John Doe (male) or Jane Doe (female) refers to unknown persons or the unknown dead bodies [1] in USA or United Kingdom as persons whose true identity is unknown or it must be withheld in a legal action, case or discussion. In India the dead ones are simply referred to as unknown dead bodies.
The law everywhere and in every country requires that identification has to be carried out both in the living and in the dead [2,3]. This identification is primarily the domain of the investigative agencies and the forensic experts, both medical and non-medical, play an important role in the said process. This identification is achieved through numerous parameters, both conventional and scientific [4–8]. However, the problem of identification of “John Doe” gets aggravated and taxes the resources of most experienced forensic expert when they are recovered in skeletonised form or in mutilated state [9]. This mutilation may be intentional by the criminals in an effort to destroy all traces of identity or to facilitate disposal of the body [9]. In India, a dead body can be mutilated and the soft tissues completely devoured by various animals and vultures in a very short span of time, when disposed off in isolated lonely places. Mass disasters like earthquakes, bomb explosions, air-crash, railway accidents, etc. are other common instances where bodies can be found in a mutilated state [9,10]. Establishing identification and the cause of death as well as the manner of death in these “John Doe” cases can become a Herculean task. Organizations like NamUs [11] (The National Missing and Unidentified Persons System) in the United States help in the identification of unidentified persons.
Meticulous post-mortem examination of these cases will help in establishing the identity as well as to establish the cause of death. It is said that post mortems reveal the diseases and the lesions that the person lived with, and not necessarily those that killed him [10]. So, in these cases, after ruling out physical injury, one has also to rule out poisoning and disease. In order to do so, the usual viscera are sent for routine chemical analysis and histopathology, and an interim report is handed over to the police personnel. The final opinion regarding the cause of death is given after receiving the said reports from both the quarters concerned and after incorporating the findings. As far as possible, an attempt is made at giving a definite opinion; however, when this is not possible, “no definite opinion” is mentioned in the report as regards the cause of death and one should not venture to guess “some opinion”, just for the sake of giving opinions [10].
The project was started with the aim to study the cause and the pattern of cause of death in John or Jane Doe cases and to analyse the various efforts made on part of the investigating officer and the autopsy surgeon to establish identity in these cases.
Materials and Methods
Unidentified bodies brought for postmortem examination to the mortuary of the department of Forensic Medicine & Toxicology, Government Medical College & Hospital (GMCH), Chandigarh, India during the five year period 2008 – 2012 comprised the material for the study. Data regarding these cases was obtained from the postmortem reports, inquest papers; detailed history elicited from the concerned police officials at the time of autopsy, etc.
Observations and Results
A total of 3165 bodies were brought for postmortem examination to the mortuary of the Department during the 5yr period under study. Of these, unidentified cases “John Doe or Jane Doe” comprised 3.89% (123 cases). There were only two “Jane doe” (3%).
Maximum number of cases belonged to the age group 41-50 yr, 30.1%; followed by the age groups 31-40 & 21-30 yr, 26% and 13.8% respectively. The age groups <10 years and 11-20 yr accounted for the least number of cases, 4.9% and 4.1% [Table/Fig-1].
Age-wise distribution of unidentified cases
| Age Group | 2008 (n=19) | 2009 (n=18) | 2010 (n=23) | 2011 (n=19) | 2012 (n=44 ) | Total (n= 123) |
|---|
| No. | % | No. | % | No. | No. | No. | % | No. | % | | |
|---|
| <10 yrs | 0 | 00 | 2 | 11 | 0 | 0 | 1 | 5.2 | 3 | 6.8 | 6 | 4.9 |
| 11-20 yrs | 0 | 00 | 0 | 00 | 2 | 09 | 1 | 5.2 | 2 | 4.6 | 5 | 4.1 |
| 21-30 yrs | 4 | 21 | 5 | 28 | 3 | 13 | 4 | 21 | 1 | 2.3 | 17 | 13.8 |
| 31-40 yrs | 7 | 37 | 2 | 11 | 3 | 13 | 3 | 15.8 | 17 | 38.6 | 32 | 26 |
| 41-50 yrs | 7 | 37 | 6 | 33 | 8 | 35 | 4 | 21 | 12 | 27.3 | 37 | 30.1 |
| 51-60 yrs | 1 | 05 | 2 | 11 | 4 | 17 | 2 | 10.5 | 6 | 13.6 | 15 | 12.2 |
| > 60 yrs | 0 | 00 | 1 | 06 | 3 | 13 | 3 | 15.8 | 4 | 6.8 | 11 | 8.9 |
Overall, the maximum number of cases were encountered in the month of Oct, 12.2%; followed by June and Dec, 11.4% each; while the least number of cases was seen in the months of Jan and March 4.1%, each. However, year-wise, there was no such pattern – the months when maximum cases were brought to the mortuary being: January in 2008, April & May in 2009, June in 2010 Oct in 2011 and July in 2012 [Table/Fig-2].
Month-wise distribution of the cases
| Month | 2008 (n=19) | 2009 (n=18) | 2010 (n=23) | 2011 (n=19) | 2012 (n=44 ) | Total (n= 123) |
|---|
| No. | % | No. | % | No. | No. | No. | % | No. | % | No. | % |
|---|
| Jan | 4 | 21 | 0 | 00 | 0 | 00 | 0 | 0 | 1 | 2.3 | 5 | 4.1 |
| Feb | 2 | 11 | 2 | 11 | 1 | 04 | 0 | 0 | 4 | 9.0 | 9 | 7.3 |
| Mar | 0 | 00 | 1 | 06 | 1 | 04 | 1 | 5.2 | 2 | 4.6 | 5 | 4.1 |
| Apr | 2 | 11 | 3 | 17 | 1 | 04 | 0 | 0 | 2 | 4.6 | 8 | 6.5 |
| May | 1 | 05 | 3 | 17 | 4 | 17 | 0 | 0 | 5 | 11.4 | 13 | 10.6 |
| June | 2 | 11 | 1 | 06 | 6 | 26 | 1 | 5.2 | 4 | 9.0 | 14 | 11.4 |
| July | 1 | 05 | 1 | 06 | 3 | 13 | 0 | 0 | 7 | 15.9 | 12 | 9.7 |
| Aug | 2 | 11 | 2 | 11 | 0 | 00 | 0 | 0 | 6 | 13.6 | 10 | 8.1 |
| Sep | 2 | 11 | 1 | 06 | 2 | 09 | 3 | 15.8 | 2 | 4.6 | 10 | 8.1 |
| Oct | 2 | 11 | 2 | 11 | 2 | 09 | 7 | 36.8 | 2 | 4.6 | 15 | 12.2 |
| Nov | 1 | 05 | 1 | 06 | 0 | 00 | 3 | 15.8 | 3 | 6.8 | 8 | 6.5 |
| Dec | 0 | 00 | 1 | 06 | 3 | 13 | 4 | 21 | 6 | 13.6 | 14 | 11.4 |
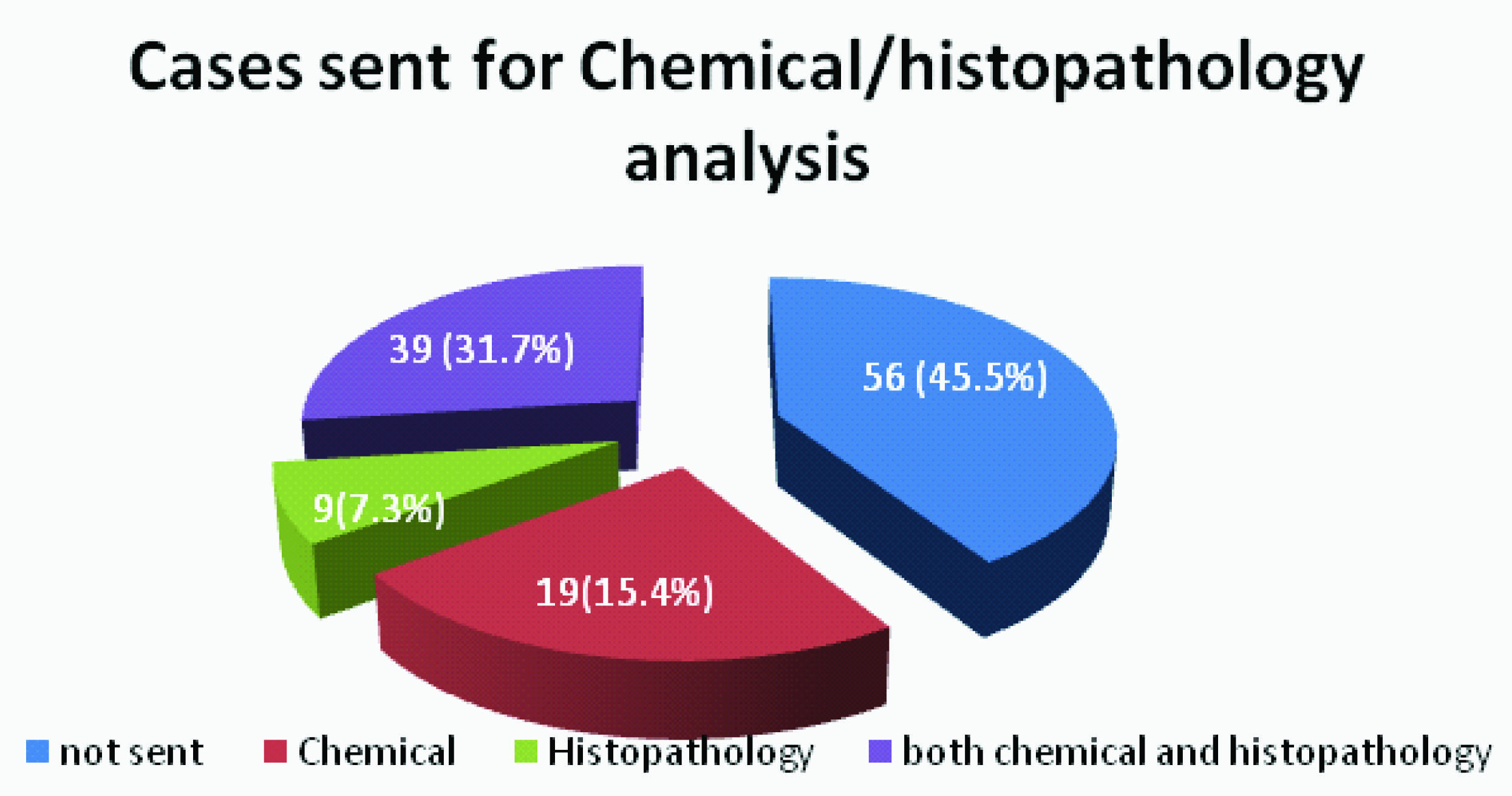
Opinion regarding the cause of death was given at the time of autopsy in 45.5% of cases while in the remaining cases additional investigations were requested. Viscera for chemical analysis were sent in 15.4%cases, histopathology in 7.3% and for both chemical analysis and histopathology, in 31.7% cases [Table/Fig-3].
Cases sent for Chemical/ Histopathological analysiss
Majority of the opinions regarding the cause of death in “John Doe” cases during the 5yr period were either given as ‘cranio-cerebral damage’ or the opinion regarding the same was reserved for want of the reports of the toxicological and histopathological analysis of the viscera. Haemorrhage and shock, and multiple organ failure/disease was responsible in 9.8% cases each whereas coronary insufficiency/ cardiac disease laortic aneurysm were responsible for 8.9% deaths, [Table/Fig-4].
Cause of death-wise distribution of cases
| S No | Cause of Death | 2008 (n=19) | 2009 (n=18) | 2010 (n=23) | 2011 (n=19) | 2012 (n=44 ) | Total (n= 123) |
|---|
| 1 | Cranio-cerebral damage | 5 | 26 | 6 | 33 | 7 | 30 | 5 | 26.3 | 14 | 31.8 | 37 | 30.1 |
| 2 | Opinion reserved | 6 | 32 | 4 | 22 | 7 | 30 | 7 | 36.8 | 14 | 31.8 | 38 | 30.9 |
| 3 | Coronary insufficiency | 3 | 16 | 1 | 06 | 1 | 09 | 0 | 0 | 2 | 4.5 | 7 | 5.7 |
| 4 | Hemorrhage & shock | 0 | 00 | 2 | 11 | 2 | 09 | 4 | 20.8 | 4 | 9.1 | 12 | 9.8 |
| 5 | No Definite opinion | 2 | 11 | 2 | 11 | 0 | 00 | 0 | 0 | 4 | 9.1 | 8 | 6.5 |
| 6 | Cardiac disease | 0 | 00 | 0 | 00 | 2 | 13 | 0 | 0 | 0 | 00 | 2 | 1.6 |
| 7 | Rupture aortic aneurysm | 0 | 00 | 0 | 00 | 2 | 13 | 0 | 0 | 0 | 00 | 2 | 1.6 |
| 8 | Hanging | 1 | 05 | 1 | 06 | 0 | 00 | 0 | 0 | 0 | 00 | 2 | 1.6 |
| 9 | Cirrhosis of liver | 0 | 00 | 1 | 06 | 0 | 00 | 0 | 0 | 0 | 00 | 1 | 0.8 |
| 10 | CO poisoning/ poisoning | 1 | 05 | 0 | 00 | 0 | 00 | 0 | 0 | 1 | 2.3 | 2 | 1.6 |
| 11 | Multiple disease conditions | 1 | 05 | 1 | 06 | 2 | 13 | 3 | 15.6 | 5 | 11.4 | 12 | 9.8 |
The police usually took 10 -15d on an average to get the postmortem conducted in “John Doe” cases [Table/Fig-5]. The police had completed all their formalities regarding photographs and publication of notice in dailies in all the cases. They had, however, taken fingerprints in 40% cases only. In rest of the cases the fingerprints were not taken by the police, either because a request for the same was made to the forensic expert or the body was either mutilated, decomposed, or was skeletonised. The autopsy surgeon, on the other hand, had handed over clothes in 46% cases (to facilitate the process of identification), finger pulps of all the ten fingers in separate sealed packets in 43% cases, noted the marks of identification (65%), deformities/tattoos in 19% cases and preserved sternum for DNA analysis and blood for cross matching in 8%cases [Table/Fig-6].
Time between death and Post mortem
| Days | 2008 (n=19) | 2009 (n=18) | 2010 (n=23) | 2011 (n=19) | 2012 (n=44 ) | Total (n= 123) |
|---|
| 0-3 days | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 0 |
| 4-6 days | 1 | 5.2 | 2 | 11 | 2 | 8.7 | 1 | 5.2 | 3 | 6.8 | 9 | 7.3 |
| 7-9 days | 2 | 10.4 | 1 | 5.5 | 4 | 17.4 | 3 | 15.6 | 5 | 11.3 | 15 | 12.2 |
| 10-12days | 6 | 31.2 | 4 | 22 | 5 | 21.5 | 4 | 20.8 | 8 | 18.1 | 27 | 22 |
| 13-15 days | 3 | 15.6 | 5 | 27.5 | 5 | 21.5 | 4 | 20.8 | 10 | 22.7 | 27 | 22 |
| 16-18 days | 3 | 15.6 | 2 | 11 | 2 | 8.7 | 2 | 10.4 | 5 | 11.3 | 14 | 11.4 |
| 19-21 days | 1 | 5.2 | 1 | 5.5 | 1 | 4.3 | 2 | 10.4 | 4 | 9 | 9 | 7.3 |
| 22-24 days | 1 | 5.2 | 1 | 5.5 | 0 | 0 | 0 | 0 | 2 | 4.6 | 4 | 3.2 |
| 25-27 days | 0 | 0 | 0 | 0 | 1 | 4.3 | 0 | 0 | 1 | 2.3 | 2 | 1.6 |
| 28-30 days | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 1 | 2.3 | 1 | 0.8 |
| >30 Days | 2 | 10.4 | 2 | 11 | 3 | 13.2 | 3 | 15.6 | 5 | 11.3 | 15 | 12.2 |
Efforts put in to establish identity
| Type of efforts | 2008 (n=19) | 2009 (n=18) | 2010 (n=23) | 2011 (n=19) | 2012 (n=44 ) | Total (n= 123) |
|---|
| n% | n% | n% | n% | n% | n% |
| Efforts of the police |
| Fingerprints | 7 | 37 | 7 | 39 | 10 | 43 | 5 | 26.3 | 20 | 45 | 49 | 40 |
| Photographs | 19 | 100 | 18 | 100 | 23 | 100 | 19 | 100 | 44 | 100 | 123 | 100 |
| Advts. In dailies | 19 | 100 | 18 | 100 | 23 | 100 | 19 | 100 | 44 | 100 | 123 | 100 |
| Inquiry from people | 19 | 100 | 18 | 100 | 23 | 100 | 19 | 100 | 44 | 100 | 123 | 100 |
| Data/material retrieved by the autopsy surgeon |
| Clothes handed over | 12 | 63 | 10 | 56 | 16 | 70 | 4 | 21 | 14 | 32 | 56 | 46 |
| Noting: Tattoos | 4 | 21 | 3 | 17 | 6 | 26 | 1 | 5.2 | 3 | 7 | 17 | 14 |
| Deformities | 1 | 05 | 0 | 00 | 2 | 13 | 0 | 0 | 3 | 7 | 06 | 05 |
| Marks of identification | 5 | 26 | 4 | 22 | 8 | 35 | 19 | 100 | 44 | 100 | 80 | 65 |
| Finger pulps preserved | 8 | 42 | 10 | 56 | 14 | 61 | 5 | 26.3 | 16 | 36 | 53 | 43 |
| Sternum for DNA/ Blood for cross match | 0 | 00 | 1 | 06 | 3 | 13 | 1 | 5.2 | 9 | 20 | 10 | 8 |
Discussion
In every autopsy surgeon’s career, unidentified bodies brought for postmortem examination comprise a small but a very significant and important group of cases. These cases test the real skills and expertise of the forensic expert and the investigative agencies, to the limit. Most of the unknown cases require time consuming formalities, as required by the law, viz., a waiting period of about 72h, hue and cry appeals along with publication of photographs and details of the deceased in the leading dailies, interactive pooling of data from various agencies all over the country, etc., to name a few. A forensic medicine specialist opines regarding the cause, manner and nature of death, based on his findings, reports of the investigations sought by him from different laboratories. Thus, he contributes very useful information regarding the unknown dead body, by giving detailed data gathered from a thorough examination and dissection of the body. It is here that his skill and expertise come in to play.
A thorough search of the literature did not yield much information regarding the efforts that were put in to establish the identity of the unidentified dead in the Indian context. Most of the literature emphasised on the individual body identification or identification of victims of mass disasters [7,12–15]. In the present study, unidentified bodies comprised 3.89% of the total autopsy load of the department during period under consideration. In other studies, it was observed that John Doe cases accounted for about 4- 10% of the total autopsy load [15,16]. John Doe cases accounted for 97% of the total cases as compared to 87% of cases in a study in Kolkata [17] and 80 % in US [1]. Similar observations were published from Maharashtra [12]. These observations can be supported by the fact that India is a predominantly patriarchal society where man earn for livelihood outside and the women’s main domain is her home – be it her parental or in-laws. As such, they leave their homes in search of jobs and venture to far off places for better opportunities of earning their livelihood. Many a times, the family is even not aware of the place of employment of the person and in case of his death at such places, his body is brought to the morgue as “unidentified”, where legal formalities dictate a post-mortem examination. The age group 31-60 was responsible for 68.3% of cases, similar to the study done by Chattopadhyay [17]. This is the most mobile age group for various reasons, both economic and social and hence also the age group prone to unnatural deaths – suicidal, accidental or homicidal. This is in contrast with our previous studies where we observed the most common age group to be 16-25 yr in cases of hanging [18], 21-30 yr in cases of poisoning, burns and vehicular accidents [19−22]. Though the socio-economic data of these John Doe cases could not be compiled for obvious reasons, usually a majority of these cases are from the lowermost rungs of the socio-economic ladder.
Viscera were sent for chemical analysis in 61% cases. In the other 39% cases, the cause of death was either obvious or histopathology report was sought. Of the 75 cases in which viscera were sent for analysis, reports were not received in about half (47%) cases till finalisation of this paper. This is a very sizeable percentage of cases and speaks volumes of the delay taken by the various laboratories in processing the cases [23]. This has become a routine in our present medico-legal set-up where it takes several years sometimes for the reports to reach the autopsy surgeon. Even when they are received, they may be inconclusive in a majority of cases, making the task of giving a definite opinion regarding the cause of death very difficult.
Cranio cerebral trauma was the principal cause of death in 37 (75.5%) cases out of a total of 49 trauma cases. This result was similar to the study done by Paulozzi in US [1] wherein, among all deaths for which the cause was known, 82.7% were due to injuries. Mechanical trauma may be one of the reasons why the body remained unidentified. This could be in instances such as a) hit and run accidents with crushing of head and face, b) body being dismembered when being run over by a heavy vehicle or train, c) a person being involved in a fatal accident just on arrival in a completely new place, etc.
In the present study nearly 50% of the cases were natural deaths. These results were more or less similar to the study done by Chattopadhyay [17] where nearly half (48.3%) of the cases were due to some diseases, pathological conditions or old age.
The chances of the body getting identified increases if it is a case of homicide. Homicidal manner of death with firearms/sharp weapons did not find mention in any of the cases in the present study and one of the probable reasons could be that the police make sincere efforts to trace the victim in order to solve the crime on priority basis and thus the body no longer remains unknown. Moreover, homicide of unknown persons is a rarity unless it is done with the motive of robbery. This was in contrast to 5.9% of homicides observed by Chattopadhyay [17].
Some of the routine steps undertaken by the police in order to trace the unidentified bodies are taking and preserving fingerprints (40%), publishing photographs in dailies/ newspapers (100%), pasting pamphlets outside mortuaries/ hospitals/ police stations/railway stations,(100%) etc. Besides these, advertisements in the local TV channels are aired and a thorough enquiry is made in the locality (100%) in which the dead body was found. Though this kind of activity results in greater number of bodies getting identified but it is a time consuming process and the police usually requests a post-mortem examination only after completing the above mentioned formalities. This postponement of request by the police for autopsy till all efforts at identifying the body are exhausted is usually done to avoid unwanted allegations by the relatives at a later date when the body is identified. This exercise usually delays post mortems (75%) examination to between 7-21 days.
The efforts by the autopsy surgeon to facilitate the process of identification of the victim were not sufficient due to the lack of a common proforma detailing the steps. In some of the cases doctor preserved samples for DNA analysis whereas in other cases it was not done. Clothes of the victim were given unsealed to the IO in 63% of the cases. This was so because many a times, identification is based on the personal artefacts of the victim and it may be the only means of identification by the relatives. Noting of the tattoo marks were done in all the cases which had tattoos engraved on them, (22%) so that some clue as regards the positive identification of the victim is made. Relatives easily recognize the tattoos on the person of their near and dear ones, and in these cases, even the description of the tattoos help in identification. Visible marks of identification were recorded (at least two) in 28% cases. Fingerprints are the gold standard for identification and hence, the pulps of the finger were removed and preserved in separate labelled bottles in formalin in 53% of the cases on the request of the police. Though this method might seem barbaric and amounts to mutilation of the dead body, it is in vogue in this part of the country. Sternum bone for DNA analysis/ blood for cross matching were sent in 7% of the cases, again on the request of the police officials.
Conclusion and Suggestions
Unidentified dead bodies were only 4% of the total dead bodies coming to the autopsy in the mortuary of the department. However, as is clear from the above, these cases take far more time and effort in their processing; which still remains incomplete.
Following suggestions may help streamline the process:
Drafting of additional legislation for the management of unidentified dead bodies.
Efforts for identification on the part of police personnel should be streamlined and procedures to be laid down and followed strictly.
Bodies that are unknown/ unclaimed should be presented for autopsy forthwith without any delay so that decomposition and other artefacts do not set in and obscure the findings of the postmortem examination.
Active investigation and modern investigative techniques are to be used, workload of the police officers needs to be redistributed, and accountability of the police has to be fixed to get the body identified.
Internet based sites of the police like ZIPNET [24] (Zonal Integrated Police Networking) in Northern India, where entries of all the missing persons/ John Doe cases are recorded should be made popular so that chances of the body getting identified increases.
Proformas detailing simple colour photograph of the body, especially of the clothes, the tattoo marks, scars, deformities, old fracture sites, dental records, full body X-ray, description of surgical implants, fingerprints etc will help the police in identifying such bodies.
DNA analysis and fingerprinting should be done in each and every case so that proper records will be there for identification of the deceased years after the death or postmortem.
The efforts of getting the body identified on the part of both the police and the autopsy surgeons, seemed short to an extent and much could have been done. With a little effort on the part of the doctor and the investigation officer, in many cases, surprisingly, a large amount of information could have been obtained even in the presence of advanced state of decomposition. Such information could have been of use to the doctor and the investigation agencies both in establishing identity and in forming an opinion about the cause and manner of death.