Introduction
Periodontal health is the “sine qua non,” a prerequisite, of successful comprehensive dentistry [1]. To achieve the long-term therapeutic targets of comfort, function, predictable treatment, longevity, and ease of restorative and maintenance care; active periodontal infection must be treated and controlled before the initiation of restorative, esthetic, and implant dentistry. In addition, the residual effects of periodontal disease or anatomic aberrations inconsistent with realizing and maintaining long-term stability must be addressed. More recently, this phase of treatment includes techniques performed in anticipation of esthetic or implant dentistry, such as clinical crown lengthening, covering denuded roots, alveolar ridge retention or augmentation, and implant site development [2].
The treatment plan includes all procedures required for the establishment and maintenance of oral health and involves the following decisions: [3]
Need for emergency treatment (pain, acute infections).
Teeth that will require removal.
Periodontal pocket therapy techniques (Nonsurgical followed by surgical).
Endodontic therapy.
The need for occlusal correction, including orthodontic therapy.
The use of implant therapy.
The need for caries removal and the placement of temporary and final restorations.
Prosthetic replacements that may be needed and which teeth will be abutments if a fixed prosthesis is used.
Decisions regarding esthetic considerations in periodontal therapy.
Sequence of therapy.
Unforeseen developments during treatment may necessitate modification of the initial treatment plan. However, except for emergencies, no therapy should be initiated until a treatment plan has been established [3].
Several Models were developed for Periodontal Treatment planning within the context of comprehensive dental treatment plans. We will discuss below two of the most well known models and develop a new treatment model that best fits the goals and sequence of periodontal treatment.
Model 1 of Periodontal Treatment Planning: (Lindhe Textbook): [4]
In this model, treatment is undergone in four phases:
Systemic phase of therapy including smoking counseling
Initial (or hygiene) phase of periodontal therapy, i.e. cause-related therapy
Corrective phase of therapy, i.e. additional measures such as periodontal surgery, and/or endodontic therapy, implant surgery, restorative, orthodontic and/or prosthetic treatment
Maintenance phase (care), i.e. supportive periodontal therapy (SPT).
Model 2 of Periodontal Treatment Planning (Carranza Textbook): [5]
In this model, treatment is divided into the following phases as detailed below:
Preliminary Phase
(a) Treatment of emergencies:
Dental or periapical
Periodontal
Other
(b) Extraction of hopeless teeth and provisional replacement if needed (may be postponed to a more convenient time)
Nonsurgical Phase (Phase I Therapy)
(a) Plaque control and patient education:
Diet control (in patients with rampant caries)
Removal of calculus and root planing
Correction of restorative and prosthetic irritation factors
Excavation of caries and restoration (temporary or final, depending on whether a definitive prognosis for the tooth has been determined and the location of caries)
Antimicrobial therapy (local or systemic)
Occlusal therapy
Minor orthodontic movement
Provisional splinting and prosthesis
Evaluation of Response to Nonsurgical Phase, Rechecking
Pocket depth and gingival inflammation
Plaque and calculus, caries
Surgical Phase (Phase II Therapy)
(a) Periodontal therapy, including placement of implants
(b) Endodontic therapy
Restorative Phase (Phase III Therapy)
(a) Final restorations
(b) Fixed and removable prosthodontic appliances
(c) Evaluation of response to restorative procedures
In this second model, the sequence in which these phases of therapy are performed may vary to some extent in response to the requirements of the case. However, the preferred sequence, which covers the vast majority of cases, is non-linear [5].
Although, the phases of treatment in this model have been numbered, the recommended sequence does not follow the numbers. Phase I, or the nonsurgical phase,is directed to the elimination of the aetiologic factors of gingival and periodontal diseases. When successfully performed, this phase stops the progression of dental and periodontal disease [6]. Immediately after completion of phase I therapy, the patient should be placed on the maintenance phase (phase IV) to preserve the results obtained and prevent any further deterioration and recurrence of disease. While on the maintenance phase, with its periodic evaluation, the patient enters into the surgical phase (phase II) and the restorative phase(phase III) of treatment. These phases include periodontal surgery to treat and improve the condition of the periodontal and surrounding tissues. This may include regeneration of the gingiva and bone for function and aesthetics, placement of implants, and restorative therapy [7].
The Trimeric Model of Periodontal Treatment Planning
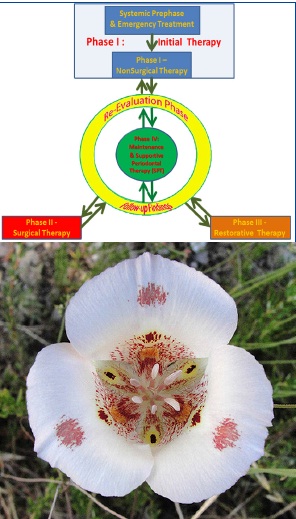
The model we introduce in this article, called the Trimeric Model due to the arrangement of treatment steps that resembles the petals of a trimeric flower e.g. Mariposa Lilly, introduce a modification of the second model of periodontal treatment planning in which periodontal treatment is done in stages (phases) that are ended with, centered, and aimed towards the maintenance phase (Phase IV) which is the final aim that the patient will be placed in for lifetime.Each phase is followed by a Re-evaluation Phase in which decision of the next step of treatment is made. This model is presented in [Table/Fig-1] and explained below:
a. The trimeric model of periodontal treatment planning. b. Mariposa lily a trimeric flower [8].
Phase I (Initial Therapy – Disease Control Phase)
Initial therapy or phase I is the first step in the sequence of procedures that constitute periodontal treatment.
The objective of initial therapy is the reduction or elimination of gingival inflammation. This is achieved by complete removal of all factors responsible for gingival inflammation such as plaque, calculus, correction of defective restorations, restoration of carious lesions, etc.
As Emergency treatment is the first treatment done for those needing it, some may separate a systemic prephase prior to this Phase and keep Phase I Periodontal Therapy as solely a Nonsurgical Therapy (Scaling and Root Planing) only.
Initial Therapy involves the following procedures:
1. Treatment of Emergencies
Emergency treatment is the first priority for any dental patient in need of it. This includes extracting or root canal treating infected or abscessed teeth, treatment of periodontal abscesses, or beginning root canal treatment of Endo-Perio Lesions. This may include antimicrobial therapy.
2. Antimicrobial therapy
Antimicrobial therapy is used mostly locally in periodontics. This includes mouthwashes and local delivery of antimicrobials into the periodontal pockets. Rarely, we may need systemic antibiotic treatment in case of specific microbial infections (as streptococcal mucositis, herpes gingivostomatitis, and candidiasis) and infections with systemic involvement.
3. Diet Control
Dietary deficiencies (as Iron or Zinc Deficiencies, folate deficiency, or Vitamin Deficiencies B12, C or D) should be addressed and corrected from the start of periodontal treatment. This might include referral to general or specialized physician or a dietician.
Serious systemic diseases as Diabetes may be discovered in the periodontal clinic, and such patients should be referred to the appropriate physician and a dietician. We should be well versed on these aspects of medicine and diet therapy to guide our patients to appropriate treatment and explain to them how these treatments are integral to their periodontal treatment.
4. Patient Education and motivation
Treatment plan should be understood by the patient before the active treatment is initiated and the dentist should teach the patient how to do oral hygiene measures. The patient should understand from the beginning of treatment that the responsibility of maintaining his teeth is primarily his or hers.
5. Correction of Iatrogenic Factors
Few exceptions; rough, over-contoured, over-hanging, or subgingivally located Restorations, Removable or fixed Prosthesis and Orthodontic Appliances may be associated with pronounced accumulation of plaque and periodontal inflammation.
Like calculus, such restorations or appliances interfere with efficient plaque control and must be corrected or removed to allow for reduction or elimination of gingival inflammation.
6. Deep Caries
Carious lesions should be excavated and temporary restorations placed. Caries in the vicinity of the gingiva interferes with plaque removal and consequently with gingival health. And Exposed teeth should be treated. Endodontics for Infected teeth should be started in this phase.
7. Hopeless Teeth
If some teeth have been diagnosed as “hopeless” and they are not in a strategic or vital position for temporary maintenance of occlusal relations, such teeth should be extracted at this time. Partially impacted third molars with communication to the oral cavity should also be extracted.
8. Preliminary Scaling
The next step should be gross scaling and polishing of the teeth, followed by specific instruction in oral hygiene.
9. Temporary Splinting, occlusal adjustment, and minor orthodontic tooth movement
Although temporary splinting for mobile teeth has not proved to be useful in promoting periodontal healing during therapy, It may facilitate treatment procedures as scaling, occlusal therapy, and surgical periodontal therapy. Heavy contact on mobile teeth should be reduced or orthodontic tooth movement should be done to correct it.
10. Scaling and Root Planing
Fine scaling and root planning are necessary to eliminate irritation from subgingival calculus and contaminated cementum.
Re-evaluation Phase:
In the trimeric model, re-evaulation is a transitional step that needs to be done between every phase of the Treatment plan and the other. It is usually done after 3-6 weeks from initial therapy. It includes:
Re-evaluation of the results of initial therapy (extent of improvement in pocket depths and attachment level for the whole periodontium).
Re-evaluation of oral hygiene status and affirming Oral Hygiene instruction if needed.
Measuring Bleeding and Plaque score and checking for improvement.
Review of the Diagnosis and prognosis and modification of the whole treatment plan if needed.
Re-evaluation should be done after 3-6 weeks of Surgical and Restorative Therapy and is the most important phase in the treatment plan as the major decisions during treatment are made in it.
Phase II (Surgical Therapy)
During the evaluation of Phase I, evaluate the need of the periodontium for surgery. Surgery may be indicated in the following cases: [9].
Pocket management in specific situations. The most popular traditional indication is the presence of pockets of ≥5mm.
Irregular bony contours or deep craters.
Areas of suspected incomplete removal of local deposits.
Degree II and III furcation involvements.
Distal areas of last molars with expected mucogingival problems.
Persistent inflammation.
Root coverage.
Removal of gingival enlargements.
Phase III (Restorative Therapy)
In which Restoration of the defects with fixed or removable prosthodontics, Periodontal Prosthesis, or other kinds of restorations are done.
Phase IV (Maintenance Phase - Supportive Periodontal Therapy):
Preservation of the periodontal health of the treated patient is as important as the elimination of periodontal disease. In the maintenance phase, patients are placed on a schedule of periodic recall visits for maintenance care to prevent recurrence of the disease. The intervals between recall appointments are varied according to the patient condition.
This should be the end goal of periodontal treatment. The long-term success of periodontal treatment depends on the maintenance of the results achieved in the other phases of the periodontal treatment plan. This mandates a lifelong relation between the patient and the treating dentist or periodontist.
Advantages of the Trimeric Model of Periodontal Treatment planning:
Introduces a logical, easy to remember order of the steps of treatment of periodontal disease.
Making maintenance phase in the center of the treatment plan clearly establishes it as the goal of periodontal treatment that should be reached after completion of the necessary treatments.
Clearly indicates the necessity of reevaluation between the treatment phases to check the improvement of the periodontal condition after each treatment phase and revise the overall treatment plan accordingly.
The Extended Trimeric Model
The trimeric model of periodontal treatment planning can be extended by including the preparation of the periodontium for restorative dentistry and Adjunctive Orthodontic Therapy.This extended trimeric periodontal treatment planning model adds the following two aspects to the original Trimeric model:
1. The Expansion of the Surgical Phase
Surgical Procedures could be divided into two major types:
Periodontal Surgery: Surgeries to control active periodontal disease. E.g. pocket reduction surgeries.
Preprosthetic Surgery: Surgeries to prepare for the Restorative Phase. E.g. crown lengthening surgery, root coverage surgery.
2. Adjunctive Orthodontic Therapy
Orthodontic treatment has been shown to be a useful adjunctive to periodontal therapy [10–13]. It has a unique position in the periodontal treatment plan, as it should be undertaken only after active periodontal disease has been controlled. The following considerations should be kept in mind on attempting orthodontic treatment for periodontal patients [14]:
As long as they are periodontally healthy, teeth with pre-existing bone loss may be moved orthodontically without incurring additional attachment loss [15,16].
Failure to control active periodontitis can result in acute exacerbations and bone loss during tooth movement [17].
If nonsurgical treatment is sufficient to control active periodontal disease, definitive surgical periodontal pocket therapy may be postponed until after the completion of orthodontic tooth movement. In this way, positive bone changes that may happen during orthodontic therapy can be utilized to improve the periodontal bone defects.
However, deep pockets and furcation invasions may require surgical access for root instrumentation in advance of orthodontic tooth movement (periodontal surgery as defined above).
Soft tissue grafting procedures are often indicated in anticipation of orthodontic therapy to increase the dimension of attached tissue (preprosthetic surgery as defined above) [18].
As a result of the above considerations, adjunctive orthodontic therapy is placed separately and in close association with the surgical therapy Phase (Phase II) where some surgical procedures may precede it while other surgical procedures should be done after its completion.
The Extended Trimeric Model Diagram
The Extended trimeric model of periodontal treatment planning is illustrated in [Table/Fig-2].
The extended trimeric model with the steps arranged in clockwise manner and with the multidisciplinary nature of the treatment of dental and periodontal treatment emphasized
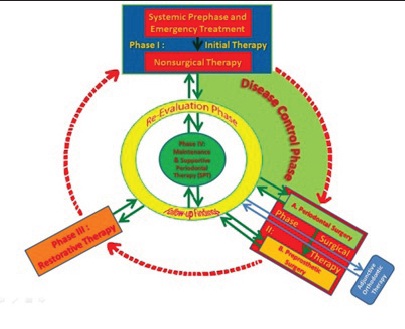
Note the following in the above figure of the extended Trimeric model of periodontal Treatment planning:
The broken red arrows doesn’t indicate jumping from a stage to the next stage but only the logical order of treatment phases as re-evaluation phase should be reached between each phase and the other with transfer to maintenance phase (and thus finishing the treatment) once treatment objectives are accomplished even if the phases of treatment are not all done.
The green highlighting indicate the disease control phase which includes the initial phase and part of the surgical phase (specifically periodontal surgery) but not adjunctive Orthodontic therapy.
Advantages of the Extended Trimeric Treatment plan model:
Introduces a clear and logical framework of the steps of treatment of periodontal disease.
Clarifies the stabilization (Disease Control) stage of periodontal therapy as not all surgical procedures are needed for stabilization of periodontal disease and as other procedures are clearly indicated for the preparation to restorative therapy.
Indicates the placement of adjunctive orthodontic therapy after the stabilization of periodontal infection and before any restorative or surgical preparation to restorative therapy.
[1]. Kramer JM, Nevins M, Int J PeriodontRestor Dent. 1981; 1:4.(editorial). In: Newman MG, Takie HH, Klokkevold PR, Carranza FACarranza’s Clinical Periodontology 2012 Ed 11St. LouisSaunders Elsevier:608 [Google Scholar]
[2]. Newman MG, Takie HH, Klokkevold PR, Carranza FA, Carranza’s Clinical Periodontology 2012 Ed 11St. LouisSaunders Elsevier:608 [Google Scholar]
[3]. Newman MG, Takie HH, Klokkevold PR, Carranza FA, Carranza’s Clinical Periodontology 2012 Ed 11St. LouisSaunders Elsevier:384 [Google Scholar]
[4]. Lindhe J, Lang NP, Karring T, Clinical Periodontology and Implant Dentistry 2008 655 Vol 2Ed 5OxfordBlackwell [Google Scholar]
[5]. Newman MG, Takie HH, Klokkevold PR, Carranza FA, Carranza’s Clinical Periodontology 2012 Ed 11St. LouisSaunders ElsevierFigure 34-1, Preferred sequence of periodontal therapy; p. 386 [Google Scholar]
[6]. Newman MG, Takie HH, Klokkevold PR, Carranza FA, Carranza’s Clinical Periodontology 2012 Ed 11St. LouisSaunders Elsevier:386 [Google Scholar]
[7]. Newman MG, Takie HH, Klokkevold PR, Carranza FA, Carranza’s Clinical Periodontology 2012 Ed 11St. LouisSaunders Elsevier:385 [Google Scholar]
[8]. Image retrieved from:https://www.flickr.com/photos/11563230@N04/4700136544 in april, 30. 2014 [Google Scholar]
[9]. Newman MG, Takie HH, Klokkevold PR, Carranza FA, Carranza’s Clinical Periodontology 2012 Ed 11St. LouisSaunders Elsevier:514 [Google Scholar]
[10]. Brown SI, The effect of orthodontic therapy on certain types of periodontal defects. I. Clinical findingsJ Periodontol 1973 44:742 [Google Scholar]
[11]. Ingber JS, Forced eruption. Part I. A method of treating isolated one and two wall infrabony osseous defects: rationale and case report. J Periodontol 1974; 45:199. In: Lindhe J, Lang NP, Karring TClinical Periodontology and Implant Dentistry 2008 Ed 5OxfordBlackwell [Google Scholar]
[12]. Ingber JS, Forced eruption. Part II. A method of treating non-restorable teeth: periodontal and restorative considerations. J Periodontol. 1976; 47:203. In: Lindhe J, Lang NP, Karring TClinical Periodontology and Implant Dentistry 2008 Ed 5OxfordBlackwell [Google Scholar]
[13]. Kokich VG, Esthetics: the orthodontic-periodontic restorative connection.SeminOrthodont 1996; 2:21. In: Lindhe J, Lang NP, Karring TClinical Periodontology and Implant Dentistry 2008 Ed 5OxfordBlackwell [Google Scholar]
[14]. Newman MG, Takie HH, Klokkevold PR, Carranza FA, Carranza’s Clinical Periodontology 2012 Ed 11St. LouisSaunders Elsevier:385online material of chapter 65 [Google Scholar]
[15]. Polson AM, Reed BE, Long-term effects of orthodontic treatment on crestal bone levels. J Periodontol. 1984; 55:28. In: Lindhe J, Lang NP, Karring TClinical Periodontology and Implant Dentistry 2008 Ed 5OxfordBlackwell [Google Scholar]
[16]. Polson AM, Caton J, Polson A, Periodontal response to tooth movement into intrabony defects. J Periodontol. 1984; 55:197. In: Lindhe J, Lang NP, Karring TClinical Periodontology and Implant Dentistry 2008 Ed 5OxfordBlackwell [Google Scholar]
[17]. Folio J, Rams TE, Keyes PH, Orthodontic therapy in patients with juvenile periodontitis: clinical and microbiological effects. Am J Orthodont. 1985; 87:421. In: Lindhe J, Lang NP, Karring TClinical Periodontology and Implant Dentistry 2008 Ed 5OxfordBlackwell [Google Scholar]
[18]. Wennström JL, Mucogingival therapy.In Proceedings of the World Workshop on Periodontics. Ann Periodontol. 1996; 1:671. In: Lindhe J, Lang NP, Karring TClinical Periodontology and Implant Dentistry 2008 Ed 5OxfordBlackwell [Google Scholar]