Spontaneous Expulsion of Foreign Body (Seewing Machine Needle) From Right Middle Lobe Bronchus - A Rare Case Report
Ashwin Ashok Jaiswal1, Amrish Kumar Garg2
1 Senior Medical Officer, Department of ENT & Head Neck Surgery, J.L.N. Hospital & Research Centre, Bhilai, Chhattisgarh, India.
2 Joint Director & Head of Department, Department of ENT & Head Neck Surgery, J.L.N.Hospital & Research Centre, Bhilai, Chhattisgarh, India.
NAME, ADDRESS, E-MAIL ID OF THE CORRESPONDING AUTHOR: Dr. Ashwin Ashok Jaiswal, MBBS, DLO, DNB (ENT), SR. Medical Officer, Department of ENT & Head Neck Surgery, J.L.N. Hospital & Research Centre, Sector 9, Bhilai, Dist. Durg, Chhattisgarh-490009, India.
Phone: 9407983605
E-mail: ash1978jaiswal@gmail.com
Aspirated foreign bodies continue to present challenges to the Otorhinolaryngologists. The major issues involve the accurate diagnosis at the earliest and speedy, safe removal of the foreign body. Endoscopic removal is the mainstay of management of foreign body in tracheobronchial tree. Spontaneous expulsion of foreign body bronchus is a rare entity with few cases reported in literature. We report a rare and interesting case of 18-year-old male patient presented with sharp and pointed metallic foreign body in Right Middle lobe Bronchus i.e., sewing machine needle. Patient was admitted and planned for bronchoscopy. But prior to it, foreign body was spontaneously expelled out. The patient was discharged next day without any complication. Spontaneous expulsion saves the patient from the dangers of endoscopic removal of foreign body, but impose a great danger of subglottic lodgement of foreign body.
Bronchoscopy, Foreign body bronchus, Otorhinolaryngologists, Tracheobronchial tree
Case Report
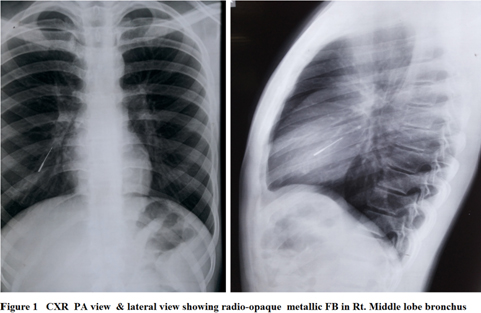
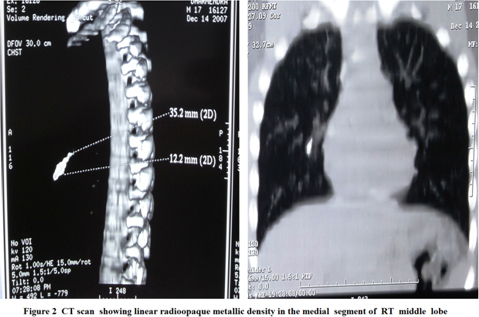
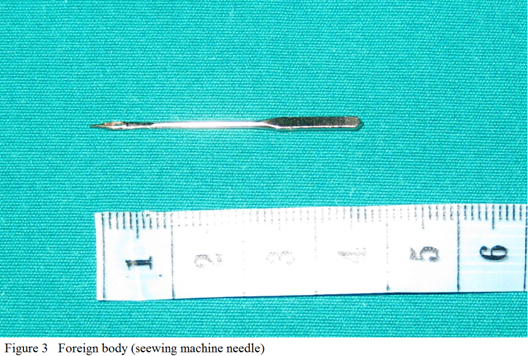
A 18-year-old male patient, Tailor by occupation, presented to our hospital with a history of accidental inhalation of a sewing machine needle while trying to hold it in between teeth during changing it from sewing machine. Immediately the patient had bouts of coughing followed by right-sided and retrosternal chest pain which was relieved almost instantly. There was no associated dyspnoea, hemoptysis or abdominal pain. He was fully conscious, alert and cooperative on arrival to ENT OPD on the next day. Patient complained of intermittent bouts of cough on & off. Physical examination showed no abnormality. Chest roentegenogram demonstrated a radioopaque sharp pointed foreign body, lodged in the right bronchus [Table/Fig-1]. This was confirmed by CT scan which revealed a linear radioopaque metallic density in bronchus of medial segment of Rt. Middle lobe [Table/Fig-2]. It was decided that bronchoscopic removal would be attempted; in case it fails surgical removal would be adopted. During the preoperative preparation on the day of planned bronchoscopy , when the patient turned on his left side, he had continuous bouts of cough and expectorated the foreign body spontaneously. The foreign body was 3.5 cm in length [Table/Fig-3].There was no postexpectoration dyspnoea, hemoptysis or chest pain. He was kept for 24h under observation. Repeated chest roentegnogram was normal and he was discharged on next day.
CXR PA view and lateral view showing radioopaque metallic F.B.in right middle lobe bronchus
CT scan thorax showing linear radio-opaque metallic density in medial segment of right middle lobe
Foreign body (Seewing machine Needle)
Discussion
A foreign body inhalation in the tracheobronchial tree is a dangerous & common medical emergency with serious and potentially lethal consequences [1]. The larynx performs a very efficient sphincteric function to protect the lower respiratory tract and, therefore, it is unusual for a foreign body to be inhaled rather than swallowed [2]. In 1921, Jackson suggested that spontaneous expulsion of intrapulmonary foreign bodies occurs so rarely that removal should be performed early to avoid subsequent complications [3,4]. Spontaneous expulsion of foreign body bronchus is unimaginable and quite rare. Very few reports of such an occurrence are available in the literature. Negus (1948) has given an incidence of about 2% of spontaneous expulsion of foreign body from air passage while it has been quoted to vary between 2 to 4% by Chevalier Jackson [5–7].
“Nature cures by its own ways.” It is well known that nature has developed its own reflex protective mechanisms which are strong enough, but they seldom come into action up to the level of complete cure [5]. Spontaneous expulsion of foreign body bronchus is a rare entity with few cases reported in literature. Gupta and Sood reported two cases, One was a 2-year-old male child who spontaneously expelled out cycle tube metallic valve from right bronchus four days after inhalation while the other was a 20-year-old male who spontaneously expelled out a four anna metallic coin from trachea, few hours after its inhalation [8]. Ryndin VD reported two cases of aspirated needles which were expelled out spontaneously [9]. While SK Gupta reported spontaneous expulsion of iron nail from Left main bronchus [5] whereas Hadi MA mentioned spontaneous expulsion of iron nail from Rt lower lobe bronchus [10].
In our case, it is quite interesting and uncommon to see such a sharp & pointed metallic sewing machine needle which was lodged in Right Middle lobe bronchus was spontaneously expelled out without any complications. Definite history of inhalation and clinical manifestations such as choking, cough, respiratory distress and wheeze are important in diagnosis of foreign body inhalation [11]. Clinical manifestations depend on type, size and location of the foreign body. The diagnosis can be immediately established as in our patient, or, it can be delayed for the weeks or months especially if the history is not clear. Such cases may present with established complication such as emphysema, atelectasis, bronchectasis, pneumonia or lung abscess [10]. Roentegnograms are mandatory in establishing the diagnosis, locating the site of the foreign body and can also be helpful in demonstrating the presence of respiratory complication [10]. One more interesting thing is that it should be easier to lodge into as well as to be removed for a foreign body from right main bronchus due to obvious anatomical reasons. From anatomic consideration, inhaled foreign bodies are commonly located in right bronchial system as compared to the left [11] [Table/Fig-4]. In our case too, foreign body sewing machine needle was lodged in Right segmental bronchus & due to anatomical reasons must have expelled out spontaneously.
Comparison of inhaled foreign bodies in the right and left bronchial systems absolute and interpeak latencies of BAEP from previous studies [11]
| Site | % |
|---|
| Right main stem bronchus | 42.0-70.0 |
| Left main stem bronchus | 18.7-32.6 |
| Right segmental bronchi | 22.0 |
| Left segmental bronchi | 3.0 |
| Trachea | 27.5 |
| Larynx | 1.0-7.5 |
As subglottis is the narrowest part in the upper respiratory tract in children, there is always an obvious risk during spontaneous expulsion of foreign body from tracheobronchial tree, the foreign body may lodge into subglottis and may impose a life threatening emergency requiring urgent intervention [5]. It is unwise and dangerous and inadvisable to wait for spontaneous expulsion in cases of foreign body bronchus but while preparing for endoscopy, a constant watch should be kept over the patient and every forceful bout of cough should be looked with suspicion of spontaneous expulsion and a danger of foreign body lodgement into subglottis during such rare but possible occurrence should be kept in mind [5].
Removal of intrabronchial foreign bodies should be performed once the diagnosis is made. This can be achieved either by bronchoscopy or thoracotomy. Rigid bronchoscopy is the gold standard for removal of foreign bodies from tracheobronchial tree under direct vision. Spontaneous expectoration of foreign bodies is rare. Since time is of essence, delay in intervention complicates the picture and makes subsequent removal even more difficult [10]. Extrapulmonary foreign bodies, if asymptomatic, are best left alone. Intrapulmonary ones on the other hand, should be diagnosed promptly both clinically and radiologically and early intervention is advised to avoid complications [12]. Education is the best preventive measure for decreasing the incidence of this problem.
Conclusion
Sponataneous expulsion of sharp metallic foreign body from bronchus is a rare entity. Endoscopic removal is the mainstay of management of foreign body in tracheobronchial tree. Irrespective of size, shape and nature of foreign body, there is always a rare but existing possibility of spontaneous expulsion. On one hand, it saves the patient from the dangers of endoscopic removal of foreign body, but it may also impose a great danger of subglottic lodgement of foreign body.
[1]. Skoulakis Charalambos E, Panagiotis G, Doxas Papadakis Chariton E, Proimos Efklidis, Christodoulou Panos, Helidonis Emmanuel S, Bronchoscopy For Foreign Body Removal In Children. A Review & Analysis of 210 CasesInternational Journal of Pediatric Otorhinolaryngology 2000 53:143-48. [Google Scholar]
[2]. Kent SE, Watson MG, Laryngeal foreign bodiesThe Journal of Laryngology and Otology 1990 104:131-33. [Google Scholar]
[3]. Jackson C, Prognosis of foreign body in the lungJAMA 1921 77:1178 [Google Scholar]
[4]. Marc SS, Alan JC, Munir A, Spontaneous endobronchial erosion and expectoration of a retained intra thoracic bullet: Case reportThe Journal of Trauma 1992 33(6):909-11. [Google Scholar]
[5]. Gupta SK, Mundra RK, Goyal A, Indian Journal of’ Otolaryngology and Head and Neck Surgery 2004 56(3):233-34. [Google Scholar]
[6]. Negus VE, Diseases of nose and throat 1948 LondonCassell and Co.Ltd. [Google Scholar]
[7]. Jackson and Jackson: Diseases of nose, throat and ear 1959 2nd EdPhiladelphia and LondonW.B. Saunders Co. [Google Scholar]
[8]. Gupta IS, Sood VP, Foreign body in the air passage (spontaneous expulsion)Indian Journal of Otolaryngology 1967 19(4):173-76. [Google Scholar]
[9]. Ryndin VD, Octavio F, Two cases of spontaneous expulsion of aspirated needles from the lungsGrud Serdechnososudistaia Khir.” [jour] 1986 6:90-1. [Google Scholar]
[10]. Hadi MA, Al-Telmesani LM, Spontaneous expulsion of intrabronchial metallic foreign body: A case reportJ Fam Community Med 1997 4:77-9. [Google Scholar]
[11]. Liancai Mu, Ping He, Degiang Sun, Inhalation of foreign bodies in Chinese children: A review of 400 casesLaryngoscope 1991 101:657-60. [Google Scholar]
[12]. Mital OP, Prasad R, Singhal SK, Malika A, Singh PN, Spontaneous expulsion of a long standing endobronchial metallic foreign bodyIndian J Chest Dis Allied Sci 1979 21:45-7. [Google Scholar]