Dexamethasone as An Additive to Bupivacaine in Fascia Lliaca Compartment Block: A Prospective, Randomized and Double Blind Study
Suresh Kumar N1, Kiran N2, Ravi M3, Don Sebastian4, Punith Gowda RM5
1 Assistant Professor, Department of Anaesthesiology, Sri Devaraj Urs Medical College, Tamaka, Kolar, Karnataka, India.
2 Assistant Professor, Department of Anaesthesiology, Sri Devaraj Urs Medical College, SDUAHER, Tamaka, Kolar, Karnataka, India.
3 Professor, Department of Anaesthesiology, Sri Devaraj Urs Medical College, SDUAHER, Tamaka, Kolar, Karnataka, India.
4 Tutor, Department of Anaesthesiology, Sri Devaraj Urs Medical College, SDUAHER, Tamaka, Kolar, Karnataka, India.
5 Tutor, Department of Anaesthesiology, Sri Devaraj Urs Medical College, SDUAHER, Tamaka, Kolar, Karnataka, India.
NAME, ADDRESS, E-MAIL ID OF THE CORRESPONDING AUTHOR: Dr. Ravi. M, Professor, Anaesthesiology, Sri Devaraj Urs Medical College, SDUAHER, Tamaka, Kolar, Karnataka, India.
Phone: 9845287591,
E-mail: ravijaggu@gmail.com
Background: Patients with fracture femur experience severe pain on movement during positioning for spinal anaesthesia. Fascia Iliaca Compartment Block (FICB) has been used effectively for providing analgesia during positioning of the patient for spinal anaesthesia.
Aim: To test the hypothesis that, adding dexamethasone would significantly prolong the duration of Bupivacaine in FICB.
Materials and Methods: Sixty patients aged 18 to 80 years posted for ORIF (Open Reduction and Internal Fixation) of fracture femur were included to receive FICB. This was a prospective, randomized, double blind study done at tertiary medical college hospital. Thirty patients received 38ml of 0.25 % bupivacaine with 2ml saline and another 30 patients received 38ml of 0.25 % bupivacaine with 2ml dexamethasone (8mg). Thirty minutes after FICB, patient satisfaction during positioning for spinal anesthesia was recorded. In the post-operative period, duration of analgesia and the total doses of rescue analgesics were recorded in both the groups.
Results: Patients who received Bupivacaine with dexamethasone had significant prolongation of analgesia and required fewer doses of rescue analgesics as compared to patients who received Bupivacaine alone for FICB. However, the onset of analgesia, VAS scores and patient satisfaction during positioning for spinal anaesthesia were similar in both groups.
Conclusion: Our study shows that adding Dexamethasone (8mg) to Bupivacaine for FICB significantly prolonged the duration of block and decreased the requirement of rescue analgesics as compared to patients who received Bupivacaine alone. FICB is relatively easy and safe to perform. In our study we did not encounter any complication while doing the procedures and also by adding dexamethasone.
Fracture femur, Nerve block, Patient positioning
Introduction
Fracture femur is a common injury which is associated with excruciating pain. Fractures may involve the femoral neck, shaft or distal femur. These operations are more often managed with regional anaesthesia techniques. Positioning for neuraxial blocks is always challenging because, even slight overriding of the fracture ends, is intensely painful [1]. Hence, prior to neuraxial blockade, analgesia is provided by conventional modes of pain relief like non-steroidal anti-inflammatory drugs (NSAIDs), opioids and also by peripheral nerve blocks such as, femoral nerve block, 3 in 1 block and Fascia iliaca compartment block (FICB). Conventional pain treatment (NSAIDs, paracetamol and IV morphine) has undesirable side-effects, many of those being particularly unwanted in patients with high co-morbidity. Opioids may cause respiratory depression, hypotension, dizziness, mental confusion, constipation, itching, urine retention and nausea. NSAIDs may cause gastrointestinal haemorrhage and affect renal function. Amongst the procedures, FICB is believed to be advantageous because of its safety and efficacy. It has been demonstrated that FICB provides effective analgesia for fracture femur when given preoperatively [2].
In comparison to epidural analgesia, Peripheral Nerve Blocks (PNB), despite providing effective unilateral analgesia, also reduces the incidence of opioid-related and autonomic side-effects, produces less motor blockade, and fewer, neurological complications [3,4]
Many adjuvants like epinephrine, clonidine, opioids, ketamine, and midazolam were combined with local anaesthetics to prolong the duration of analgesia from nerve blocks, but have met with limited success. However, the glucocorticoid dexamethasone has been shown to be effective in a small number of preclinical [5,6] and clinical studies [7–10].
Steroid injections produce a degree of vasoconstriction, so one theory suggests that the drug acts by reducing local anaesthetic absorption. Another theory tells that dexamethasone potentiates the activity of inhibitory potassium channels on nociceptive C-fibres (via glucocorticoid receptors), thereby decreasing their activity [11].
Aim
Aim of the study was to check the effectiveness of FICB for patient positioning during spinal anaesthesia and to compare the duration of postoperative analgesia using Bupivacaine alone and Dexamethasone with Bupivacaine.
Materials and Methods
After obtaining Institutional ethical committee approval and informed written consent from the patients, we studied 60 patients.
Inclusion Criteria: ASA grade 1 patients aged between 18 to 80-years who were planned for ORIF of fracture femur under Spinal anaesthesia.
Exclusion Criteria: Patients refusal, allergy to local anaesthetics, peripheral neuropathy, bleeding diathesis, previous femoral bypass surgery, inguinal hernia, inflammation or infection over injection site, morbid obesity, patients on previous opioid therapy, psychiatric disorders and polytrauma.
Patients were randomized into two groups using a computer generated random number table. Group B (38ml of 0.25% Bupivacaine + 2ml saline) and Group BD (38ml of 0.25% Bupivacaine + 2ml dexamethasone ). Medication was prepared by a staff member who was not involved in the study and delivered in unidentifiable syringes. All blocks were performed by trained anaesthetists.
Patients were monitored with electrocardiography, pulse-oximetry and non-invasive blood pressure prior to FICB and throughout the procedure. The procedure and technique of the FICB was done as described by Dalens et al., [12]. A line is drawn on the skin from anterior superior iliac spine to pubic tubercle. Needle insertion is 1cm caudad to junction between lateral and middle third. Under aseptic precautions, skin and deeper tissues infiltrated with 1% Lidocaine. Using a blunted or short-beveled needle skin was pierced at right angle to its surface. Identification of the correct compartment was based on two ‘gives’ followed by a loss of resistance; first ‘give’ felt is fascia lata and second is fascia iliaca. We used a blunt 21G hypodermic needle to make it easier to feel the ‘give’. Local anaesthetic was injected in 5ml aliquots after negative aspiration.
There should be no resistance to injection. If the needle tip is likely to be within iliacus muscle, then withdraw slightly until injection is easy. There should be no pain or paraesthesia on injection. Patients comfort while positioning for spinal anaesthesia were noted 30 minutes after FICB using VAS scores. All adverse effects were noted.
The severity of postoperative pain was assessed by a blinded study team member using a visual analog score(VAS) upon admission to the Surgical I.C.U. Patients reporting pain scores 4 and above were given Intravenous (i.v) Tramadol (100 mg) as rescue analgesia.
Statistical Analysis
Descriptive and inferential statistical analysis has been carried out in the present study. Results on continuous measurements are presented on Mean + SD (Min-Max) and results on categorical measurements are presented in Number (%). Significance is assessed at 5 % level of significance.
Student t-test (two tailed, independent) has been used to find the significance of study parameters on continuous scale between two Groups. Inter Group analysis on metric parameters.
Chi-square/ Fisher Exact test has been used to find the significance of study parameters on categorical scale between two or more Groups.
Significant Figures
+ Suggestive significance (p-value: 0.05<P 0.10)
* Moderately significant (p-value:0.01<P 0.05)
** Strongly significant (p-value : P 0.01)
Statistical software: The statistical software namely SAS 9.2, SPSS 15.0, Stata 10.1, MedCalc 9.0.1 ,Systat 12.0 and R environment ver.2.11.1 were used for the analysis of the data and Microsoft word and Excel have been used to generate graphs, tables etc.
A total of 60 patients were recruited for the study [Table/Fig-1]. Age, gender and ASA grades were comparable in between the Groups. VAS scores done 30 minutes after FICB were comparable between the 2 Groups and did not show any statistically significant difference [Table/Fig-2].
| Duration of analgesia(Hrs) | Group B | Group BD |
|---|
| No | % | No | % |
|---|
| 1-5 | 0 | 0.0 | 0 | 0.0 |
| 6-10 | 27 | 90.0 | 6 | 20.0 |
| 11-15 | 3 | 10.0 | 6 | 20.0 |
| 16-20 | 0 | 0.0 | 10 | 33.3 |
| >20 | 0 | 0.0 | 8 | 26.7 |
| Total | 30 | 100.0 | 30 | 100.0 |
| Mean ± SD | 7.85±1.62 | 16.33±5.69 |
Duration of analgesia is significant in Group B with P <0.001**
Total doses of rescue analgesia
| Total doses of rescue analgesia | Group B | Group BD |
|---|
| No | % | No | % |
|---|
| 0 | 0 | 0.0 | 8 | 26.7 |
| 1 | 5 | 16.7 | 17 | 56.7 |
| 2 | 18 | 60.0 | 4 | 13.3 |
| 3 | 7 | 23.3 | 1 | 3.3 |
| Total | 30 | 100.0 | 30 | 100.0 |
Total dose of rescue analgesia is significantly more in Group B with p < 0.001**
In our study, the duration of analgesia was significantly longer in Group BD when compared to Group B (p<0.001**) as seen in [Table/Fig-3]. Total doses of rescue analgesics required were significantly higher in Group B, as shown in [Table/Fig-4].
| AGE IN YEARS | MALE | FEMALE |
|---|
| 18-29 | 18 | 0 |
| 30-39 | 9 | 3 |
| 40-49 | 5 | 3 |
| 50-59 | 4 | 2 |
| 60-69 | 6 | 2 |
| 70-80 | 5 | 3 |
| VAS score | Group B | Group BD |
|---|
| No | % | No | % |
|---|
| 0 | 4 | 13.3 | 4 | 13.3 |
| 1 | 7 | 23.3 | 7 | 23.3 |
| 2 | 10 | 33.3 | 13 | 43.3 |
| 3 | 8 | 26.7 | 6 | 20.0 |
| Total | 30 | 100.0 | 30 | 100.0 |
Distribution of VAS score is statistically similar in two Groups with p=0.904
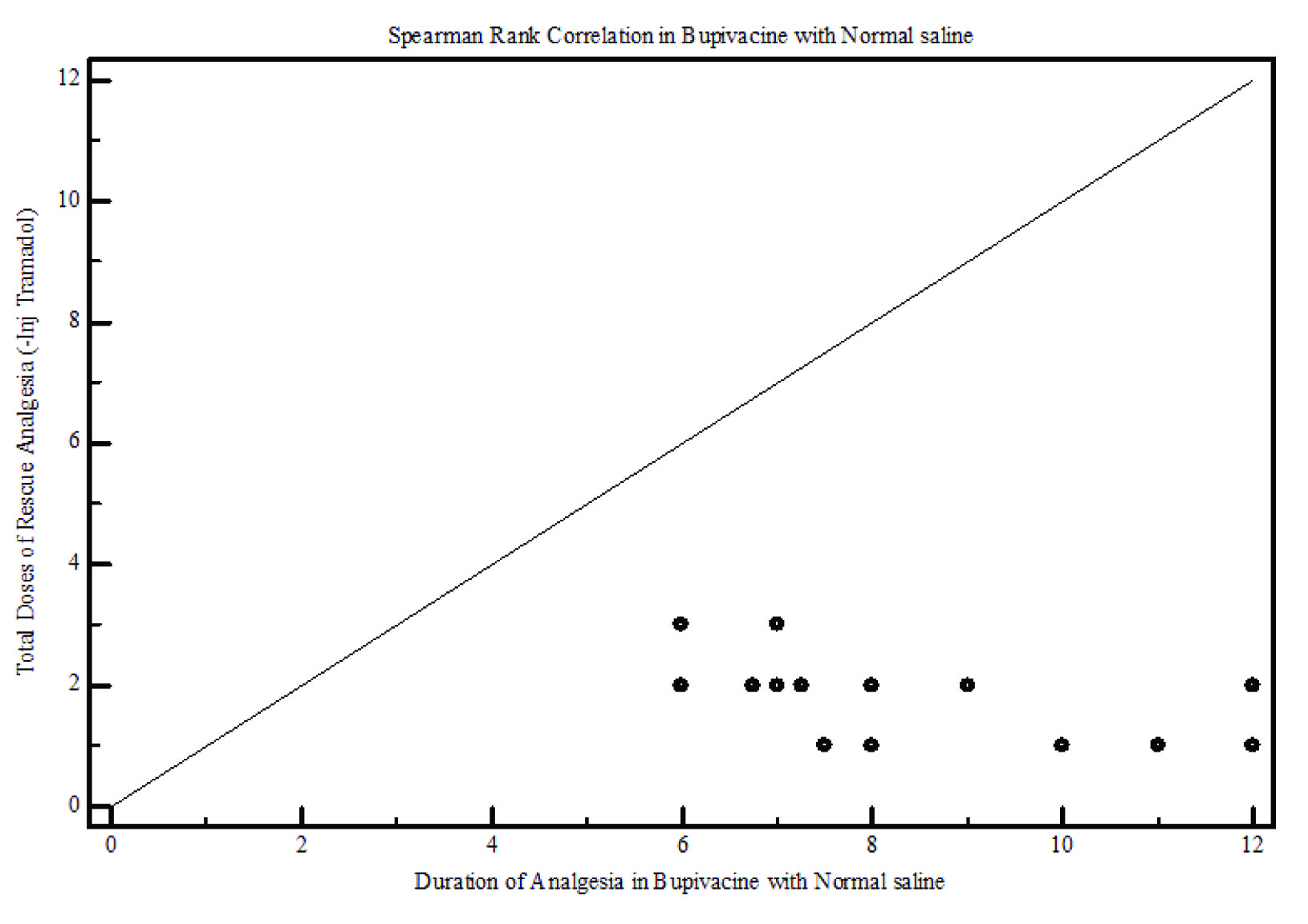
Spearman rank correlation shows a moderate negative correlation, as duration of analgesia is reduced there is increased requirement of total doses of rescue analgesics in Group B [Table/Fig-5].
Duartion of analgesia Group B
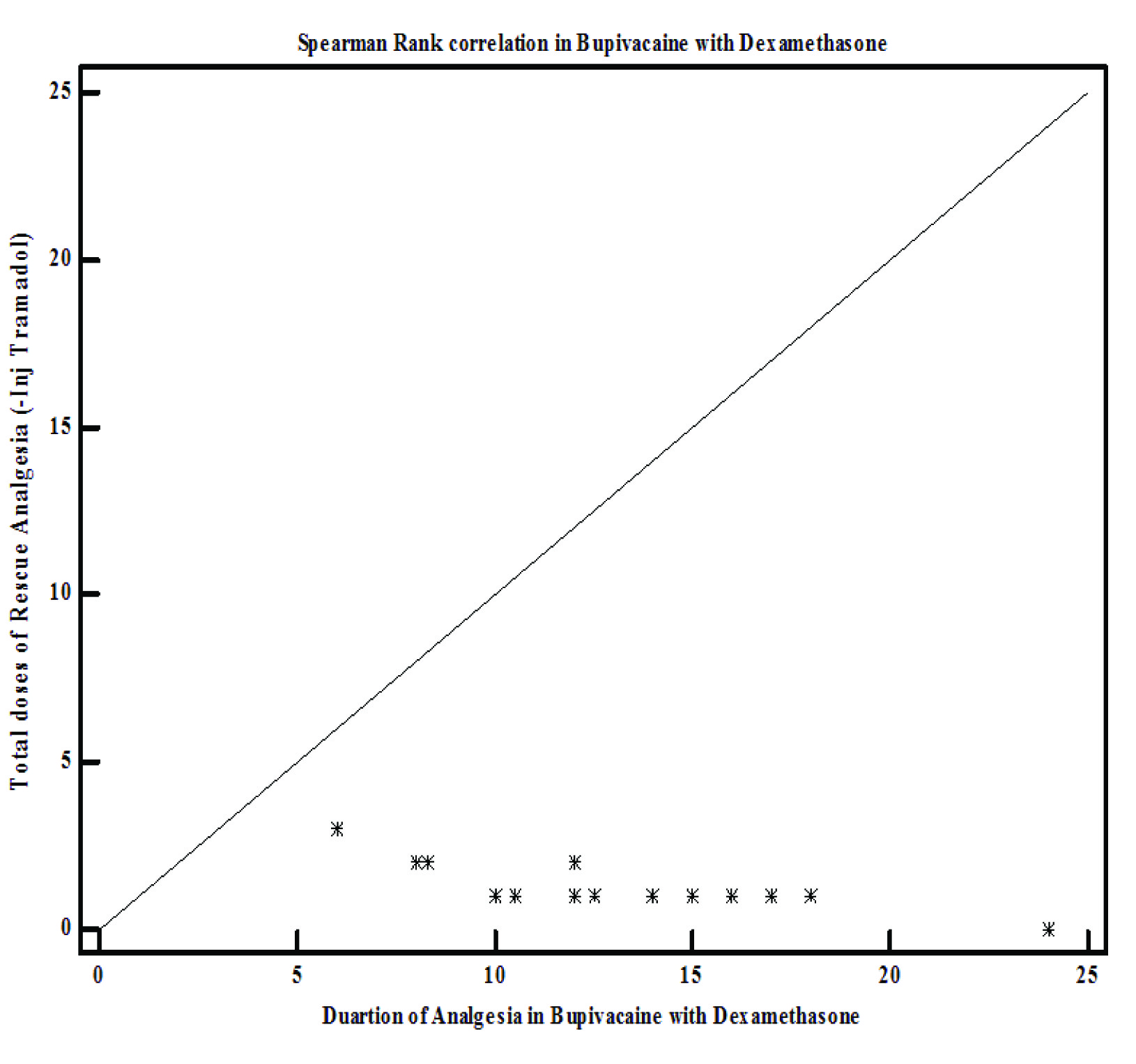
And in Group BD there is weak negative correlation, as duration of analgesia is more there is fewer requirements of rescue analgesic doses [Table/Fig-6].
Duration of Analgesia Group BD
Discussion
The FICB was first described in 1989 and was performed initially on children and later on adults. It was mainly used to provide analgesia following surgical procedures in the hip, femur and knee, treatment of burns on the thigh and in prehospital treatment of fracture femur [13,14].
Candal-Couto et al., demonstrated that FICB allows patients being able to tolerate a sitting position with femoral neck fractures [15].
FICB is more effective in blocking lateral cutaneous nerve of thigh and femoral nerve [16]. The FICB is not only easy to perform but it is also associated with minimal risk as the analgesic is injected at a safe distance from the femoral artery and femoral nerve. It is always safe to perform the FICB prior to spinal anaesthesia as the patient can respond during administration of the local anaesthetic and can prevent intraneuronal injections [17]. There are reports of postoperative neuropathy when FICB was attempted after spinal anaesthesia [18].
This study is the first to examine the effect of dexamethasone on plain bupivacaine for FICB in patients with fracture femur. We observed that prolongation of block duration was 1.5 to 2 times when dexamethasone was added as an additive to plain bupivacaine. This block prolongation was also observed when dexamethasone was combined with mepivacaine for supraclavicular blocks [8]. Similarly, K. C. Cummings 3rd et al., [19] also observed that, dexamethasone significantly prolonged the duration of ropivacaine and bupivacaine when used for the interscalene block. However, the existing literature supports the clinically important benefit we observed in our study.
Elderly patients with fracture femur are more prone to delirium because of pain and medications. Adequate analgesia not only prevents delirium but also, allows increased mobility and shorter hospital stay [20]. Analgesia provided by femoral nerve blockade can be compared to that of epidural analgesia but, with a lower incidence of hypotension [21–23].
Till date no trial has reported neurotoxicity attributable to dexamethasone. In our study, no adverse events were detected. Additionally, epidural corticosteroids have been used safely for a long time in treating patients with radicular pain arising from nerve root irritation [24]. Dexamethasone in particular has been studied as an adjuvant to epidural local anaesthetics [25].
Steroids administered perineurally are eventually absorbed and produce systemic effects. Given i.v., several steroids have been shown to improve postoperative pain and reduce postoperative nausea and vomiting [26–29].
Conclusion
Our study demonstrates that FICB done prior to spinal anaesthesia would ensure patient comfort during positioning for SAB (Sub-arachnoid block) and also provide postoperative analgesia. Our study further tells that, by adding dexamethasone to plain bupivacaine would significantly prolong postoperative analgesia.
Duration of analgesia is significant in Group B with P <0.001**
Total dose of rescue analgesia is significantly more in Group B with p < 0.001**
Distribution of VAS score is statistically similar in two Groups with p=0.904
[1]. Adams HA, Saatweber P, Schmitz CS, Hecker H, Postoperative pain management in orthopaedic patients: no differences in painscore, but improved stress control by epidural anaesthesiaEur J Anaesthesiol 2002 19:658-65. [Google Scholar]
[2]. Foss NB, Kristensen BB, Bundgaard M, Bak M, Heiring C, Virkelyst C, Fascia iliaca compartment blockade for acute pain control in hip fracture patientsAnesthesiology 2007 106:773-78. [Google Scholar]
[3]. Chelly JE, Greger J, Gebhard R, Coupe K, Clyburn TA, Buckle R, Continuous femoral blocks improve recovery and outcome of patients undergoing total knee arthroplastyJ Arthroplasty 2001 16:436-45. [Google Scholar]
[4]. Horlocker TT, Kopp SL, Pagnano MW, Hebl JR, Analgesia for total hip and knee arthroplasty: a multimodal pathway featuring peripheral nerve blockJ Am Acad Orthop Surg 2006 14:126-35. [Google Scholar]
[5]. Colombo G, Padera R, Langer R, Kohane DS, Prolonged duration local anesthesia with lipid-protein-sugar particles containing bupivacaine and dexamethasoneJ Biomed Mater Res A 2005 75:458-64. [Google Scholar]
[6]. Drager C, Benziger D, Gao F, Berde CB, Prolonged intercostal nerve blockade in sheep using controlled-release of bupivacaine and dexamethasone from polymer microspheresAnesthesiology 1998 89:969-79. [Google Scholar]
[7]. Movafegh A, Razazian M, Hajimaohamadi F, Meysamie A, Dexamethasone added to lidocaine prolongs axillary brachial plexus blockadeAnesth Analg 2006 102:263-67. [Google Scholar]
[8]. Parrington SJ, O’Donnell D, Chan VW, Brown-Shreves D, Subramanyam R, Qu M, Dexamethasone added to mepivacaine prolongs the duration of analgesia after supraclavicular brachial plexus blockadeReg Anesth Pain Med 2010 35:422-26. [Google Scholar]
[9]. Shrestha BR, Maharjan SK, Tabedar S, Supraclavicular brachial plexus block with and without dexamethasone—a comparative studyKathmandu Univ Med J 2003 1:158-60. [Google Scholar]
[10]. Vieira PA, Pulai I, Tsao GC, Manikantan P, Keller B, Connelly NR, Dexamethasone with bupivacaine increases duration of analgesia in ultrasound-guided interscalene brachial plexus blockadeEur J Anaesthesiol 2010 27:285-88. [Google Scholar]
[11]. Attardi B, Takimoto K, Gealy R, Severns C, Levitan ES, Glucocorticoid induced up-regulation of a pituitary K+ channel mRNA in vitro and in vivoReceptors Channels 1993 1:287-93. [Google Scholar]
[12]. Dalens B, Vanneuville G, Tanguy A, Comparison of the fascia iliaca compartment block with the 3-in-1 block in childrenAnesth Analg 1989 69:705-13. [Google Scholar]
[13]. Cuignet O, Mbuyamba J, Pirson J, The long-term analgesic efficacy of a single-shot fascia iliaca compartment block in burn patients undergoing skin-grafting proceduresJ Burn Care Rehabil 2005 26:409-15. [Google Scholar]
[14]. Lopez S, Gros T, Bernard N, Plasse C, Capdevila X, Fascia iliaca compartment block for femoral bone fractures in prehospital careReg Anesth Pain Med 2003 28:203-07. [Google Scholar]
[15]. Candal-Couto JJ, McVie JL, Haslam N, Innes AR, Rushmer J, Pre-operative analgesia for patients with femoral neck fractures using a modified fascia iliaca block techniqueInjury 2005 36:505-10. [Google Scholar]
[16]. Morau D, Lopez S, Biboulet P, Bernard N, Amar J, Capdevila X, Comparison of continuous 3-in-1 and fascia iliaca compartment blocks for postoperative analgesia: feasibility, catheter migration, distribution of sensory block, and analgesic efficacyReg Anesth Pain Med 2003 28:309-14. [Google Scholar]
[17]. Capdevila X, Biboulet P, Bouregba M, Barthelet Y, Rubenovitch J, d’Athis F, Comparison of the three-in-one and fascia iliaca compartment blocks in adults: clinical and radiographic analysisAnesth Analg 1998 86:1039-44. [Google Scholar]
[18]. Gros T, Bassoul B, Dareau S, Delire V, Roche B, Eledjam JJ, Postoperative neuropathy following fascia iliaca compartment blockadeAnn Fr Anesth Reanim 2006 25:216-17. [Google Scholar]
[19]. Cummings KC 3rd, Napierkowski DE, Parra-Sanchez I, Kurz A, Dalton JE, Brems JJ, Effect of dexamethasone on the duration of interscalene nerve blocks with ropivacaine or bupivacaineBr J Anaesth 2011 107:446-53. [Google Scholar]
[20]. Mouzopoulos G, Vasiliadis G, Lasanianos N, Nikolaras G, Morakis E, Kaminaris M, Fascia iliaca block prophylaxis for hip fracture patients at risk for delirium: a randomized placebo-controlled studyJ Orthop Traumatol 2009 10:127-33. [Google Scholar]
[21]. Fowler SJ, Symons J, Sabato S, Myles PS, Epidural analgesia compared with peripheral nerve blockade after major knee surgery: a systematic review and meta-analysis of randomized trialsBr J Anaesth 2008 100:154-64. [Google Scholar]
[22]. Choi PT, Bhandari M, Scott J, Douketis J, Epidural analgesia for pain relief following hip or knee replacementCochrane Database Syst Rev 2003 :CD003071 [Google Scholar]
[23]. Richman JM, Liu SS, Courpas G, Wong R, Rowlingson AJ, McGready J, Does continuous peripheral nerve block provide superior pain control to opioids? A meta-analysisAnesth Analg 2006 102:248-57. [Google Scholar]
[24]. Price C, Arden N K, Coglan L, Rogers P, Cost-effectiveness and safety of epidural steroids in the management of sciaticaHealth Technol Assess 2005 9:1-58. [Google Scholar]
[25]. Khafagy HF, Refaat AI, El-Sabae HH, Youssif MA, Efficacy of epidural dexamethasone versus fentanyl on postoperative analgesiaJ Anesth 2010 24:531-36. [Google Scholar]
[26]. Bisgaard T, Klarskov B, Kehlet H, Rosenberg J, Preoperative dexamethasone improves surgical outcome after laparoscopic cholecystectomy: a randomized double-blind placebo-controlled trialAnn Surg 2003 238:651-60. [Google Scholar]
[27]. Nagelschmidt M, Fu ZX, Saad S, Dimmeler S, Neugebauer E, Preoperative high dose methylprednisolone improves patients outcome after abdominal surgeryEur J Surg 1999 165:971-78. [Google Scholar]
[28]. Aasboe V, Raeder JC, Groegaard B, Betamethasone reduces postoperative pain and nausea after ambulatory surgeryAnesth Analg 1998 87:319-23. [Google Scholar]
[29]. Kardash KJ, Sarrazin F, Tessler MJ, Velly AM, Single-dose dexamethasone reduces dynamic pain after total hip arthroplastyAnesth Analg 2008 106:1253-57. [Google Scholar]