Relationship of High Sensitivity C-Reactive Protein Levels to Anthropometric and other Metabolic Parameters in Indian Children with Simple Overweight and Obesity
Devi Dayal1, Hemant Jain2, Savita Verma Attri3, Bhavneet Bharti4, Anil Kumar Bhalla5
1 Associate Professor, Department of Pediatrics, Advanced Pediatrics Center, Postgraduate Institute of Medical Education and Research, Chandigarh, India.
2 Registrar, Department of Pediatrics, Advanced Pediatrics Center, Postgraduate Institute of Medical Education and Research, Chandigarh, India.
3 Associate Professor, Department of Pediatrics, Advanced Pediatrics Center, Postgraduate Institute of Medical Education and Research, Chandigarh, India.
4 Associate Professor, Department of Pediatrics, Advanced Pediatrics Center, Postgraduate Institute of Medical Education and Research, Chandigarh, India.
5 Professor, Department of Pediatrics, Advanced Pediatrics Center, Postgraduate Institute of Medical Education and Research, Chandigarh, India.
NAME, ADDRESS, E-MAIL ID OF THE CORRESPONDING AUTHOR: Dr. Devi Dayal, Associate Professor, Department of Pediatrics, Pediatric Endocrinology & Diabetes Unit, Advanced Pediatrics Center, Postgraduate Institute of Medical Education and Research, Chandigarh-160012, India. Phone : 0091-172-2755657, 0091-172-2772777 , E-mail : drdevidayal@gmail.com
Context: High senstivity C-reactive protein (hsCRP) levels correlate well other parameters of obesity related metabolic syndrome (MS) and can be used as predictors of future cardiovascular disease risk. There is limited data on hsCRP levels in Indian children with simple obesity.
Aim: To study the relationship of hsCRP levels with various anthropometric as well as metabolic parameters in children with simple overweight and obesity.
Materials and Methods: This case control study was conducted in Paediatric Endocrinology clinic of a tertiary care hospital in Northern India. Levels of hsCRP were estimated in 100 overweight and obese children (BMI between 85th and 95th percentiles according to age & gender specific CDC 2000 growth charts) aged between 6 and 16 years and in 100 nearly age and sex matched healthy controls. These levels were then correlated to various anthropometric (body mass index, BMI; waist circumference, WC; hip circumference, HC; waist hip ratio, WHR; blood pressure) and biochemical (fasting blood glucose, FBG; total cholesterol, TC; high-density lipoprotein-cholesterol, HDL-C; low-density lipoprotein cholesterol, LDL-C; very low-density lipoprotein-cholesterol, VLDL-C; triglycerides, TG) parameters.
Results: Mean levels of hsCRP were significantly higher in the study group (3.92±2.20 versus 2.15±1.05 mg/L) as compared to controls. Significantly more (58% versus 10%) subjects in the study group had hsCRP (>3 mg/L). Of all the parameters studied, only BMI showed a positive correlation with hsCRP levels in the study group. Multiple logistic regression analysis for predicting outcome of high hsCRP showed positive correlation with BMI; with every 1 kg/m2 increase in BMI, odds of high hsCRP level were increased by 37% (OR=1.37; 95% CI 1.23-1.53, p-value <0.0001). Mean values of all the biochemical parameters except HDL-C were significantly higher in the study group.
Conclusion: Levels of hsCRP were significantly elevated in overweight and obese children as compared to non-obese children. In addition, these patients also showed abnormalities of lipid and glucose metabolism.
Childhood obesity, Subclinical inflammation, Hscrp levels
Introduction
The prevalence of overweight and obesity in children is increasing even in developing countries [1,2]. The associated metabolic syndrome (MS) is also showing an increasing trend [1–3]. Although prevalence rates of MS differ due to diverse criteria applied for its diagnosis, but range between 2.3% and 35.2% in developing countries [1]. The obesity related MS is known to be associated with a low grade systemic inflammation [4–6]. Of the many markers used to detect this inflammatory state in obesity, C-reactive protein (CRP) has emerged as the analyte of choice [7]. High CRP levels have consistently been demonstrated as childhood predictors of adult MS amongst other predictors [8,9]. High CRP levels also correlate well with other parameters of MS [10]. Majority of the previous studies showing raised CRP levels in obese children are from the developed countries [4–9,11–14]. The need to generate data from the developing countries is even more in view of the recent observations and recommendations for diagnosis of obesity and MS for Asian Indians [15]. The addition of CRP to standard cholesterol evaluation may also provide a simple and inexpensive method to improve risk prediction and compliance with preventive approaches.
Aim
The present study was thus conducted with an aim to see the relationship of high sensitivity CRP (hsCRP) levels with various anthropometric as well as metabolic parameters in children with simple obesity.
Materials and Methods
One hundred children (60 boys and 40 girls) with simple overweight (BMI between 85th and 95th percentiles according to age & gender specific CDC 2000 growth charts) and obesity (BMI >95th percentile) and aged between 6 and 16 years were enrolled into the study [16]. Those having an acute infection, secondary obesity, known primary hyperlipidemias, diabetes or hypertension, hereditary or systemic inflammatory diseases, on any regular medications or significant physical training program were excluded. One hundred (56 boys and 44 girls) age matched non-obese (BMI between 25th & 75th percentiles according to age and gender specific CDC 2000 growth charts) children were taken as controls. The obese subjects were recruited from the Pediatric Endocrinology clinic of the hospital and controls were recruited from a nearby government run school. The study was approved by the Institute’s Ethics Committee. Written informed consent from parents and assent from the participating children was obtained.
Clinical Assessment
A thorough physical examination was done in all subjects to exclude any significant systemic illness. Blood pressure was measured with a mercury sphygmomanometer after 20min of rest in supine position. Weight was measured on electronic weighing machine (Avery, India) to the nearest 50g with children barefoot and wearing light clothing. Height was measured with a stadiometer to the nearest 1mm. BMI was calculated as the ratio of body weight to body height squared and expressed as Kg/m2. Waist and hip circumference was measured to the nearest 0.1cm by using standardized anthropometric techniques. Waist to hip ratio (WHR) was calculated.
Laboratory Assessment
Blood glucose and lipid profile (TC; HDL-C; VLDL-C; TG) were done by clinical chemistry automatic analyser (Dade Behring). Concentration of LDL-C was calculated using Friedwald formula as LDL C=TC– HDL–(TG/5). Atherogenic index was calculated as ratio of LDL– C/HDL– C. Measurement of hsCRP was done by the method based on particle enhanced turbidimetric immunoassay (PETIA) technique (Flex Reagent cartridge, Dimension clinical chemistry system, Dade Behring Ltd, UK) [17]. In this method, latex particles coated with antibody to CRP aggregate in presence of CRP in sample and increase turbidity proportional to CRP concentration which is then determined by a mathematical function. The analytical sensitivity of this method is 0.5 mg/L.
Statistical Analysis
Comparison between groups was done for various categorical variables using Chi-square test. The mean values of age, anthropometry and quantitative biochemical variables were compared using independent t-test. Pearson’s correlation coefficients were calculated between different quantitative variables. Multivariate linear and logistic analysis was carried out to find significant predictors for the outcome of hs-CRP after adjusting for various confounding variables. A p-value (two-tailed) <0.05 was taken as significant.
Results
The study cohort comprised of 116 (58%) boys and 84 (42%) girls. The anthropometric characteristics and blood pressure were significantly different in the 2 groups [Table/Fig-1]. Within group comparison of these parameters did not show any differences between boys and girls.
Baseline characteristics of the 2 groups
| Parameter | Study group (Mean±SD) | Control group (Mean±SD) | p-value |
|---|
| Age (yrs) | 11.5±2.28 | 11.7±0.73 | 0.404 |
| BMI (kg/m2) | 24.5±2.85 | 17.5±1.65 | <0.001 |
| WC (cms) | 77.7±9.20 | 60.5±4.52 | <0.001 |
| HC (cms) | 86.8±8.67 | 78.7±5.58 | <0.001 |
| WHR | 0.89±.079 | 0.76±.047 | <0.001 |
| SBP | 116.2±9.72 | 109.1±8.03 | <0.001 |
| DBP | 72.2±8.33 | 68.9±6.97 | 0.003 |
Abbreviations: BMI, body mass index; WC, waist circumference; HC, hip circumference; WHR, waist hip ratio; SBP, systolic blood pressure; DBP, diastolic blood pressure
Biochemical Parameters
Mean values of all the biochemical parameters except HDL-C were significantly higher in the study group [Table/Fig-2].
Comparison of biochemical parameters among two groups
| Parameter | Study group (Mean±SD) | Control group (Mean±SD) | p-value |
|---|
| TC (mg/dL) | 157.9±32.39 | 144.4±22.09 | 0.001 |
| HDL-C (mg/dL) | 36.4±8.26 | 39.3±6.27 | 0.005 |
| LDL-C (mg/dL) | 95.4±26.77 | 88.3±18.45 | 0.032 |
| AI | 2.62±0.91 | 2.26±0.45 | 0.002 |
| FBG (mg/dL) | 89.8±9.86 | 81.6±8.71 | <0.001 |
| hs-CRP (mg/L) | 3.92±2.20 | 2.15±1.05 | <0.001 |
Abbreviations: TC, total cholesterol; HDL-C, high density lipoprotein-cholesterol; LDL-C, low density lipoprotein cholesterol; AI, atherogenic index; FBG, fasting blood glucose
Subjects were divided into three subcategories based on their hsCRP levels (<1, 1-3 and >3 mg/L) and comparison was done among two groups. Significantly more (58% versus 10%) subjects in the study group had hsCRP levels of >3 mg/L [Table/Fig-3].
Distribution of hs-CRP among three subcategories
| hs-CRP levels | <1 mg/L | 1-3 mg/L | >3 mg/L |
|---|
| Study group | 2 | 40 | 58 |
| Control group | 2 | 88 | 10 |
Correlation between hsCRP and other parameters
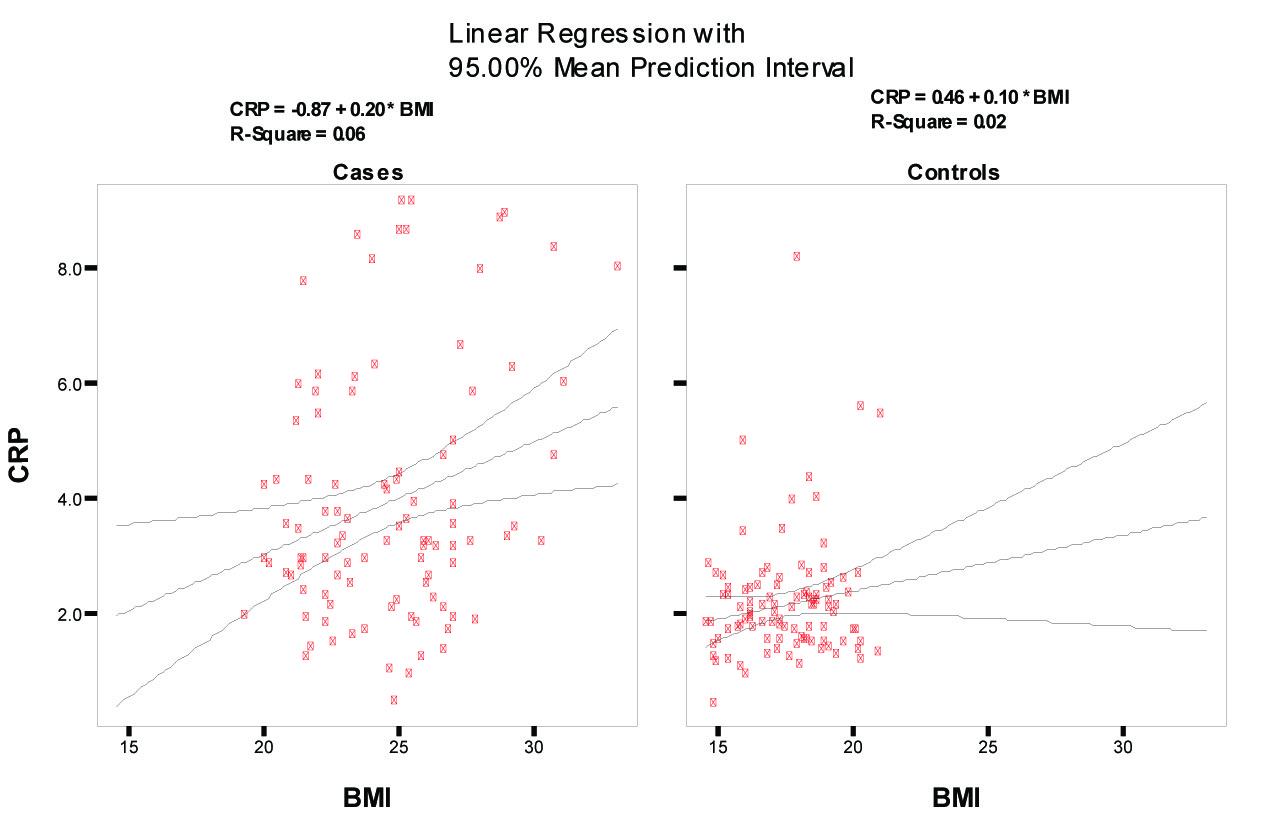
In the study group, BMI showed a positive correlation with hs-CRP levels while no correlation was observed between hsCRP and other parameters of obesity in control group. The scatter diagram shows comparative linear correlation between BMI and CRP for the two groups [Table/Fig-4]. Though both regression lines are positively correlated, the relationship was statistically significant for cases only. However, R-square (coefficient of determination) is 0.06; that is only 6% of variability in CRP levels could be explained by BMI in cases. In the Multiple logistic regression analysis only BMI showed independent predictive ability for hsCRP (>3 mg/L). With every 1 kg/m2 increase in BMI, odds of high hsCRP level were increased by 37% (multivariate OR 1.37, 95% CI 1.23-1.53, p-value <0.0001).
correlation between BMI and hsCRP among two groups
Correlation analysis between CRP and other Parameters for study group
| Pearson correlation coefficient | p value |
|---|
| Age (years) | -0.001 | 0.995 |
| BMI (kg/m2) | 0.253 | 0.011 |
| WHR | 0.134 | 0.185 |
| SBP | 0.029 | 0.774 |
| DBP | -0.043 | 0.669 |
| TC (mg/dl) | 0.170 | 0.090 |
| HDL-C (mg/dl) | 0.214 | 0.06 |
| LDL-C (mg/dl) | 0.115 | 0.256 |
| LDL-C/HDL-C | -0.067 | 0.509 |
| FBS (mg/dl) | 0.153 | 0.129 |
Discussion
Obesity related metabolic syndrome is associated with increase in the levels of a number of markers of inflammation especially CRP [4–6]. This subclinical or low grade inflammatory state in simple obesity is associated with increased risk for cardiovascular disease and diabetes [8–10]. Detection of this systemic inflammation may help to identify children and adolescents at high risk for developing cardiovascular disease and diabetes as adults. A recent study indicates that the inflammatory state reflected in the increase in hsCRP levels is present even during early stages of accumulation of weight towards obesity [18].
Overweight and obese children in our study had significantly higher hs-CRP levels indicating presence of inflammatory state in the study group. Previous studies have shown similar results in young overweight and obese individuals [7,8,11–14,18]. However, the values of hs-CRP obtained in our study are higher as compared to some previous observations [11]. In the study by Hiura et al., mean CRP values were 0.33 and 1.20 mg/L in non-obese and obese groups respectively; this may be due to exclusion of children with high hs-CRP values in the obese group assuming the possibility of acute infection. As many as 23 out of 109 obese children were excluded in that study because of hsCRP values of > 3 mg/L [11]. The authors of the study did discuss the possibility that hsCRP elevation was not necessarily due to acute infection in obese children who were excluded [11]. The hsCRP levels in our study were also higher as compared to those found in a similar study from South India [19]. Although, it was not mentioned if exclusion criteria similar to the study by Hiura et al., were applied, the authors of the Indian study did acknowledge the limitation of a small sample size [19]. Since all our children were thoroughly examined to rule out any recent infection or other inflammatory states, the high levels of hsCRP obtained were probably a reflection of presence of subclinical inflammation in these patients. A strong positive correlation was observed between BMI and hsCRP levels in obese children but same degree of correlation was not seen between WHR and hsCRP although subjects with lower WHR had lower hsCRP levels. Earlier studies also have shown similar positive correlation between BMI, waist circumference (WC) and CRP [20]. Although, obese children had significant differences in lipid levels as compared to controls, the correlation between hsCRP and parameters of lipid profile was not significant. The atherogenic index, an expression of impaired lipid metabolism in obesity, was altered in the study group, an observation made in earlier studies also [11]. Atherogenic dyslipidemia is considered as an important cardiovascular disease risk factor in obese patients [21]. Similarly FBS was also higher in the overweight/obese group although no subject fulfilled criteria for diagnosis of diabetes. Similar observations have been made in different studies in children and indicate the presence of risk factors for metabolic syndrome in obese children [19,22].
The mean systolic and diastolic blood pressures differed significantly amongst the two study groups although none of the subjects were actually hypertensive. These results are consistent with some previous studies [10,11]. Our observation adds to the hypothesis that inflammatory state that occurs in obesity may contribute to elevation of blood pressure [23]. Elevated blood pressure and in particular the pulse pressure has been associated with an increased risk of cardiovascular disease and the underlying mechanism may be inflammation as demonstrated by elevated CRP levels [24]. Hypertension may also increase cardiovascular risk by causing chronic endothelial injury promoting structural and functional vascular alterations, especially in the microvascular network [25]. The higher values of hsCRP as compared to previous studies [11] as well as the alterations in blood pressure, lipids and blood glucose in our study may indicate the enhanced cardiovascular risk in Indian children with simple obesity particularly in view of the recent recommendations for diagnosis of obesity and MS for Asian Indians [15].
Conclusion
Children with overweight and obesity have increased hsCRP levels that may indicate a low grade systemic inflammation in these children. Additionally, they have elevations of blood pressure, FBG and lipids.
Abbreviations: BMI, body mass index; WC, waist circumference; HC, hip circumference; WHR, waist hip ratio; SBP, systolic blood pressure; DBP, diastolic blood pressure
Abbreviations: TC, total cholesterol; HDL-C, high density lipoprotein-cholesterol; LDL-C, low density lipoprotein cholesterol; AI, atherogenic index; FBG, fasting blood glucose
[1]. Misra A, Khurana L, Obesity and metabolic syndrome in developing countriesJ Clin Endocrinol Metab 2008 93:S9-30. [Google Scholar]
[2]. Ramachandran A, Snehalatha C, Rising Burden of Obesity in AsiaJournal of Obesity 2010 2010Article ID 868573, 8 pages. doi:10.1155/2010/868573 [Google Scholar]
[3]. Ganie MA, Metabolic syndrome in Indian children – An alarming riseIndian J Endocrinol Metab 2010 14:1-2. [Google Scholar]
[4]. Tamakoshi K, Yatsuya H, Kondo T, Hori Y, Ishikawa M, Zhang H, The metabolic syndrome is associated with elevated circulating C-reactive protein in healthy reference range, a systemic low-grade inflammatory stateInt J Obes Relat Metab Disord 2003 27:443-49. [Google Scholar]
[5]. Valle M, Martos R, Gascon F, Canete R, Zafra MA, Morales R, Low-grade systemic inflammation, hypoadiponectinemia and a high concentration of leptin are present in very young obese children and correlate with metabolic syndromeDiab Metab 2005 31:55-62. [Google Scholar]
[6]. Shin JY, Kim SY, Jeung MJ, Eun SH, Woo CW, Yoon SY, Serum adiponectin, C-reactive protein and TNF-alpha levels in obese Korean childrenJ Pediatr Endocrinol Metab 2008 21:23-29. [Google Scholar]
[7]. Pearson TA, Mensah GA, Alexander RW, Anderson JL, Cannon RO 3rd, Criqui M, Markers of inflammation and cardiovascular disease: Application to clinical and public health practice: A statement for healthcare professionals from the Centers for Disease Control and Prevention and the American Heart AssociationCirculation 2003 107:499-511. [Google Scholar]
[8]. Mattsson N, Rönnemaa T, Juonala M, Viikari JS, Raitakari OT, Childhood predictors of the metabolic syndrome in adulthood. The Cardiovascular Risk in Young Finns StudyAnn Med 2008 40:542-52. [Google Scholar]
[9]. Soriano-Guillén L, Hernández-García B, Pita J, Domínguez-Garrido N, Del Río-Camacho G, Rovira A, High-sensitivity C-reactive protein is a good marker of cardiovascular risk in obese children and adolescentsEur J Endocrinol 2008 159:R1-4. [Google Scholar]
[10]. López-Jaramillo P, Herrera E, Garcia RG, Camacho PA, Castillo VR, Inter-relationships between body mass index, C-reactive protein and blood pressure in a Hispanic pediatric populationAm J Hypertens 2008 21:527-32. [Google Scholar]
[11]. Hiura M, Kikuchi T, Nagasaki K, Uchiyama M, Elevation of serum C-reactive protein levels is associated with obesity in boysHypertens Res 2003 26:541-46. [Google Scholar]
[12]. Ford ES, Ajani UA, Mokdad AH, The metabolic syndrome and concentrations of C-reactive protein among U.S. youthDiabetes Care 2005 28:878-81. [Google Scholar]
[13]. Guran O, Akalin F, Ayabakan C, Dereli FY, Haklar G, High-sensitivity C-reactive protein in children at risk for coronary artery diseaseActa Paediatr 2007 96:1214-19. [Google Scholar]
[14]. Roh EJ, Lim JW, Ko KO, Cheon EJ, A useful predictor of early atherosclerosis in obese children: serum high-sensitivity C-reactive proteinJ Korean Med Sci 2007 22:192-97. [Google Scholar]
[15]. Misra A, Chowbey P, Makkar BM, Vikram NK, Wasir JS, Chada D, Consensus statement for diagnosis of obesity, abdominal obesity and metabolic syndrome for Asian Indians and recommendations for physical activity, medical and surgical managementJ Assoc Physicians India 2009 57:163-70. [Google Scholar]
[16]. Kuczmarski RJ, Ogden CL, Grummer-Strawn LM, Flegal KM, Guo SS, Wei R, CDC growth charts: United StatesAdv Data 2000 314:1-27. [Google Scholar]
[17]. Teitz NW, Textbook of Clinical Chemistry 1999 Philadelphia, PAW.B. Saunders Co:42-72. [Google Scholar]
[18]. Kitsios K, Papadopoulou M, Kosta K, Kadoglou N, Papagianni M, Tsiroukidou K, High-Sensitivity C-Reactive Protein Levels and Metabolic Disorders in Obese and Overweight Children and AdolescentsJ Clin Res Pediatr Endocrinol 2013 5:44-49. [Google Scholar]
[19]. Namburi RP, Ponnala AR, Karthik TS, Rani PR, Maheshwari R, A study on metabolic variables and its association with high sensitive C-reactive protein in obese children and adolescentsIndian J Endocrinol Metab 2013 17(1):S360-62. [Google Scholar]
[20]. Steene-Johannessen J, Kolle E, Reseland JE, Anderssen SA, Andersen LB, Waist circumference is related to low-grade inflammation in youthInt J Pediatr Obes 2010 5:313-19. [Google Scholar]
[21]. Musunuru K, Atherogenic dyslipidemia: Cardiovascular risk and dietary interventionLipids 2010 45:907-14. [Google Scholar]
[22]. Beauloye V, Zech F, Tran HT, Clapuyt P, Maes M, Brichard SM, Determinants of early atherosclerosis in obese children and adolescentsJ Clin Endocrinol Metab 2007 92:3025-32. [Google Scholar]
[23]. Jarvisalo MJ, Harmoinen A, Hakanen M, Paakkunainen U, Viikari J, Hartiala J, Elevated serum C-reactive protein levels and early arterial changes in healthy childrenArterioscler Thromb Vasc Biol 2002 22:1323-28. [Google Scholar]
[24]. Abramson JL, Weintraub WS, Vaccarino V, Association between pulse pressure and C-reactive protein among apparently healthy US adultsHypertension 2002 39:197-202. [Google Scholar]
[25]. Yannoutsos A, Levy BI, Safar ME, Slama G, Blacher J, Pathophysiology of hypertension: interactions between macro and microvascular alterations through endothelial dysfunctionJ Hypertens 2014 32:216-24. [Google Scholar]