Granulocytic Sarcoma with Compressive Myelopathy: A Rare Presentation of Chronic Myelogenous Leukemia
Abhijeet P. Ganapule1, Auro Viswabandya2, Anita Jasper3, Palak Patel4, Gautami Kokil5
1Assistant Professor, Department of Haematology, Christian Medical College and Hospital, Vellore, Tamil Nadu, India.
2Professor, Department of Haematology, Christian Medical College and Hospital, Vellore, Tamil Nadu, India.
3Assistant Professor, Department of Radiology, Christian Medical College and Hospital, Vellore, Tamil Nadu, India.
4Assistant Professor, Department of Pathology, Christian Medical College and Hospital, Vellore, Tamil Nadu, India.
5Fellow In Haematopathology, Department of Pathology, Christian Medical College and Hospital, Vellore, Tamil Nadu, India.
NAME, ADDRESS, E-MAIL ID OF THE CORRESPONDING AUTHOR: Dr. Abhijeet P. Ganapule, Assistant Professor, Department of Haematology, Ida Scudder R oad, Christian Medical College and Hospital Vellore-632004, Tamil Nadu, India.
Phone: 0416-2286095,
E-mail: abhiganapule@gmail.com
Granulocytic sarcoma occurs most commonly in acute myelogenous leukemia. The appearance of granulocytic sarcoma in chronic myelogenous leukemia signals accelerated phase/ blast transformation. This is a rare case of undiagnosed chronic myelogenous leukemia with granulocytic sarcoma causing cord compression, which went into tumour lysis syndrome requiring dialysis after starting of steroids and radiotherapy. A 43-year-old male presented in emergency department with acute onset of flaccid paralysis. On clinical examination, there was hepatosplenomegaly and lower motor neuron paralysis in the lower limbs. The peripheral smear was consistent with chronic myelogenous leukemia in chronic phase. The MRI spine revealed para-spinal and epidural masses causing cord compression and the biopsy from the paraspinal mass was consistent with granulocytic sarcoma.
Cord compression, Granulocytic sarcoma, Tumour lysis syndrome
Case Report
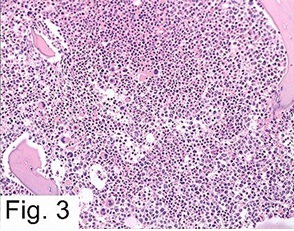
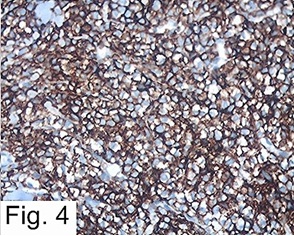
A 43-years-old male presented with a history of progressive back pain for last 4 days unrelieved by analgesics. He noticed progressive unsteady gait for two days and sudden onset of paraplegia on the day of admission. On clinical examination there was liver of 2cm and spleen of 10cm. Neurological examination showed flaccid paralysis of lower limb with bladder and bowel involvement. MRI spine showed para-vertebral soft tissue lesions at multiple levels, largest being on the right side at T6-T8 level [Table/Fig-1]. Epidural soft tissue component at the T9-11 level compressing and displacing the cord to the left side was associated with cord oedema [Table/Fig-2]. The biopsy from the paraspinal mass was composed of immature cells with round to irregular nuclei, fine chromatin and inconspicuous nucleoli, with moderate amount of eosinophilic cytoplasm. Few eosinophilic myelocytes were also seen. There is high endothelial venular proliferation. The immunohistochemistry on the malignant cells were as follows MPO+, CD 43+, CD20-, CD3-, focally positive CD 34 and MIB-75% [Table/Fig-3,4] The examination of the peripheral count revealed a leukocyte count of 2,52,600/mm3 with neutrophils- 58%, promyelocytes- 2%, myelocytes- 13%, metamyelocytes- 10%, band forms- 11%, basophils- 2%, eosinophils- 3%, blasts- 1% with 2 nucleated RBCs/100 WBCs. Hemoglobin was 11.6 grams/dl and the platelet count was 166,000/mm3. This profile was consistent with chronic myelogenous leukemia in chronic phase. The bone marrow aspiration done was consistent with chronic myeloid leukemia in chronic phase. The Fluorescent in Situ Hybridization was positive for BCR-ABL fusion (98% positive), reverse transcriptase polymerase chain reaction showed b3 a2 transcript and conventional cytogenetics revealled 46, XY, t(9;22) (q34;q11.2) (20). He was started on allopurinol, sodabicarbonate, dexamethasone and cytoreductive doses of hydroxyurea. He received 30 gray RT in 10 fractions for reduction of the cord compression due to tumour. He went into tumour lysis syndrome (TLS) following steroids and radiotherapy with biochemical parameters as follows calcium-7mg/dl, phosphorus-6 mg/dl, creatinine 2.7mg/dl, potassium-6 mille-equivalent/liter. He required one sitting of dialysis on second day of starting the therapy following which the tumour lysis settled. The paraparesis recovered over next five weeks and currently he has lower limb power of 5/5.
He was later initiated on Imatinib and two months on treatment has achieved complete hematological response.
T2-weighted coronal image through the lower thoracic and lumbar spine showing T2 hyperintense right paravertebral soft tissue (thin white arrows) at T6-8 level
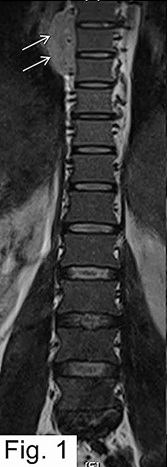
T2-weighted sagittal image of the lower thoracic and lumbar spine shows diffusely hypointense marrow signal (hollow white arrows). Hyperintense soft tissue (thin white arrows) in the posterior epidural space compresses the lower thoracic cord at T10-12 level with swelling and hyperintensity of the cord extending from T9 upto the conus (solid white arrows)

Haematoxylin and Eosin (20X) section of tissue showing monotonous population of malignant cells [
Immunohistochemistry showing CD43 positive cells in tissue at 40 X
Paraplegia due to GS of the spine at the initial manifestation of undiagnosed CML
| Reference | Year Reported | Patient age/gender | Tumor location | Length of survival |
| Present case | 2013 | 43/M | T6-T8 Paravertebral mass | 3 months alive on follow |
| | | | T9-11 Epidural mass | |
| Barbara Bryant et al.,[1] | 2006 | 53/F | T4-T6 | 4 months |
| Widhyde et al.,[2] | 1963 | 12/F | T6 | 8 months |
| Rand and Rand et al.,[3] | 1960 | 6/F | T1-T5 | 5 months |
| Critchley and Greenfield et al.,[4] | 1930 | 14/M | T2, T7 | 4 months |
Discussion
Chronic myeloid leukemia in chronic phase (CML-CP) presenting with compressive myelopathy is very rare [1-4].Here, we report a patient with chronic myeloid leukemia in chronic phase (CML-CP) who presented with compressive myelopathy due to spinal granulocytic sarcoma (GS). Malignant spinal cord compression (MSCC) is an uncommon event occurring in cancer patients with cumulative incidence of 2.5% during the course of the disease [5]. The commonest tumour associated with MSCC is multiple myeloma with the incidence being 1.95% [5]. MSCC is a rare event in leukemia with cumulative incidence of 0.3% along the course of the disease [5].Acute myeloid leukemia rarely presenting as GS causing cord compression has reported in literature [6,7]. There have been only four case reports of CML presenting as paraplegia at presentation due to GS of spine and this probably is the fifth case to the best of our knowledge in literature [1-4] [Table/Fig-5]. Patient with GS in CML have poor prognosis [1-4,8] [Table/Fig-5]. In cases with cord compression related to metastatic deposit, surgical decompression compared to radiotherapy has better chance of achieving ambulation [9]. However, in our case we gave radiotherapy as there were tumour deposits at multiple levels, so surgical decompression was not possible. He responded to radiotherapy and regained his lower limb power, currently is ambulatory with normal bowel, bladder functions. The tumour lysis syndrome requiring dialysis, which occurred post RT and steroids was probably due to steroid responsiveness of the tumour with superadded effect of RT.
Conclusion
Unique features of our case are CML presenting with compressive myelopathy due GS and patient later went into TLS after he was exposed to steroids and RT. While clinically evaluating a case of CML with focal neurological deficit, GS as cause must be kept in differential diagnosis.
[1]. Bryant Barbara J, Alperin Jack, Elghetany M Tarek, Paraplegia as the presenting manifestation of extramedullary megakaryoblastic transformation of previously undiagnosed chronic myeloid leukemia.American Journal of Hematology 2007 82:150-54. [Google Scholar]
[2]. DE Wildhyde, JA Jane, S Mulan, Spinal epidural leukemiaAm J Med 1963 34:281-87. [Google Scholar]
[3]. WR Rand, CW Rand, Intraspinal tumours of childhood. Springfield, IL: Charles C. Thomas. 1960 214 [Google Scholar]
[4]. M Critchely, JG Greenfield, Spinal symptoms in chloroma and leukemiaBrain. 1930 :53-11. [Google Scholar]
[5]. DA Loblow, NJ Laperriere, WJ Mackillop, A population – based study of malignant spinal cord compression in OntarioClin Oncol 2003 15:211-17. [Google Scholar]
[6]. DM Landis, DM Aboulafia, Granulocytic sarcoma: Uncommon complication of aleukemic leukemia causing spinal cord compression. A case report and literature review.Leukemia lymphoma 2003 44:1753-60. [Google Scholar]
[7]. PD Anjaria, UG Gadgil, M Gaikwad, Unusual presentation of acute myeloid leukemia.J Postgrad Med 1976 22:44-6. [Google Scholar]
[8]. TY Lant, DT Lin, HF Tion, Prognostic factor of treatment outcome in patient with granulocytic sarcoma.Acta hematology 2009 122:238-46. [Google Scholar]
[9]. JR Paul Klimo, J Clinton, Thompson Kestle John R.W,, A metanalysis of surgery versus conventional radiotherapy for treatment of metastatic spinal epidural diseaseNeuro-oncology 2005 7(1):64-76. [Google Scholar]