A mucocele is a common benign lesion of the minor salivary gland mucosa that most frequently affects children and young adults. A 6-year-old male patient reported to the Department of Pedodontics and Preventive Dentistry, with the chief complaint of a painless swelling on floor of the mouth on his left side. The purpose of this case report is to present the treatment of mucocele present in floor of the mouth in a child patient using liquid nitrogen cryosurgery. Also, discussed are the mechanism of action, current protocol of cryosurgery recommended in the management of mucoceles, clinical advantages and disadvantages together with the clinical outcomes.
Case Report
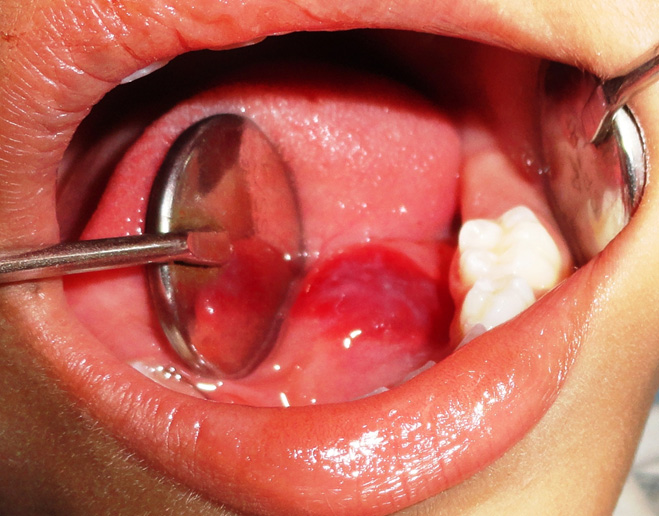
A 6-year-old male patient reported to the Department of Pedodontics and Preventive Dentistry, Sardar Patel Post Graduate Institute of dental and Medical Sciences, Lucknow, India with the chief complaint of a painless swelling on floor of the mouth on his left side which had been present since three weeks [Table/Fig-1]. Past medical, family and dental history was not contributory. Upon examination, the lesion appears well circumscribed, transparent, single bump with slight bluish or normal colour, around half inch in size, painless, flaccid consistency, clearly defined limits and a smooth surface.

A differential diagnosis of mucocele, oral hemangioma, oral lympangioma, lipoma, and soft tissue abscess was made. The history and clinical findings lead to the diagnosis of a superficial mucocele. The appearance of mucocele is pathognomonic, and so the data about the lesion location, rapid appearance, size, bluish colour and the consistency.
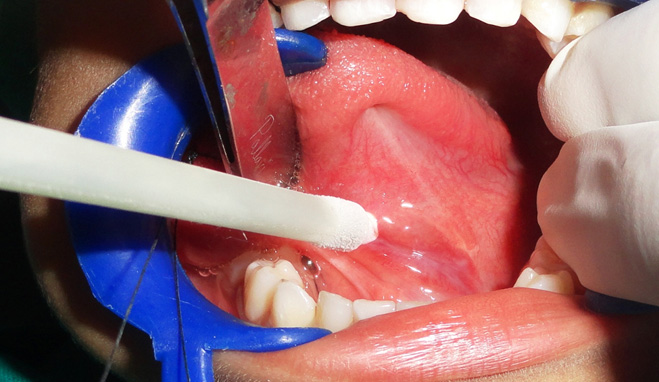
Signed informed consent was given by the parents. Considering his young age, the option of treatment was cryosurgery. Local anesthesia was given to anesthetise the surrounding structures. A thread of suture material was passed through the tongue, to deflect the tongue to the opposite side and to gain the proper access. A cryoprobe was attached to the liquid nitrogen spray equipment. The lesion was exposed directly to four consecutive freeze-thaw cycles [Table/Fig-2]. Each cycle lasted 5 to 10 sec and moved from the center of the lesion to the borders until the lesion appeared white and frozen, resembling an ice ball [Table/Fig-3]. [Table/Fig-4,5and6] shows the clinical appearance immediately, three days and one week after the procedure repectively. No recurrence at the 1st,3rd and 6th months follow-up was reported [Table/Fig-7].

Photograph immediately after treatment
3rd day follow-up photograph

One week follow-up photograph

3 months follow-up photograph

Discussion
Mucocele is a common lesion of the oral mucosa that results from an alteration of minor salivary glands due to a mucous accumulation. It causes limited swelling. When located on the floor of the mouth these lesions are called ranulas because the inflammation resembles the belly of a frog [1,2].
Children are most commonly affected with equal gender predilection and with a clinical history of a painless swelling, often recurrent in nature that may be present for months or even for years before the patient seeks the treatment [3]. Generally, histological examination is required to confirm lesion diagnosis but biopsy prior to cryotherapy may compromise the final result for clinically diagnosable lesions such as mucoceles [4].
Several treatment modalities have been proposed in literature for management of mucoceles, varying from excision of the lesion, marsupialisation, micromarsupialisation, carbon dioxide laser, gamma-linolenic acid and Erbium laser. A novel method of injecting an ultraflow rubber base impression material into a mucocele on the tongue’s ventral surface. This procedure showed a clear demarcated limit of the lesion, making surgical excision easier [5,6].
Surgical treatment of such cystic lesion in children poses more difficult situation compared to adults. A variety of non surgical procedures have been proposed for therapy of ranula, all of them aiming at avoiding surgery in the floor of the mouth, which may be complicated by the proximity to important structures like the submandibular duct and the lingual nerve and artery [6].
Cryotherapy is the deliberate destruction of tissue by application of extreme cold. Reports of tissue destruction by freezing date back to the British physician, Arnott. He treated breast cancer, uterine cancers, and some skin cancer with this modality of treatment. Gage treated oral cancers with liquid nitrogen [4,5].
Nowadays, liquid nitrogen is by far the most popular cryogen agent, and been used in different specialties. Temperatures of-25°C to -50°C (-13°F to -58°F) can be achieved within 30sec if a sufficient amount of liquid nitrogen is applied by spray or probe. Inflammation develops during 24h after treatment, further contributing to destruction of the lesion through immunologically mediated mechanisms. After cryosurgery, blister formation and oedema occur between 24h and 72h and crusting between 3 day and 14 day in all patients [5].
Mechanism Of Action Of Cryosurgery
The basic technique of cryotherapy stresses rapid cooling, slow thawing and repetition of the freezing process to maximize tissue destruction The two methods recognized are a closed system with use of probes and nitrous oxide, or an open system with use of a liquid nitrogen spray or a cotton tip [4,7]. In the present case, closed system was used. These probes follow the principles of Joule-Thompson expansion which enable substances to undergo a drop in temperature when moved from a high pressure area to a lower pressure area [4,8].
For instance, when nitrous oxide is released from the high pressure inside the cryoprobe to the lower pressure cryo tip, the drop in temperature allows freezing of the tissues to occur. At present, the optimal temperature of cell death is unclear, however, it has been determined that most tissues freeze at -2.2°C and that the temperature must fall below -20°C for cell death to occur [4,7,8].
Immediately following treatment, cryolesions are indistinguishable from the original tissue. However, latent damage is produced which progresses to severe damage and subsequent necrosis to the tissues in following days [8].
During the freeze cycle as the temperature drops, it is believed that extracellular water undergoes crystallisation. In addition, membrane lipids harden at low temperatures decreasing cell resistance to shrinkage. As extracellular stores of water diminish, the electrolyte concentration increases. In order to counteract this concentration gradient, intracellular water moves out of the cell, and this water becomes involved in the crystallisation process. Also, intracellular ice formed remains trapped within the cellular membrane. As a result of these processes, intracellular electrolytes reach toxic levels, which become lethal to the cell. During a slow thaw cycle, cells at the periphery of the cryolesion will take up excess electrolytes. To equalise this gradient, water enters the cell and can lead to swelling and lysis [7,8].
Cryotherapy is well-received by patients due to a relative lack of discomfort, the absence of bleeding and minimal to no scarring. It is an effective, simple, predictable, relatively self-limiting and safe method for almost all types of oral lesions. As it causes necrosis and sloughing as part of treatment, delayed healing is an inherent problem with this technique else, it is free from complications such as pain, haemorrhage, infection, inadvertant damage to adjacent structures or scar formation that are seen with knife excision or electrosurgery. Surgical excision and sutures can make children and parents anxious. Cryotherapy can be repeated without permanent side effects and is more localised in action than radiotherapy or chemotherapy. Perhaps its greatest advantage is its usefulness in candidates for whom surgery is contraindicated due to either age or medical history [5,9].
The main disadvantage of this technique is the lack of a specimen to be examined microscopically to confirm the diagnosis. Other disadvantages include unpredictable degree of swelling and lack of precision with depth and area of freezing [5]. According to Farah and Savage, current protocols suggest that for most benign mucosal lesions, a 1 to 2 min freeze-thaw cycle using a cryoprobe is sufficient [4].
Conclusion
Mucoceles are caused when a salivary duct is severed and the mucus spills into the adjacent tissue forming a mass surrounded by granulation tissue. These lesions are predominant in children. Several treatment modalities have been described in literature, which includes liquid nitrogen cryosurgery—a therapeutic alternative for treating mucoceles in children.
[1]. Ata-Ali J, Carrillo C, Bonet C, Balaguer J, Peñarrocha M, Peñarrocha M, Oral Mucocele: Review Of The LiteratureJ Clin Exp Dent 2010 2(1):e10-3. [Google Scholar]
[2]. Suresh BV, Vohra SK, Huge Plunging RanulaJ Maxillofac Oral Surg 2102 11(4):487-90. [Google Scholar]
[3]. Sagari SK, Vamsi KC, Shah D, Singh V, Patil GB, Saawarn S, Micro- marsupialization: A minimally invasive technique for mucocele in children and adolescentJournal of Indian Society of Pedodontics and Preventive Dentistry 2012 30(3):188-91. [Google Scholar]
[4]. Farah CS, Savage NW, Cryotherapy for treatment of oral lesionsAustralian Dental Journal 2006 51(1):2-5. [Google Scholar]
[5]. Moraes PC, Teixeira RG, Thomaz LA, Arsati F, Junqueira JLC, Oliveira LB, Liquid Nitrogen Cryosurgery for Treatment of Mucoceles in ChildrenPediatr Dentistry 2012 34:159-61. [Google Scholar]
[6]. Shehata EA, Hassan HS, Surgical Treatment of Ranula: Comparison between Marsupialization and Sublingual Sialadenectomy in Pediatric PatientsAnnals of Pediatric Surgery 2008 3(4):89-93. [Google Scholar]
[7]. Pogrel MA, The use of liquid nitrogen cryotherapy in the management of locally aggressive bone lesionsJ Oral Maxillofac Surg 1993 51:269-73. [Google Scholar]
[8]. Salmassy DA, Pogrel MA, Liquid nitrogen cryosurgery and immediate bone grafting in the management of aggressive primary jaw lesionsJ Oral Maxillofac Surg 1995 53:784-90. [Google Scholar]
[9]. Narula R, Malik B, Role of Cryosurgery in the Management of Benign and Premalignant Lesions of the Maxillofacial RegionIndian Journal of Dental Sciences 2012 2(4):63-66. [Google Scholar]