Rupture of Aortic Sinus Valsalva Aneurysm and its Management
Kalyan Chakravarthy Peddinti1, Vijayalakshmi Gattu2, Kartika Balaji Samala3, Manikumari Karuturi4, Pratap Ramathoti5
1 Assistant Professor, Department of Anaesthesiology and Critical Care, GSL Medical College and General Hospital, Lakshmipuram, Rajahmundry, Andhra Pradesh, India.
2 Professor, Department of Anaesthesiology and Critical Care, GSL Medical College and General Hospital, Lakshmipuram, Rajahmundry, Andhra Pradesh, India.
3 Senior Resident, Department of Anaesthesiology and Critical Care, GSL Medical College and General Hospital, Lakshmipuram, Rajahmundry, Andhra Pradesh, India.
4 Postgraduate, Department of Anaesthesiology and Critical Care, GSL Medical College and General Hospital, Lakshmipuram, Rajahmundry, Andhra Pradesh, India.
5 Professor and Head, Department of Anaesthesiology and Critical Care, GSL Medical College and General Hospital, Lakshmipuram, Rajahmundry, Andhra Pradesh, India.
NAME, ADDRESS, E-MAIL ID OF THE CORRESPONDING AUTHOR: Dr. Kartika Balaji Samala, Senior Resident, Department of Anaesthesiology and Critical Care, GSL Medical College and General Hospital, Lakshmipuram, Rajahmundry-533296,Andhra Pradesh, India.
Phone: 9959216211
E-mail: Kartik1414@gmail.com
Here, we present successful management of a patient with rupture of right sinus valsalva and ventricular septal defect. Aneurysm of the aortic sinus also known as sinus of valsalva (ASOV) is a rare cardiac defect which can be congenital or acquired. Right coronary sinus (most common) usually ruptures into the right ventricle causing left to right shunt as seen in our patient. Unruptured aneurysms cause obstruction to right ventricular outflow tract. A 29-year-old male patient presented with dyspnea, palpitations, easy fatigability and severe limitation of physical activity. Transthoracic echocardiography showed membranous out pouching of the right coronary cusp (RCC) into the right ventricle. Patient was medically managed with drugs. Under general anaesthesia, after instituting cardiopulmonary bypass (CPB) surgical repair with pericardial patch, closure of subpulmonic ventricular septal defect was performed. Patient vitals were stable after surgery and he was asymptomatic on the first follow-up after discharge.
Cardiopulmonary bypass, Right coronary cusp, Sinus of valsalva aneurysm
Case Report
A 29-year-old patient came to our hospital with worsening exertional dyspnea of three months duration. He also complained of cough since five months, palpitations, swollen neck veins, feet and easy fatigability since three months. Palpitations were precipitated by exertion and relieved on taking rest. Patient gave history of severe limitation of physical activity.
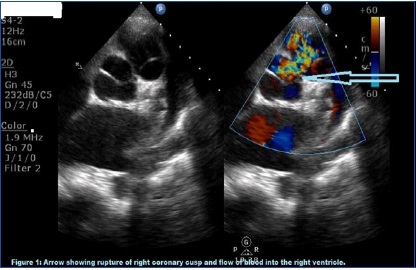
On physical examination, patient was in respiratory distress with a rate of 30 per minute. He had a regular bounding pulse of 116 beats/minute and blood pressure of 115/50 mm Hg. He had an elevated jugular venous pressure and pitting ankle oedema. On auscultation, his lungs were clear. Precordial examination revealed a grade 4/6 continuous murmur best heard over left sternal border. Chest X-ray revealed cardiomegaly and pulmonary venous congestion. ECG showed sinus tachycardia. Transthoracic echocardiography of patient showed a membranous out pouching of the right coronary cusp (RCC) into the right ventricle with 8.0 mm width perforation. Coronary angiogram showed normal study [Table/Fig-1]. A diagnosis of ruptured aneurysm of right sinus of valsalva was confirmed and patient was managed with diuretics, ACE inhibitors, digoxin, antibiotics and planned for surgery.
Arrow showing rupture of right coronary cusp and flow of blood into right ventricle
Patient was premedicated with midazolam and induction of anaesthesia was performed in a propped up position. General anaesthesia was maintained with Isoflurane, Vecuronium, Fentanyl. Intraoperative monitoring with ECG, pulseoximetry, capnography, temperature, urine output was done. Invasive arterial blood pressure monitoring was done after right radial artery cannulation and CVP monitoring by right internal jugular vein cannulation. Cardiopulmonary bypass (CPB) was instituted after securing cannulas for the aorta, superior vena cava, inferior vena cava. Pericardial patch was used to repair rupture sinus of valsalva and also closure of subpulmonic ventricular septal defect. Patient was transferred to ICU intubated and extubated six hours later. On postoperative day-1, chest tubes were removed and patient discharged on day-7. Patient was asymptomatic on the first follow up after discharge.
Discussion
A ruptured sinus of valsalva aneurysm is rare. It is usually congenital in origin. Congenital aneurysms result from localized weakness of elastic lamina at the junction of aortic media and annulus fibrosus. They are usually seen in patients with Marfans and Ehlers-Danlos syndrome [1]. Acquired aneurysms are caused by infectious diseases like bacterial-endocarditis, syphilis, tuberculosis. Degenerating conditions like atherosclerosis, cystic medial necrosis, injury from deceleration trauma are also associated with acquired ASOV [2]. The most common cardiac anomalies with ASOV are ventricular septal defects (30-60%), aortic insufficiency (20-30%), bicuspid aortic valve (10%) and coronary anomalies [3].
The sinuses are named according to their relationship with the coronaries. i.e. the right coronary sinus, the left coronary sinus and the non-coronary sinus [4]. Among the congenital sinus of valsalva aneurysms, right coronary accounts for 65-85%, non-coronary (10-30%) and left coronary very rare (less than 5%) [5].
The right coronary sinus (most common) usually ruptures into the right ventricle causing left to right shunt as seen in our patient [6]. Sometimes it may rupture into the right atrium. Non-coronary sinus usually ruptures into the right atrium and left coronary sinuses though rare may rupture into pericardium causing tamponade and death if unrecognised. About one-third of patients develop left-to-right shunting immediately following the rupture of aneurysm into right heart causing dyspnea and chest pain. Half of the patients show gradually worsening dyspnea, fatigue, chest pain, peripheral oedema over months or years following rupture as seen in our patient. Compensatory mechanisms in the body were not helpful but in our patient it showed the features of congestive heart failure. Body adjusts hemodynamically to the left-to-right shunting in asymptomatic patients. As the degree of shunt increases, volume overload overcome the compensatory mechanisms causing congestive heart failure [7]. Unruptured aneurysms cause obstruction to right ventricular outflow tract. Arrhythmias, complete heart block, myocardial ischemia, transient ischemic attacks are sometimes associated with unruptured aneurysms.
Our patient showed complaints with three months duration and his diagnosis was confirmed by transthoracic echocardiography and coronary angiography. Transesophageal echocardiography (TEE) is an invaluable tool in the operating room for anesthesiologist and could not be used due to the lack in our hospital setup. Intraoperative events were uneventful during induction, surgical correction when patient was on CPB and post extubation.
Conclusion
Here, we would like to say rupture ASOV is not so common and particular attention should be given in optimizing medications for heart failure and perioperative management.
[1]. Takahashi T, Koide T, Yamaguchi H, Nakamura N, Ohshima Y, Suzuki J, Ehlers-Danlos syndrome with aortic regurgitation, dilation of the sinuses of valsalva, and abnormal dermal collagen fibrilsAm Heart J 1992 123:1709-12. [Google Scholar]
[2]. Feldman DN, Roman MJ, Aneurysms of the sinus of valsalvaCardiology 2006 106:73-81. [Google Scholar]
[3]. Sakakibara S, Konno S, Congenital aneurysm of the sinus of valsalva associated with ventricular septal defect. Anatomical aspectsAm Heart J 1968 75:595-603. [Google Scholar]
[4]. Perloff JK, The clinical recognition of congenital heart disease 1978 2nd edPhiladelphiaWB Saunders:590-03. [Google Scholar]
[5]. Fishbein MC, Obma R, Roberts WC, Unruptured sinus of valsalva aneurysmAm J Cardiol 1975 35:918 [Google Scholar]
[6]. Yilmaz AT, Demirkilic U, Ozal E, Tatar H, Ozturk OY, Aneurysms of the sinus of valsalvaJ Cardiovasc Surg 1997 38:119-24. [Google Scholar]
[7]. Bonfils-Roberts EA, DuShane JW, McGoon DC, Danielson GK, Aortic sinus fistula-surgical considerations and results of operationAnnals of Thoracic Surgery 1971 12:492-502. [Google Scholar]