Epilepsy refers to a disorder of brain characterised by the periodic and unpredictable occurrence of seizure. The term ‘Seizure’ refers to a transient alteration of behaviour due to the disordered, synchronous, and rhythmic firing of populations of brain neuron [1]. The episodes of seizures are unpredictable and their frequency is highly variable.
As per WHO, epilepsy is one of the most common serious brain disorder that affects not only the individual, but also disturbs the family and the society in general. WHO estimates that 8 per 1000 population worldwide have epilepsy, with higher prevalence in developing countries as compared to developed countries. Further, there are approximately 10 million people estimated to be with epilepsy in India accounting for 1/5th of the global burden [2].
Epilepsy occurs in men and women and can begin at any age, but is most frequently diagnosed in early life or in old age. Up to 5% of the world’s population may have a single seizure at some time in their lives, but a diagnosis of epilepsy is reserved for those who have recurring seizures, i.e. at least two unprovoked seizures.
The anticonvulsants also commonly known as antiepileptic drugs are a diverse group of pharmaceuticals used in the treatment of epileptic seizures. The goal of an anticonvulsant is to suppress the rapid and excessive firing of neurons that start a seizure. Treatment of epilepsy is often a lifelong affair.
Several studies have reported that commonly used antiepileptic drugs like phenytoin, phenobarbital and carbamazepine, increase serum HDL-C levels, while some others documented no such effect. Further, some researchers also observed that valproic acid and other newer antiepileptic drugs like lamotrigine and levetiracetam has no influence on serum lipid profile [3].
Serum concentration of certain lipids and lipoproteins in young adults are important risk factors for the development of coronary heart disease in later life. Considerable data has suggested that besides total cholesterol (TC), elevated triglyceride (TG) concentrations, increased LDL-C and decreased HDL-C contribute to cardiovascular diseases. Thus, assessing changes in serum lipid levels following antiepileptic drugs may be useful to choose the safest drug and prevention of cardiovascular complications in later life [4].
The effect of antiepileptic drugs on serum lipid levels had already been documented in western literature. However, information in this regard is scarce from India.
So, the present study was planned to find and compare the effect of conventional and newer antiepileptic drugs on lipid profile of epileptic patients.
To evaluate effect of antiepileptic drugs on serum lipid profile among young adults with epilepsy in a tertiary care hospital in Pondicherry.
Materials and Methods
A prospective hospital based cross-sectional study was conducted in a tertiary care hospital. This study was carried around a semi-urban population between months May-June 2013 (two months).
In view of study duration (two months) and considering number of epileptic patients attending Department of Neurology and taking antiepileptic drugs for last six months or more and on regular follow up; approximately 60 patients on commonly used antiepileptic drugs (20 on phenytoin, 20 on oxcarbazepine, 20 on valproic Acid) and 20 patients on newer antiepileptic drug (levetiracetam) was included in the study. Age and sex matching 80 controls were taken.
Ethical Permission
Ethical permission to conduct the hospital based study was obtained from Institution Ethical Committee before commencement of study. Confidentiality was maintained throughout the study period.
Inclusion criteria
Young adult patients between 20 to 40 years of age (both sex),
Visiting Department of Neurology of the tertiary care hospital during May-June 2013,
Taking antiepileptic drugs for last 6 months or more and.
Willing to participate and giving informed written consent.
Exclusion criteria
Patients with secondary epilepsy,
Patients with other neurological or psychiatric disorder,
Patients with other genetic or medical disorder,
Pregnant females on antiepileptic drugs,
Patients with serious illness, malignancy or other complications,
Patients taking hypolipidaemic drugs and
Patients on more than one antiepileptic drug.
Selection of controls
Relatives of study subjects between 20 to 40 years age (both sex),
Accompanying study subjects to Department of Neurology during the study period,
Without any other medical, genetic or psychiatric disorder,
Not on any hypolipidaemic drugs,
Willing to participate and giving informed written consent.
Specimen Collection
Blood sample was collected both from study subjects and controls. 5ml of venous blood was collected by trained lab technician under sterile conditions using a disposable syringe between 8.00 to 10.00 a.m. after overnight fasting and the sample was tested for TC, HDL-C, LDL-C and TG. The blood was allowed to clot in a plain bulb at room temperature, and the serum was separated by centrifugation at 3000rpm for 10min. It was then kept frozen at -20°C to be analysed later on.
TC was calculated by enzymatic method and expressed in mg/dl. HDL-C was calculated using polyanion precipitation and expressed as mg/dl. LDL-C was calculated using Friedewald’s equation and expressed in mg/dl. Triacylglycerol (TAG) in serum was converted to glycerol and then estimated using glycerol kinase enzyme based kinetic method and expressed in mg/dl. LDL-C/HDL-C ratio was also calculated.
Data Collection Procedure
Laboratory reports of all study subjects and controls were collected by investigator student from the Central Investigation Laboratory of tertiary care hospital. Information regarding patients’ age, sex, diagnosis, treatment duration, medication history, TC, LDL-C, HDL-C, TG levels were collected.
Statistical Analysis
Collected data was entered in Microsoft_Office_Excel 2010 and analysed using SPSS. Inc statistical software version 17.0. Descriptive statistics explained using mean ± SD. Inferential statistics was used depending on the nature of variables. We used one way ANOVA and followed by independent t-test for comparison with control group and statistically significant was considered at P-value <0.05.
Results
There were 20 patients each in phenytoin, carbamazepine, valproic acid and levetiracetam group. For each group 20 controls were taken so total numbers of controls were 80.
We observed statistically significant high mean TC, HDL-C, LDL-C and TG levels in the group receiving phenytoin for more than six months when compared with control group. The mean TC, HDL-C, LDL-C and TG levels were 186.5 ± 7.87 mg/dl, 71.1 ± 3.14 mg/dl, 88.25 ± 7.49 mg/dl and 133.7 ± 4.50 mg/dl respectively [Table/Fig-1].
TC, HDL-C, LDL, TG levels in patients receiving phenytoin for more than 6 months
| Lipid Profile Parameter | Group | Mean ± Sth. Deviation | p-value |
|---|
| TC (mg/dl) | Control | 171.9 ± 8.60 | 0.0001† |
| Phenytoin | 186.5 ± 7.87 |
| HDL-C (mg/dl) | Control | 63.9 ± 3.16 | 0.0001† |
| Phenytoin | 71.1 ± 3.14 |
| LDL-C (mg/dl) | Control | 82.75 ± 7.85 | 0.029† |
| Phenytoin | 88.25 ± 7.49 |
| TG (mg/dl) | Control | 126.7 ± 4.50 | 0.0001† |
| Phenytoin | 133.7 ±4.50 |
* Significant level with p<0.05 † Highly Significant level with p<0.01
We observed statistically significant high mean TC, HDL-C and TG levels in the group receiving oxcarbazepine for more than six month when compared with control. However, no significant difference was observed in mean LDL-C levels when compared to control. The mean TC, HDL-C, LDL-C and TG levels were 179.0 ± 8.79 mg/dl, 67.10 ± 3.40 mg/dl, 86.40 ± 7.32 mg/dl and 129.70 ± 4.51 mg/dl respectively [Table/Fig-2].
TC, HDL-C, LDL, TG levels in patients receiving oxcarbazepine for more than 6 months
| Lipid Profile Parameter | Group | Mean ± Std. Deviation | p-value |
|---|
| TC | Control | 171.90 ± 8.61 | 0.013* |
| Oxcarbazepine | 179.05 ± 8.79 |
| HDL | Control | 63.90 ± 3.16 | 0.004† |
| Oxcarbazepine | 67.10 ± 3.40 |
| LDL | Control | 82.75 ± 7.85 | 0.137 |
| Oxcarbazepine | 86.40 ± 7.32 |
| TG | Control | 126.70 ± 4.51 | 0.042* |
| Oxcarbazepine | 129.70 ± 4.51 |
*Significant level with p<0.05 †Highly Significant level with p<0.01
We did not observe any statistically significant difference among mean TC, HDL-C, LDL-C and TG levels in the group receiving valproate for more than six months when compared with control group [Table/Fig-3].
TC, HDL-C, LDL, TG levels in patients receiving valproate for more than 6 months
| Lipid Profile Parameter | Group | Mean ± Std. Deviation | p-value |
|---|
| TC | Control | 171.90 ± 8.61 | 0.053 |
| Valproate | 173.90 ± 8.50 |
| HDL | Control | 63.90 ± 3.16 | 0.057 |
| Valproate | 62.95 ± 2.87 |
| LDL | Control | 82.75 ± 7.85 | 0.137 |
| Valproate | 83.55 ± 7.39 |
| TAG | Control | 126.70 ± 4.51 | 0.042 |
| 128.55 ±5.31 |
*Significant level with p<0.05 †Highly Significant level with p<0.01
We did not observe any statistically significant difference among mean TC, HDL-C, LDL-C and TG levels in the group receiving levetiracetam for more than six months when compared with control group [Table/Fig-4].
TC, HDL-C, LDL, TG levels in patients receiving levetiracetam for more than 6 months
| Lipid Profile Parameter | Group | Mean ± Std. Deviation | p-value |
|---|
| TC | Control | 171.90 ± 8.60 | 0.715 |
| Levetiracetam | 170.90 ± 8.41 |
| HDL | Control | 63.90 ± 3.16 | 0.053 |
| Levetiracetam | 65.90 ± 3.16 |
| LDL | Control | 82.75 ± 7.85 | 0.716 |
| Levetiracetam | 81.85 ± 7.66 |
| TAG | Control | 126.70 ± 4.51 | 1.000 |
| 125.80 ± 4.78 |
* Significant level with p<0.05 † Highly Significant level with p<0.01
We observed statistically significant increase in mean TC levels in groups which received phenytoin and oxcarbazepine when compared with control. High mean TC levels were found in phenytoin followed by oxcarbazepine. Mean TC levels among patients receiving phenytoin and oxcarbazepine were 186.5 ± 7.87 mg/dl and 179.05 ± 8.79 mg/dl respectively [Table/Fig-5].
Comparison of mean TC levels in patient receiving phenytoin, oxcarbazepine, valproic acid and levetiracetam with control

We observed statistically significant increase in mean HDL-C levels in groups which received phenytoin and oxcarbazepine when compared with control. High mean HDL-C levels were found in phenytoin followed by oxcarbazepine. Mean HDL-C levels among patients receiving phenytoin and oxcarbazepine were 71.1 ± 3.14 mg/dl and 67.10 ± 3.40 mg/dl respectively [Table/Fig-6].
Comparison of mean HDL-C levels in patient receiving phenytoin, oxcarbazepine, valproic acid and levetiracetam with control

We observed statistically significant increase in mean LDL-C levels in group receiving phenytoin when compared with control. Mean LDL-C levels among patients receiving phenytoin was 88.25 ± 7.49 mg/dl [Table/Fig-7].
Comparison of mean LDL-C levels in patient receiving phenytoin, oxcarbazepine, valproic acid and levetiracetam with control

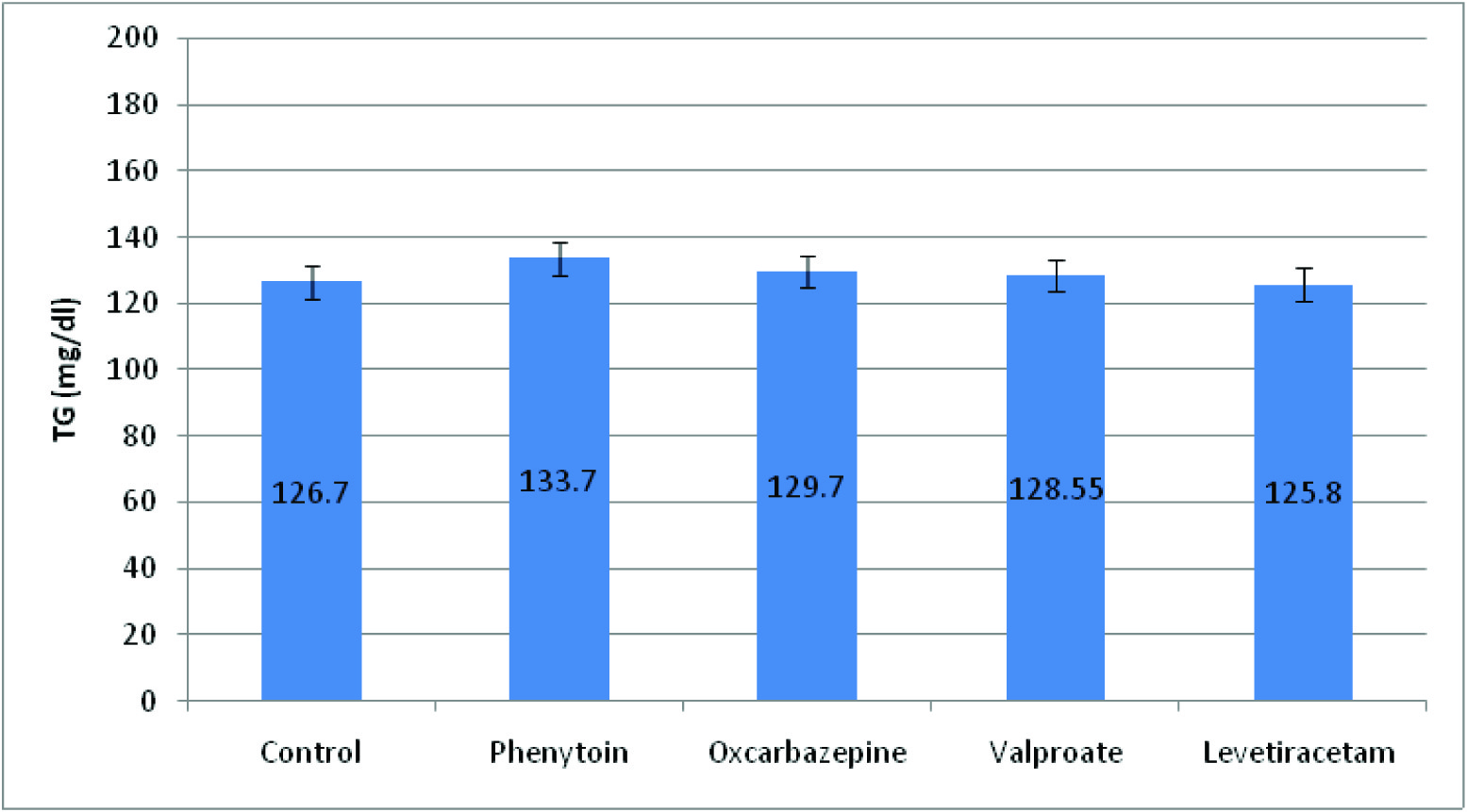
We observe statistically significant increase in mean TG levels in groups which received phenytoin and oxcarbazepine when compared with control. High mean TG levels were found in phenytoin followed by oxcarbazepine. Mean TG levels among patients receiving phenytoin and oxcarbazepine were 133.7 ± 4.50 mg/dl and 129.70 ± 4.51 mg/dl respectively [Table/Fig-8].
Comparison of mean TG levels in patient receiving Phenytoin, Oxcarbazepine, Valproic acid and Levetiracetam with control
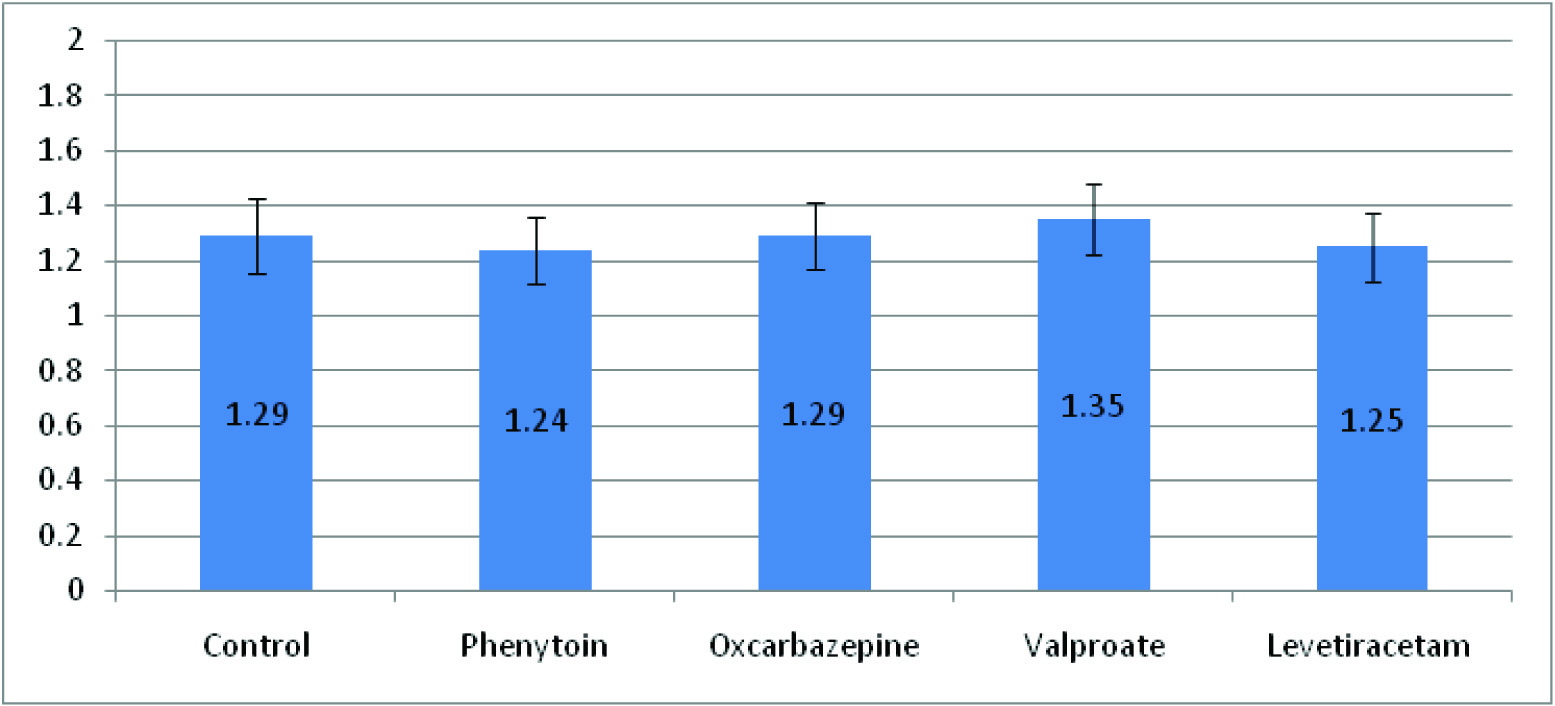
We did not observe statistical significance in any of the groups when compared with their mean LDL-C/HDL-C ratio with control-group [Table/Fig-9].
Comparison of mean LDL-C/HDL-C ratio in patient receiving Phenytoin, Oxcarbazepine, Valproic acid and Levetiracetam with control
Discussion
The present study was designed to investigate the effect of conventional and newer antiepileptic drugs on lipid profile parameters such as TC, HDL-L, LDL-C and TAG.
We observed significant increase in mean TC, HDL-C, LDL-C and TG levels when compared with the control in patients receiving phenytoin sodium for six or more months. The results in our study findings are similar to those other investigations done by P Kumar et al., Pelkonen et al., Nikkila et al., and Luoma et al., also reported same findings i.e. an increase in TG, LDL-C and HDL-C levels in epileptic patients on long-term treatment with Phenytoin [5–8]. Study results conducted by Calandre et al., and Dewan P et al., observed higher HDL-C and TC levels but no effect on LDL-C levels in epileptic patients on long-term treatment with phenytoin [9,10].
In addition, we have found similar effect for oxcarbazepine on mean TC, HDL-C and TG levels. These findings are largely consistent with and significantly extend those of other investigations. Studies of carbamazepine treated patients have mostly demonstrated increased TC levels compared with a control group, with most also showing increased LDL-C and HDL-C in this population [11–15]. However, in our study we did not observe any statistically significant difference among mean LDL-C levels which is similar to study conducted by Yi U et al., [16].
The effect of phenytoin and carbamazepine may be due to the induction of CYP enzyme. They are the inducers of CYP51 enzyme. CYP51 is a housekeeping gene of the cytochrome P450 super family which is involved in cholesterol biosynthesis in humans. The CYP450 enzyme system is involved in the synthesis and metabolism of cholesterol [17]. In particular; CYP51A1 plays a key role in cholesterol synthesis [18]. Also, carbamazepine stimulates the hepatic synthesis of cholesterols and increase the formation and pool size of bile acids, which in turn raise the level of intestinal absorption of cholesterol by facilitating micelle formation [18].
In our study oxcarbazepine is used by the neurologist may be due to the advantages such as less drug interactions, least toxic. Also, it is a weak enzyme inducer; this may be the reason why the level of LDL-C was not statistically different from control.
The patients who were on valproate and levetiracetam showed no significant change in TC, HDL-C, LDL-C and TG levels when compared with control. Study done by Mohamed Kantoush et al., 1998 showed decreased levels of LDL and TG on valproic acid which are contrasting our study results [19]. But changes investigated by E Yilmaz et al., and recent study by Erdemir A et al., and Uma Bhosale et al., showed the similar effect of valproate on serum lipid profile [4,20,21].
Our study finding was also similar to a recent study done by Mintzer et al., where they observed that when epileptic patients on inducing agents like carbamazepine and phenytoin switch to the non-inducing AEDs lamotrigine and levetiracetam, demonstrated a decline in total cholesterol [22].
There is no information available about the relationship between lipid function and levetiracetam. However, no significant effects on lipid metabolism by both levetiracetam and valproic acid suggest that both are non inducer of CYP51 enzyme.
Based on cardiovascular epidemiological literature, an increase in serum cholesterol particularly high levels of LDL-C may be regarded as an adverse effect on long-term anticonvulsant treatment as it increases the risk of coronary heart disease [23]. However, some epidemiologic studies have also demonstrated that mortality due to atherosclerosis- related heart disease is lower among patients with epilepsy treated with enzyme inducer AEDs than in the general population. This may be due to complex action i.e. increase in HDL-C (positive cardiovascular effect), TC and LDL-C (negative cardiovascular effect) levels associated with phenytoin and oxcarbamazepine [24].
Limitation
Thus, assessing changes in serum lipid levels following antiepileptic drugs may be useful to choose the safest drug and prevention of cardiovascular complications in later life.
There are some limitations of our study such as it was conducted in a particular area and sample size was also small. Hence, for a better understanding a detailed prospective clinical study on serial monitoring of changes in serum lipid levels from the beginning of the antiepileptic therapy to completion of therapy and beyond has to be instituted to augment our claim.
Conclusion
From the present study we can conclude that CYP enzyme inducer anti epileptic medicines like phenytoin and oxcarbazepine is strongly associated with increased levels of TC, LDL-C, HDL-C and TG where as valproate and levetiracetam showed no significant change. Therefore, the serum cholesterol level should be regularly monitored in patients undergoing therapy with inducer anti epileptic medicines.
* Significant level with p<0.05 † Highly Significant level with p<0.01
*Significant level with p<0.05 †Highly Significant level with p<0.01
*Significant level with p<0.05 †Highly Significant level with p<0.01
* Significant level with p<0.05 † Highly Significant level with p<0.01