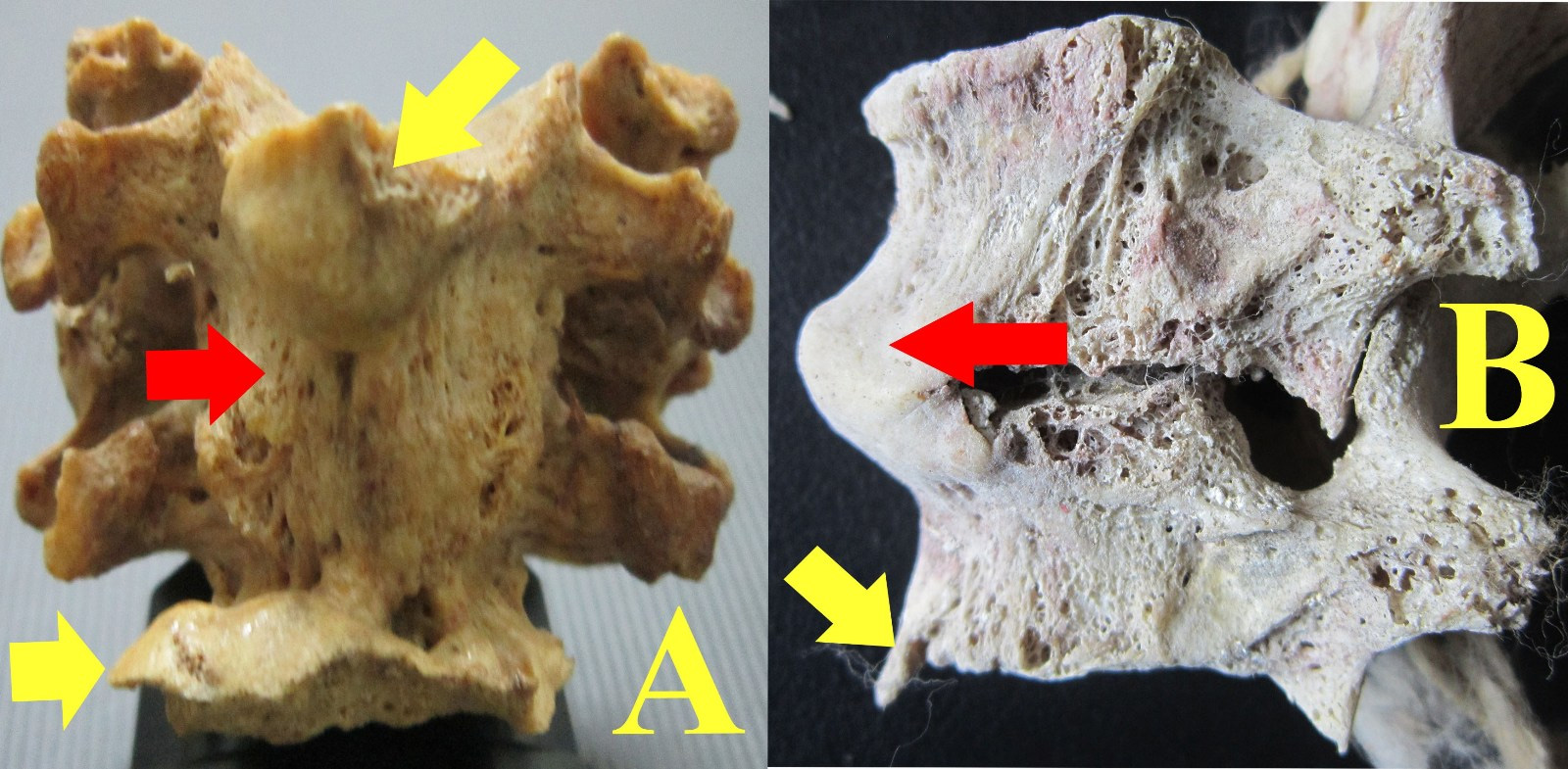
Mixed type of ossification {8 (8.42%)}: [Table/Fig-5].
Segmental type of ossified ligamentum longitudinale anterius (Yellow Arrows) at cervical and thoracic level. C7- 7th Cervical Vertebra; T1 and T2- Thoracic vertebra one and two
Showing segmental type of ossification of ligamentum longitudinale anterius (Yellow Arrows) at lumbar level. (1,2,3,4,5-Five lumbar vertebrae. 3a: Anterior view, 3b: Lateral view)
Showing continuous type of ossification of ligamentum longitudinale anterius (Yellow Arrows) at thoracic level. (T10, T11, T12: tenth, eleventh and twelfth thoracic vertebrae. 4a:Anterior view, 4b:Lateral view)
Showing mixed type of ossification of ligamentum longitudinale anterius at cervical (A) and thoracic (B) level. (Yellow arrow: Segmental type; Red arrow: Continuous type)
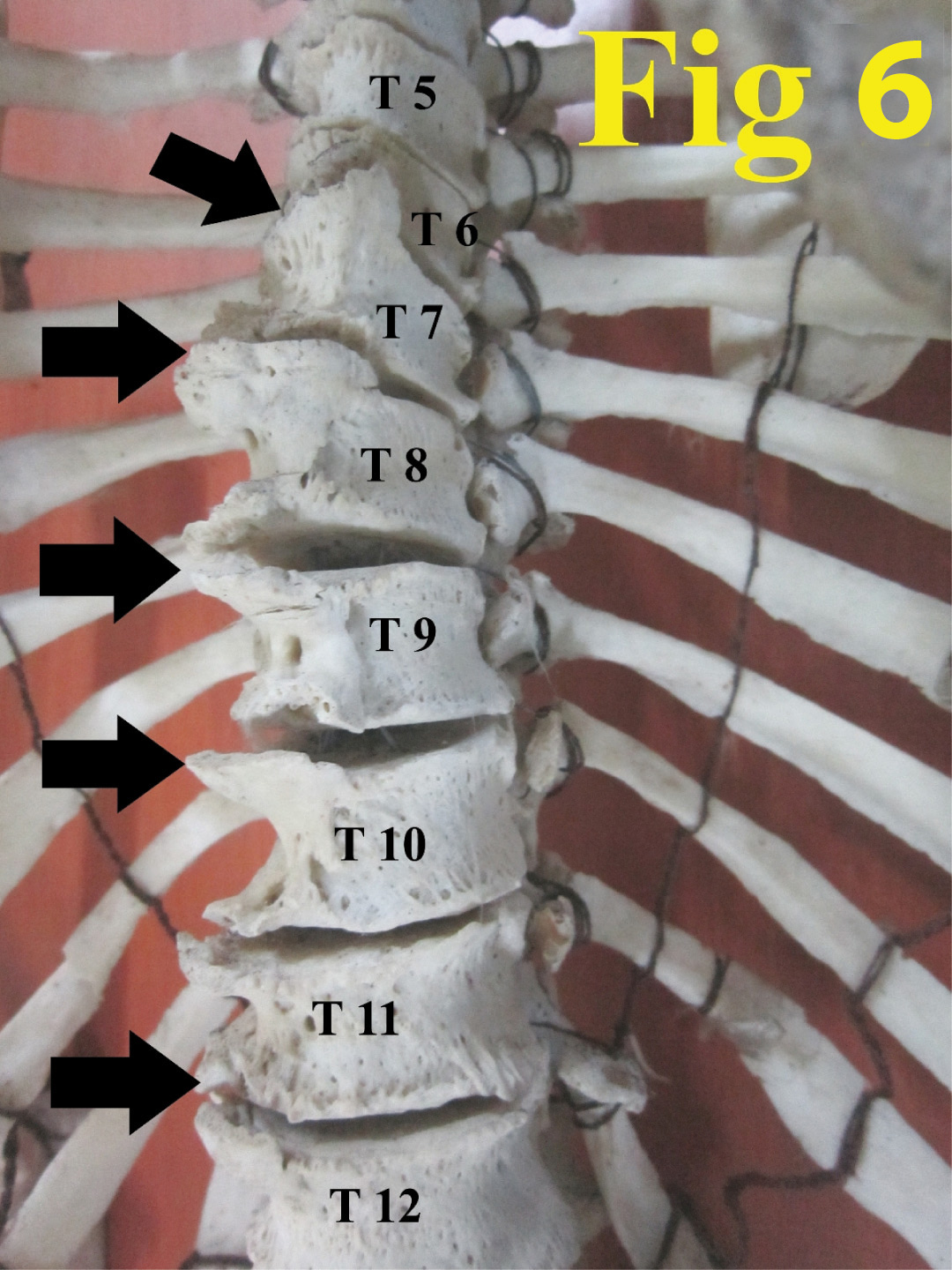
We also noted an unusual thickened and anteriorly projected segmental type of ossified anterior longitudinal ligament close to the margins of vertebral bodies. Maximum length (3.9 cm) of the entire anteriorly projected segmental type of ossified anterior longitudinal ligament was noted in two vertebral columns [Table/Fig-6, 3a, 3b].
Showing unusual thickened and anteriorly projected segmental type of ossified anterior longitudinal ligamentum longitudinale anterius (Black arrows) close to the margins of vertebral bodies at thoracic level. (T5 to T12- Thoracic vertebra five to twelve)
Discussion
Diffuse idiopathic skeletal hyperostosis often referred to as “Forestier” disease characterized by a tendency toward diffuse calcification and ossification of ligaments especially the ligamentum longitudinale anterius along the anterolateral margins of at least four contiguous vertebral bodies [3]. Ossified ligamentum longitudinale anterius typically characterized by variable thickness and seems to be a candle wax dripping down the spine. While the thoracic anterior longitudinal ligament is ossified, the areas of ossification often meet without fusion, it most characteristically affects the spine, [4] similar type of ossified anterior longitudinal ligament was noted in our study [Table/Fig-3a,3b]. Thickened and anteriorly projected (maximum length 3.9 cm of the entire anteriorly projected segmental type of ossified anterior longitudinal ligament) ossified anterior longitudinal ligament close to the margins of vertebral bodies noted in this study [Table/Fig-6,3a,3b] made this study unique, as such cases may increase the prevalence of spinal cord and soft-tissue injuries after even minor trauma.
Dysphagia may occur after a stroke, throat and mouth cancer, gastro-oesophageal reflux disease, or as symptoms of several different neurological disorders or retropharyngeal abscess. Ossified anterior longitudinal ligament may lead to the compression of the oesophagus and trachea [5–8]. Retropharyngeal space is a potential or dead space present behind the pharynx and in front of the cervical vertebrae, pre and paravertebral muscles and it allows the free expansion of the pharynx during deglutition. Ossification of ligamentum longitudinale anterius noted at this region may reduce the retropharyngeal space leading to dysphagia (difficulty in swallowing) or odynophagia (painful swallowing).Thus, the sound knowledge of the ossified ligamentum longitudinale anterius in this region can increase the success of diagnostic evaluation of the region.
Suba Anathi K et al., [9] reported continuous type of ossification of the anterior longitudinal ligament in the cervical region [cervical vertebrae (C2 -C6)], where as in this study we noted segmental and mixed type of ossification [Table/Fig-1]. Such type of ossification may compress the larynx or trachea and lead to the immobility or mucosal thickening of larynx or dysphagia [10], and may compress the recurrent laryngeal nerve causing recurrent laryngeal nerve palsy or bilateral nerve damage which can result in breathing difficulties and aphonia (the inability to speak).
The ligamentum longitudinale anterius helps to maintain stability and prevent hyperextension of vertebral column [11]. Unusual segmental type of ossification of ligamentum longitudinale anterius in the thoracic vertebrae [Table/Fig-2,6] noted in this study may increase the stiffness of the backbone and the restriction of thorax mobility for respiratory movements and may lead to development of pulmonary diseases. As per our knowledge such abnormal segmental type of ossification of ligamentum longitudinale anterius has not been cited in the recent medical literature.
The main function of lumbar vertebrae is to support the upper body, transfer weight from axial to appendicular skeleton, and provide mobility in the lower back. Ossification of ligamentum longitudinale anterius at this region will affect the biomechanics of the lumbar spine and results in low back pain problem. Ossification of ligamentum longitudinale anterius at the level of the 5th lumber vertebra and sacrum may lead to increased risk for advanced disc degeneration or disc herniation above the vertebrae [12]. A rare segmental type of ossification of ligamentum longitudinale anterius in the lumbar vertebrae was noted in this study [Table/Fig-3a,3b]. Knowledge of such ossification is not only enlightening for the orthopaedic surgeons but also vital for the clinical anatomist, Radiologists, Forensic experts, Architectures and morphologists. Increased tension upon certain fibers of the longitudinal ligaments [13], disordered pyrophosphate metabolism hypercalcemia may play a key role in the ossification of ligamentum longitudinale anterius.
Spondylosis is usually diagnosed in the cervical, thoracic, and lumbar regions and is often classified as cervical spondylosis, thoracic spondylosis, and lumbar spondylosis. Prevalence of ossified ligamentum longitudinale anterius noted in this study is 28.42%, such abnormalities may cause cervical spondylosis manifested by neck pain and stiffness resulting in limitation of movement of neck and numbness or weakness in arms, hands, and fingers due to compression of the brachial plexus that innervate the upper extremity.
Conclusion
Ossification of ligamentum longitudinale anterius will affect the biomechanics of the lumbar spine and may result in stiff neck, low back pain, dysphagia, odynophagia, compression of the brachial plexus, recurrent laryngeal nerve palsy, aphonia, and immobility or mucosal thickening of larynx. We believe that the present study has provided some important data which will contribute to the scientific literature, and such abnormal ligamentum longitudinale anterius should be kept in mind for orthopaedic surgeons, radiologists, forensic experts and morphologists to minimise serious complications in any surgical intervention or investigative procedures in the region.
[1]. Chakravarthi KK, Venumadhav N, Ravindranath G, Abnormal bone outgrowths and osseous structures around the foramen ovale may leads to mandibular compression or entrapment neuropathyInt J Bioassays 2013 2:922-25. [Google Scholar]
[2]. Chakravarthi KK, Sarath Babu K, An anatomical study of the pterygo-alar bar and porus crotaphitico buccinatoriusInt J Med Health Sci 2012 1:3-9. [Google Scholar]
[3]. Dodia AV, Pratik DS, Soman SM, Diffuse Idiopathic Skeletal Hyperostosis (DISH)-a Rare Presentation of the DiseaseIndian Journal of Applied Research 2013 3:587-89. [Google Scholar]
[4]. Miyazawa N, Akiyama I, Ossification of the ligamentum flavum of the cervical spineJ Neurosurg Sci 2007 51:139-44. [Google Scholar]
[5]. Mizuno J, Nakagawa H, Song J, Symptomatic ossification of the anterior longitudinal ligament with stenosis of the cervical spine: a report of seven casesJ Bone Joint Surg Br 2005 87:1375-79. [Google Scholar]
[6]. Resnick D, Shapiro RF, Wiesner KB, Diffuse idiopathic skeletal hyperostosis (DISH) (ankylosing hyperostosis of Forester and Rotes-Querol)Semin Arthritis Rheum 1978 7:153-87. [Google Scholar]
[7]. Underberg-Davis S, Levine MS, Giant thoracic osteophyte causing oesophageal food impactionAm J Roentgenol 1991 157:319-20. [Google Scholar]
[8]. Stuart D, Dysphagia due to cervical osteophytes: a description of five patients and a review of the literatureInt Orthop 1989 13:95-99. [Google Scholar]
[9]. Suba Anathi K, Agrawal Reena, Agrawal Sanjeeb, Multiple Cervical Vertebral Fusion with Ossification of Anterior Longitudinal LigamentAnatomical journal of Africa 2013 2:128-31. [Google Scholar]
[10]. Epstein N, Hollingsworth R, Ossification of the cervical anterior longitudinal ligament contributing to dysphagia - Case reportJournal of Neurosurgery 1999 90:261-63. [Google Scholar]
[11]. Standaring S, Gray’s Anatomy 2000 38th edititionNewyorkChurchill Livingstone:532-36. [Google Scholar]
[12]. Chakravarthi KK, Venumadhav N, Siddaraju KS, Morphological study on lumbosacral transitional vertebra in adult Indian sacra and its clinical implicationsIJABPT 2013 4:340-46. [Google Scholar]
[13]. Oppenheimer Albert, Calcification and Ossification of Vertebral LigamentsRadiology 1942 38:160-73. [Google Scholar]