Background: Only few studies about neck circumference (NC) as a measure of cardio metabolic syndrome available from India. Study was conducted to establish an association between neck circumference and cardio metabolic syndrome.
Material and Methods: Cross-sectional study was conducted in a tertiary care hospital in South India. NCEP: ATPIII 2001 guideline was used for diagnosis of Cardio-metabolic syndrome among subjects. Neck circumference was measured and it was correlated with Cardio-metabolic syndrome.
Results: Mean neck circumference was found to be 36.5 cms. Cardio-metabolic syndrome was present in 272 participants, of which 100 were females and 172 males. Among females 82(82%) had neck circumference >34cms, 18(18%) had <34cms and among males 117(68%)had NC >37cms and 55(32%) had NC<37cms. All individual parameter of cardio metabolic risk factor, i.e., BMI, waist circumference, hip circumference, systolic blood pressure, diastolic blood pressure, FBS, HDL & TG except waist/hip ratio were correlating with abnormal neck circumference when compared with those with normal neck circumference.
Conclusion: Neck circumference with metabolic syndrome correlated better among females than males. Men with NC >37 cm and women with NC >34 cm are more prone for cardio metabolic syndrome and require additional evaluation. Measurement of NC is a simple, time saving, and least invasive measurement tool.
Introduction
Alarming raise of cardiovascular disease (CVD) over the past 15 yrs has been reported by epidemiologists and international agencies such as world health organization (WHO). It is estimated that by 2020, CVD will be the largest cause of disability and death in India, with 2.6 million Indians predicted to die due to CVD. The risk of CVD accompanying the metabolic syndrome (MetS) is approximately doubled compared with an absence of the syndrome. Term “globesity” is becoming more popular worldwide to describe the epidemic trend towards increased body weight [1].
The Criteria for the metabolic syndrome according to National Cholesterol Education Program, Adult Treatment Panel III
Three or more of the following:
Elevated waist circumference: Men — greater than 40 inches (102 cm).
Women — greater than 35 inches (88 cm).
Elevated triglycerides: Equal to or greater than 150 mg/dL/specific medication.
Reduced HDL (“good”) cholesterol: Men — Less than 40 mg/dL and Women — Less than 50 mg/dL.
levated blood pressure:Equal to or greater than 130/85 mm Hg or use of medication for hypertension.
Elevated fasting glucose: Equal to or greater than 100 mg/dL (5.6 mmol/L) or use of medication for hyperglycemia.
Obesity is a state of excess adipose tissue mass. Although not a direct measure of adiposity, the most widely used method to gauge obesity is the body mass index (BMI), which is equal to weight in kg / height in meter [2]. Other approaches to quantifying obesity include anthropometry (skinfold thickness), densitometry (underwater weighing), Computerized Tomography (CT) or MRI, and electrical impedance upper body subcutaneous fat, as estimated by NC confer risk above and beyond visceral abdominal fat. Various studies indicated that NC may be independent correlate of metabolic risk factors beyond BMI and waist circumference [2].Besides, NC is considered an index of upper body obesity and ectioncorrelates positively with changes in systolic and diastolic blood pressure and other components of the metabolic syndrome [3]. The purpose of our study is to determine the reliability of NC as a measure of cardiometabolic risk factors.
Materials and Methods
This Cross sectional study was carried out in patients who attended medicine clinic in a tertiary care KMC hospital of Mangalore Southern India during September 2010 to August 2012. Total 431 patients chosen randomly in which 250 males and 181 females, fulfilling criteria of Males > 35 year and females> 40 year were included. Pregnant females, patients with thyroid disorders, history of previous neck surgery and type I diabetes mellitus were excluded. Detailed history followed by complete physical examination of patients done. All anthropometric measurement were performed among all patients according to WHO guide lines and biochemical parameters to suggest cardio-metabolic risk factors were carried out among all participants after obtaining informed consent. Ethics committee approval from the institutional ethics committee was obtained prior to the study. Statistical analysis done by using Chi-square test and Karl pearson correlation coefficient.
Neck circumference is measured the superior border of the tape measure was placed just below the laryngeal prominence and applied perpendicular to the long axis of the neck [4]. Normal value: In males < 37cms and in females < 34 cms. Waist circumference (WC) is perimeter measured at the approximate midpoint between the lower margin of the last palpable rib and the top of the iliac crest, in standing position after normal expiration. Normal value for Indian male is 85 cms and for Indian female 80 cms.Hip circumference is the perimeter at the level of the greatest posterior protuberance of the gluteals and was measured widest portion of buttocks [5].
Waist to hip ratio calculated and its normal value is 0. 88 for male, 0.81 for female [5]. BMI measured as weight in kg / (height in meter)[2]: normal 18 -24.9kg/m2 [5]. Fasting Lipid profile: Lowdensitylipoprotein,Highdensitylipoprotein,Totalcholestrol,Triglyerides and Fasting blood glucose level were obtained.
Results
Total of 431 patients were studied, of which 250 males and 181 females. 46% of them were belonging to 41-50 year age group, 24% were 51-60 and remaining 30% above 60 years. Among 431 patients, 272 patients had Metabolic syndrome (MetS) according to NCEP, ATP III guidelines [6]. Out of 272 participants with Met S, 172 (58%) patient were males and 100 (42%) were females [Table/Fig-1].
Mean NC among patients with cardio metabolic risk factor was 36.44 cms, whereas those without cardio metabolic risk factor was 34.08 cms. This correlation is statically highly significant [p-value =<0.001], [Table/Fig-2].
Among females with NC is <34cms, 26.9% had MetS, whereas among females with NC ≥34 cms, 71.9% had MetS. Among males with NC<37cms, 50.9% had MetS, whereas among NC≥ 37cms
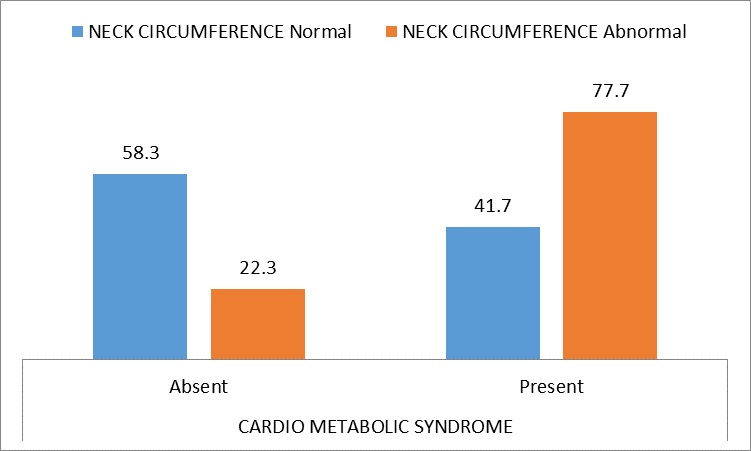
In patient with MetS, 77.7% had increased NC,whereas in those patient without MetS only 22% had abnormal NC. Again this correlation was highly significant [Table/Fig-3].
All individual parameter of cardiometabolic riskfactor i.e. BMI,waist circumference, hip circumference, systolic blood pressure, diastolic blood pressure, FBS, HDL & TG except waist/hip ratio highly significant in patient with abnormal NC when compared with those with normal NC.
Individual parameter of cardio-metabolic risk factor statically correlates with NC except for waist hip ratio [Table/Fig-4].
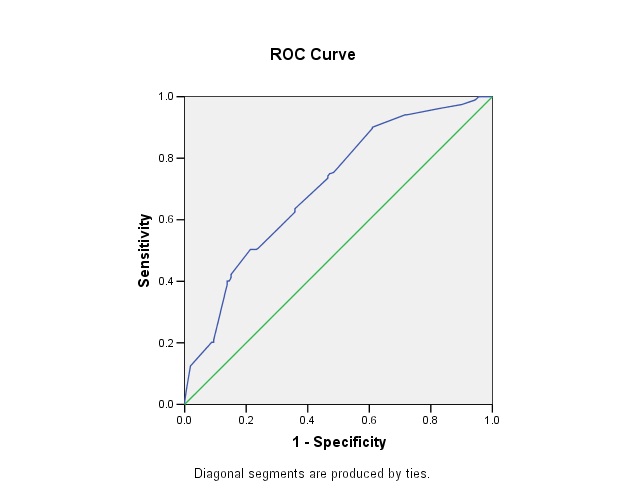
ROC Curve signifies NC with cardio metabolic syndrome with area under the curve is 70% [Table/Fig-5]. In our study for mean neck circumference 36.5cms, sensitivity is 50% and specificity is 76%.
Neck circumference in cardio-metabolic syndrome
| Cardio Metabolic Syndrome | n | Minimum | Maximum | Mean SD | Media | t-value | p- value |
| Absent | 159 | 25 | 41 | 34.08+3.960 | 34.00 | 7.453 | <0.000 |
| Present | 272 | 29 | 42 | 36.44+2.605 | 37.00 | | HS |
| Total | 431 | 25 | 42 | 35.57+3.367 | 36.00 | | |
Sex distribution v/s cardio-metabolic syndrome v/s neck circumference
| Sex | | Cardio Metabolic Syndrome | Total |
| Absent | Present |
| F | Neck Circumference | < 34 | 49 73.1%60.5% | 18 26.9% 18.0% | 67 100.0% 37.0% |
| >= 34 | 32 28.1% 39.5% | 82 71.9% 82.0% | 114 100.0% 63.0% |
| Total | | 81 44.8% 100.0% | 100 55.2% 100.0% | 181 100.0% 100.0% |
| M | Neck Circumference | < 37 | 53 49.1% 67.9% | 55 50.9% 32.0% | 108 100.0% 43.2% |
| >= 37 | 25 17.6% 32.1% | 117 82.4% 68.0% | 142 100.0% 56.8% |
| Total | | 78 31.2% 100.0% | 172 68.8% 100.0% | 250 100.0% 100.0% |
Neck circumference in metabolic syndrome
Neck circumference correlation with cardio-metabolic risk factor
| | | Karl pearson correlation coefficient r-value | p-value |
| Neck circumference | BMI | .492(**) | <0.001 |
| WAIST | .453(**) | <0.001 |
| HIP | .458(**) | <0.001 |
| W/H RATIO | -.005 | .912 |
| SBP | 243(**) | <0.001 |
| DBP | .107(*) | .027 |
| FBS | .166(**) | <0.001 |
| TC | .266(**) | <0.001 |
| LDL | .344(**) | <0.001 |
| HDL | -.173(**) | <0.001 |
| Triglyceride | .280(**) | <0.001 |
| Age | .029 | .544 |
ROC (Receiver Output Curve) analysis curve signifies neck circumference
Comparison of our study with previously conducted studies
| | Our study | Sarah Rosner Preis et al.,study[8] | S Kumar, A Gupta, S Jainstudy [7] |
| Study population | 431 | 3307 | 203 |
| Sex distribution | M:58%, F:42% | M:52%, F:48% | M:60%, F:40% |
| Mean Neck circumference | 36.5cm | 37.3cm | 33.3cm |
| BMI | 25.4kg/m2 | 27.8kg/m2 | 24.2kg/m2 |
| Lab parameter included in study | HDL,TG, LDL, total cholesterol, FBS | HDL, TG, LDL, FBS, insulin, proinsulin HOMA | FBS |
| Radiological parameter | Nil | Multi detected computerized tomography for visceral adipose tissue measurement | Nil |
| Positive correlation of NC | Significant correlation with all anthropometric measurement and lab parameter except for W:H ratio | significant correlation with all anthropometric measurement, lab parameter and VAT | significant correlation with all anthropometric measurement |
Discussion
We hypothesized that NC could be a predictor MetS in Indian population. In this study, we looked into the association between neck circumference and cardio-metabolic risk factor, whether neck circumference independently contribute to cardio-metabolic risk and that higher values of NC has any association with higher prevalence of cardiovascular risk factors.We also observed neck circumference was more strongly associated with adverse risk factor levels in women compared with men.
In our study we have taken NC, waist circumference, hip circumference, W/H ratio, BMI by calculating height and weight and blood pressure, laboratory value including fasting lipid profile (TG, HDL, LDL, TC) and FBS. In study done by Sunil Kumar et al., [7], all anthropometric measurements (weight, height, and NC) and blood pressure were performed and laboratory value FBS, lipid profile not performed due to in all patient. In the Framingham Heart Study [8] with arthropometric (weight, height, and NC, WC,HC, W/H ratio, BMI) and laboratory parameter HDL,LDL,TG,FBS,insulin, proinsulin and homeostasis model assessment of insulin resistance (HOMA-IR), imaging multi detected computerised tomography used in measuring visceral adipose tissue.
In our study MetS present in 272 participant according to criteria of NCEP: ATP111 2001 [6]. In which female were 100, 82 of them had NC more than 34cm, only 18 of them had NC less than 34 cm. In male 172 had MetS of which 117 i.e. 68% had NC more than 37cm and 55 i.e. 32% had NC less than 37cm. So NC with MetS was more correlating with female than with male.
NC is also related to cardiovascular risk factors in severely obese men and women. In our study NC, positively correlates with BMI and mean BMI for our study with metabolic syndrome is 25.4 kg/ m2, mean NC is 36.44cm, p-value is <0.001 with NC this value are statistically significant [Table/Fig-1].
In a first cross sectional study by Ben-Noun et al., [9-12] which was done to identify overweight or obese patients solely by measuring the circumference of the neck, observed that NC >37cm for men and >34cm for women were the best cutoff levels for determining the subjects with BMI >25.0 kg/m2 using the receiver output curve analysis. In our study we also observed same characteristics as NC 37 cm for men and 34 cm for women identified subjects with BMI >25.0 kg/m2 with 75% to 86% sensitivity for men and 63% to 93% for women, 80% to 90% specificity for men and 80% to 100% for women.
We found that neck circumference have positive correlation with systolic and diastolic blood pressure, t-value for systolic and diastolic blood pressure are 8.256 and 5.247, both p-value < 0.000. Ben Noun et al.,[9-12] observed relationship between changes in neck circumference and changes in blood pressure. They found that changes in systolic BP and diastolic BP correlated positively with changes in NC and other components of the metabolic syndrome.
Neck circumference were correlated with various metabolic parameter like LDL, HDL, TC, TG and FBS, t-value were 6.898, 8.472, 6.025, 9.071 & 5.160. P-value <0.001 of all these were statically significant correlations. For all risk factors,women exhibited a larger effect size in risk factor levels per SD increment in neck circumference than men. This finding can be explained by differences in bodily structures between men and women especially in India. It seems, therefore, that with an increase in NC, the likelihood of risk factors for cardiovascular disease also increases.
Our observations indicate that NC as an index of upper body fat distribution can be used to identify cardio-metabolic syndrome. In India study about neck circumference as a measure of cardiometabolic syndrome has not been done. In contrast measurement of NC is a simple, time saving, and least invasive measurement tool. Comparison of our study with previously conducted studies [Table/Fig-6].
Limitations
Since our study was a hospital based study, results may overestimate the true correlation between NC and cardio metabolic syndrome. Neck circumference is a proxy for upper-body fat; we did not have radiographic measures to directly quantify this fat deposition. Other variables such as heart variability, plasma insulin, leptin, interleukin-6, C-reactive protein, and urinary excretion of cortisol and catecholamines metabolites, which can be increased in the metabolic syndrome, were not examined in the present study. Rare endocrine disorders like Cushing’s and other obesity associated syndrome evaluation also remains a limitation of our study. However, further studies are needed to examine the relationship between neck circumference and cardio metabolic risk factor in form measurement of visceral fat tissue.
Conclusion
Patients with NC >37cm for men and >34cm for women are more prone for cardio metabolic syndrome and require additional evaluation.Men with NC <37cm and women with NC <34cm are not to be considered less prone for cardio metabolic syndrome.NC may be used as a simple, cost effective and time-saving screening measure to identify cardio metabolic risk factors in patients.
[1]. Alberti KGMM, Zimmet P, Shaw J, Metabolic syndrome—a new world-wide definition.A Consensus Statement from the International Diabetes FederationDiabetic Medicine 2006 23(5):469-80. [Google Scholar]
[2]. A Onat, G Hergençd, H Yu¨ksel, G Can, E Ayhan, Z Kaya, Neck circumference as a measure of central obesity: Associations with metabolic syndrome and obstructive sleep apnea syndrome beyond waist circumference.Clinical Nutrition 2009 28:46-51. [Google Scholar]
[3]. Jing-ya Zhou, GeHui Ming-fan ZHU, Li-jun Wang, Li Chen, Yao-zong Tan, Neck Circumference as an Independent Predictive Contributor to Cardio-Metabolic SyndromeCardiovascular Diabetology 2013 12(76) [Google Scholar]
[4]. LL Ben-Noun, A Laor, Relationship between changes in neck circumference and cardiovascular risk factors.Exp Clin Cardiol 2006 11(1):14-20. [Google Scholar]
[5]. Physical status: the use and interpretation of anthropometry. Report of a WHO Expert CommitteeWorld Health Organ Tech Rep Ser 1995 854:1-452. [Google Scholar]
[6]. Expert Panel on Detection, Evaluation, and Treatment of High Blood Cholesterol In Adults 2001 Executive Summary of the Third Report of the National Cholesterol Education Program (NCEP) Expert Panel on Detection, Evaluation, and Treatment of High Blood Cholesterol In Adults (Adult Treatment Panel III).JAMA 2011 285:2486-97. [Google Scholar]
[7]. S Kumar, A Gupta, S Jain, Neck circumference as a predictor of obesity and overweight in rural central India.Int. J. Med. Public health 2012 2(1):62-6. [Google Scholar]
[8]. PS Rosner, JM Massaro, U Hoffmann, D’Agostino RBS, Levy D, Sander J R, et al. Neck Circumference as a Novel Measure of Cardiometabolic Risk: The Framingham Heart Study.J Clin Endocrinol Metab 2010 95(8):3701-10. [Google Scholar]
[9]. LL Ben-Noun, A Laor, Relationship between changes in neck circumfer¬ence and changes in blood pressureAm J Hypertens 2004 17:409-14. [Google Scholar]
[10]. LL Ben-Noun, A Laor, Relationship of neck circumference to cardiovascular risk factors.Obes Res 2003 11:226-31. [Google Scholar]
[11]. LL Ben-Noun, A Laor, Relationship between changes in neck circumference and cardiovascular risk factors.Exp Clin Cardol. 2006 11:14-20. [Google Scholar]
[12]. LL Ben-Noun, E Sohar, A Laor, Neck circumference as a simple screening measure for identifying overweight and obese patientsObes Res 2001 9:470-77. [Google Scholar]