Introduction: Impacted teeth present a very common problem in dentistry due to the variable numbers of problems they cause. They have previously been imaged by radiography which is very inaccurate. Dental CT is an upcoming modality which very accurately images the teeth.
Aim: The aim of our study was to compare the efficacy of Dental CT with radiography in assessing the morphology of the impacted tooth and its relation to adjacent structures.
Materials and Methods: We conducted a hospital based prospective study in which all patients with impacted teeth who underwent Dental CT and Radiographic evaluation were evaluated.
Results: The morphology of all the teeth was well visualized on CT. Resorption of adjacent tooth was missed in 7 teeth by radiography. In a significant number of cases (10/30) the relation of the impacted tooth with the mandibular canal could not be visualized on the radiographs.
Conclusion: We concluded that Dental CT yields markedly better information than radiographs regarding impacted teeth with respect to divergence of the roots, relation of the impacted tooth with the adjacent tooth, nasal floor, maxillary sinus and mandibular canal. However, Dental CT was found to be only marginally better than Radiographs for assessment of number of roots, inclination of the impacted tooth and relation of the tooth with alveolar crest. Dental CT was also proved to be an indispensable diagnostic tool for the determination of the buccolingual inclination and relationsof the impacted tooth.
Introduction
An impacted tooth is incapable of fully erupting into the oral cavity, as a result of obstruction by another tooth. It may be a source of recurrent odontogenic pain, infection, and inflam mation and may require orthodontic or surgical treatment [1]. It often presents a problem in orthodontics and surgery with respect to the degree of displacement, position and inclination of the long axis of the tooth and its relation with adjacent structures [2].
Earlier, the maxillofacial region was assessed by plain radiography or tomography. Radiographic imaging was difficult because of the curved configuration of the jaws and also because radiographs are a two dimensional image of a three dimensional object. The use of such radiographs cannot always precisely determine the true morphology and relationship of an object in all dimensions, or overcome the misleading effect of superimposition [3]. However, the advent of Dentascan (Dental CT) is changing the imaging trends.
Unlike the previous imaging techniques, the oblique saggital view permits the evaluation of distinctly buccal and lingual cortical bone margins, as well as clear visualization of the internal structures [4].
As previously noted in previous studies [5], Dental CT offers superb visualization of impacted teeth and can help the clinician to plan his treatment preoperatively or prior to orthodontic therapy. The position of the tooth within the alveolar crest as well as the relation to surrounding structures is clearly visualized. Resorption of adjacent roots and hooks, in particular are easily detected and quantified by Dental CT. It has been demonstrated that the morphology of crown and root, number of roots and their divergences are poorly shown on plain film radiographs but are clearly demonstrated on CT scans. The buccolingual inclination of the long axis of the impacted tooth, dilacerations which is an angulation between the root and the crown are undetected on the plain film radiographs, whereas Dental CT clearly shows those anomalies [3].
The aim of our study was to compare the efficacy of Dental CT with radiography in assessing the morphology of the impacted tooth and its relation to adjacent structures.
Materials and Methods
We conducted a hospital based prospective study in the Department of Radiodiagnosis and Imaging in Kasturba Medical College, Manipal. All patients with impacted teeth who underwent Dental CT and Radiographic evaluation (Orthopantomogram / Intraoral Periapical view) were included in the study.
Dental radiography was performed in the Oral Medicine and Radiology Department – Orthopantomogram or Intraoral Periapical views. CT scan was done using Phillips - Brilliance 64 slice CT scanner. Informed consent was obtained from every patient undergoing the CT scan. The radiation dose was minimised by using lead aprons for the patients, by using bony algorithm for the scans and keeping a small field of view. Multiplanar reconstructions using Dentascan software were done on the workstation of Phillips - Brilliance 64 Multislice scanner. A planning line was drawn manually along the centerline of the jaw arch which formed the base for subsequent orthoradial and panoramic reconstructions. The orthoradial 2reconstructions were calculated perpendicular to the planning line and the panoramic reconstructions were calculated parallel to the planning line[Table/Fig-1,2,3,4,5and6]. The following parameters were then analysed on both Radiographs and Dental CT.
Morphology of the tooth – It was graded as follows:
Well visualized – When all the four borders of the tooth were visualized.
Poorly visualized – When 2- 3 borders of the tooth were visualized.
Not visualized – When </= 1 borders of the tooth was visualized.
Number of roots – This was reported as:
Not visualized – Unable to see how many roots.
How many roots – One, two or three
Divergence of roots – This was classified as:
Not visualized – When the divergence of roots could not be made out.
Divergent – When the tip of the roots were pointing away from each other.
Not divergent – When the tip of the roots were pointing towards each other.
Dilaceration – When there was hooking / angulation of the root.
Poorly visualized – When the inclination could not be made out.
Inclination of roots – These were of the following types:
Mesioangular – Oblique position of the tooth with crown pointing mesially.
Distoangular – Oblique position of the tooth with crown pointing distally.
Horizontal – Tooth lying horizontal to the plane of the jaw.
Vertical – Tooth lying perpendicular to the plane of the jaw.
Relation with adjacent structures – These were graded as:
Not visualized – When the relation could not be made out (due to bony overlap / obliquity of the tooth).
No contact – When the tooth outline was > 3mm away from the adjacent structure (Not touching the adjacent structure).
Doubtful contact – When the tooth outline was <3mm away from the adjacent structure but not touching the outline of the structure.
Direct contact – When the tooth outline was touching the outline of the adjacent structure but not seen beyond the limit of the adjacent structure..
Encroachment – When the tooth outline was seen beyond the limit of the adjacent structure..
Statistical Analysis
All the relevant data was entered into SPSS 11.5 data sheet for statistical calculation. Weighted Kappa values (which are a measure of observer agreement) were calculated using the Stata 10 and SPSS 11.5 software. Observer agreement can provide a general estimate of the value of an imaging technique when imaging provides the best evidence of abnormality or even if an independent method for obtaining proof exists, it may be difficult to use. The guidelines for strength of agreement as determined by Kappa values were followed as indicated in previous studies [6] [Table/Fig-7]. Similar Kappa values for comparing findings of Radiography and surgery for impacted teeth have been used previously [7]. All Kappa values obtained were statistically significant (p-value <0.005).
Results
We studied 37 impacted teeth in 26 patients. All the patients were in the age group of 11 – 50 years with mean age of 24 years. Minimum age was 19-years and maximum age was 45-years. The majority of the teeth were mandibular - 78%, whereas 22% were maxillary. The third molar was the most commonly involved tooth (n=32) followed by canines (n=4) and 1 premolar.
The morphology of all the teeth was well visualized on CT, 4 of which were not visualized on radiographs and 29 were poorly visualized.
With respect to comparison of number of roots seen on radiographs and CT, a kappa value of 63% was obtained. Hence the findings on 3radiographs were in substantial agreement with CT with respect to number of roots.
Radiographs could not identify the dilacerations which were picked up on CT (in 11 teeth). The inclination of only 1 tooth was poorly visualized on Radiograph which showed vertical impaction on CT. The inclination of the rest of the teeth was correctly visualized on the radiographs.
There were no cases with doubtful contact of the impacted tooth with the adjacent tooth on CT. The relation of 6 out of 37 teeth was not visualized on Radiographs and another 6 showed doubtful contact, resorption of adjacent tooth was missed in 7 teeth by radiography.
The relation of all 5 central maxillary teeth with the nasal floor could not be visualized on radiograph which was clearly seen on CT. Relation with the floor of the maxillary sinus was not visualized in 5 out of the 7 peripheral maxillary teeth on radiograph. In a significant number of cases (10/30) the relation of the impacted tooth with the mandibular canal could not be visualized on the radiographs. The relation of the impacted tooth with alveolar crest could not be visualized on radiograph in 8 out of 37 cases. The relation was visualized in all cases on CT.
Buccolingual inclination / buccolingual relations of the impacted tooth could not be assessed in any of the radiographs but could be accurately and easily determined on Dental CT. Hence this variable could not be compared in the two modalities.
Discussion
Impacted teeth are one of the growing concerns in dentistry. Exact localization of impacted teeth is necessary to remove them, if needed, with minimal removal of healthy bone, thus minimizing iatrogenic trauma [8]. It is important for surgeons and orthodontists to define the position and inclination of the longitudinal axis of the tooth and its distance to adjacent structures. In our study, CT scored far better than radiography and proved to be an important one stop diagnostic tool for management of impacted teeth.
In our study, the morphology of all the impacted teeth was well visualized on CT. We determined that the agreement between radiographs and CT with respect to morphology of impacted teeth is only slight, as determined by weighted Kappa values. We thus concluded that CT is considerably better that radiographs for demonstration of morphology of impacted tooth. Our findings were in conjunction with previous studies[3], where it was observed that morphology of the crown and root were poorly shown on plain film radiographs but were clearly demonstrated on Dental CT. It has also been observed previously[9] that the image quality with respect to fine dental and bony structures were better with Dental CT.
In our study, in only 4 of the cases, the number of roots could not be visualized on radiographs. When we compared the number of roots on radiographs and CT, Dentascan was found to be only marginally better than Radiographs as validated by a kappa value of 63%. The findings on radiographs were in substantial agreement with CT with respect to number of roots. The past studies [3] have also observed that the number of roots was poorly shown on plain film radiographs but were clearly demonstrated on Dental CT. However, in our study, the findings on radiographs regarding the number of roots were in accordance with that on CT. Hence, we concluded that radiographs were good enough as far as number of roots were concerned and CT did not have much of an added advantage over radiographs with respect to determining the number of roots. CT is useful only in doubtful cases when one of the roots is small and radiolucent as compared to the others.
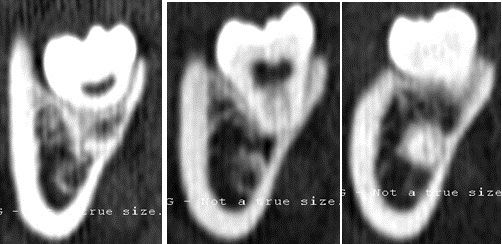
In our study, dental CT was found to be better than Radiography regarding divergence of roots which was accounted for by a kappa value of 28%, indicating only fair agreement between radiographs and CT. The radiographs could not identify the dilacerations which were picked up on CT & yielded poor information as compared to CT with respect to divergence of roots. The analysis of divergence of the roots needs good resolution since a short tip of the root maybe curved as in dilaceration [Table/Fig-8] which may be difficult to determine on Radiographs. CT shows excellent visualization of the roots hence providing a big advantage over radiographs. Our findings were in agreement with previous authors[3] who observed that dilaceration of the tooth was undetected on plain film radiographs and clearly shown on dental CT.
The inclination of only 1 tooth was poorly visualized on radiograph which showed vertical impaction on CT. The inclination of the rest of the teeth was correctly visualized on the radiographs. We found that Dental CT was only marginally better than Radiographs regarding inclination of the impacted tooth as verified by a Kappa value of 84 % which indicated almost perfect agreement between the two modalities. Previous studies [10] also showed that the inclination of the impacted teeth showed the same result in radiographs and Dental CT. This is because inclination of the tooth is determined in the mesiodistal plane and can thus be easily demonstrated by orthopantomograms. In a similar study conducted in the past [5], it was found that the axis of the displaced teeth was distoangular in 17 cases, mesioangular in 13 cases, and without inclination in six cases. Mesioangular inclination (17 out of 37) was most commonly encountered in our study as compared to the previous study [5].
In our study, there were no cases with doubtful contact with adjacent tooth on CT. The 6 teeth which showed doubtful contact on radiographs could be accurately put into the class of no contact or direct contact. Dental CT was found to be appreciably better than radiographs concerning relation with the adjacent tooth as proved by a kappa value of 34 % which showed that the agreement between radiographs and CT with respect to relation with the adjacent tooth is only fair agreement. It has also been observed earlier [3]that the relation of the impacted tooth with the adjacent structures was poorly delineated by plain film radiographs, whereas dental CT provided this information with greater clarity. CT yields better results for possible root resorption than does Radiography because of the exact proportional cross-sectional scans. Root resorption caused by impacted and displaced teeth can thus be diagnosed more precisely, a fact which may have therapeutic consequences [Table/Fig-9,10]. One of the previous studies [10] had also concluded that doubtful root resorption could be excluded with a significantly better accuracy with CT than with radiography. Another study [9] has also mentioned that Dental CT should be preferred whenever the depiction and precise assessment of fine dental structures are required, for instance, when assessing root resorption.
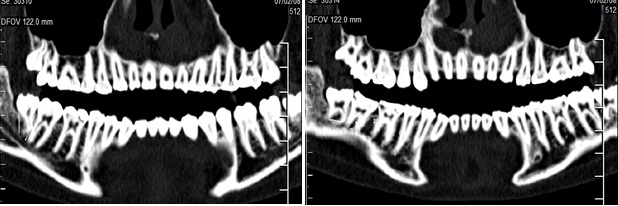
The relation of all 5 central maxillary teeth with the nasal floor could not be visualized on radiographs and was clearly seen on CT. This is due to the fact that superimposition of structures in Radiographs in the maxillary tooth obscures its relation with the nasal floor [Table/Fig-11,12]. Relation with the floor of the maxillary sinus was not visualized in 5 out of the 7 peripheral maxillary teeth on radiograph. In our study we found that Dental CT was notably better than Radiography for relation with the floor of the maxillary sinus for peripheral maxillary teeth as denoted by a kappa value of 37% which suggested only fair agreement between radiographs and CT.
Sinus disease could not be visualized in any of the 7 maxillary teeth. This was because we used only dental radiographs, that is, orthopantomograms and intraoral periapical views. For determination of sinus disease, additional radiograph is needed, whereas dental CT served as a one stop modality for assessment of all the regions. Even after the additional radiograph, sinus disease may not be accurately determined, which is very essential for the management.
The present study shows that dental CT is significantly better than Radiography as regards to relation of the impacted tooth with mandibular canal. This was denoted by a kappa value of 36% which showed only fair agreement of radiographs with CT findings. In a significant number of cases (10/30) the relation of the impacted tooth with the canal could not be visualized on the radiographs. CT yields better results for relation of the impacted tooth with the mandibular canal than does radiography because these scans can be reformatted in three planes, providing the buccolingual relation as well which cannot be determined on radiographs [Table/Fig-13,14]. One of the previous studies which was carried out to study the different methods for determining the relationship between the mandibular canal and impacted third molars and found that 61% of the surgeons considered Dental CT as the ideal radiographic method in this aspect [11]. Another author [12] has also reported in the past that radiography is not an adequate screening method for predicting inferior alveolar nerve paresthesia after extraction of impacted molar.
The relation of the impacted tooth with alveolar crest could not be visualized on Radiograph in only 8 out of 37 cases. The relation was visualized in all cases on CT. A Kappa value of 61% showed moderate agreement of radiographs with CT with regard to relation of the tooth with alveolar crest. Thus, CT was found to be only slightly better than radiographs in this aspect. The Intraoral periapical views can well delineate the relation of the tooth with alveolar crest.
Buccolingual inclination / buccolingual relations of the impacted tooth could not be assessed in any of the radiographs but could be accurately determined on dental CT. Hence this variable could not be compared in the two modalities. We concluded that CT is an indispensable modality for the determination of the buccolingual inclination and relations of the tooth [Table/Fig-15].
Axial CT scans of maxilla shows prescribed curve from which reformatted images will be derived
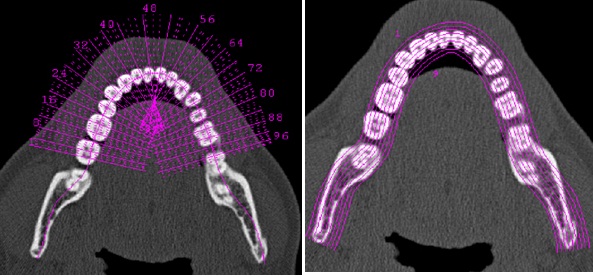
Orthoradial reconstructions calculated perpendicular to the planning line
Panoramic reconstructions calculated parallel to the planning line
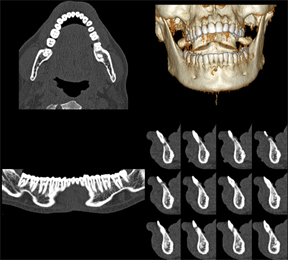
mage plate showing all the Dental CT planes along with volume rendered image
Guidelines for strength of agreement indicated with kappa values
| Feature of impacted tooth studied | Kappa value obtained (in %) | Strength of agreement between CT and Radiography |
| Morphology | 13 | Slight |
| Number of roots | 63 | Substantial |
| Divergence of roots | 28 | Fair |
| Inclination of tooth | 84 | Almost perfect |
| Relation with adjacent tooth | 34 | Fair |
| Relation with floor of maxillary sinus | 37 | Fair |
| Relation with mandibular canal | 36 | Fair |
| Relation with the alveolar crest | 61 | Moderate |
Panoramic view shows dilaceration of upper right third molar.

Radiograph showing impacted third molar impinging on the distal root of second molar with doubtful resorption of second molar. Position of the mandibular canal cannot be visualized

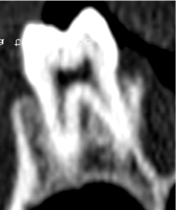
Panoramic CT view clearly showing resorption of adjacent tooth.
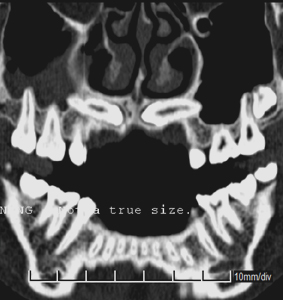
Panoramic dental CT views showing bilateral impacted maxillary cannines. Encroaching into sinus floor, direct contact with floor of nasal cavity on the left side, sinus disease present on the left side
Volume rendered image showing bilateral impacted maxillary cannines

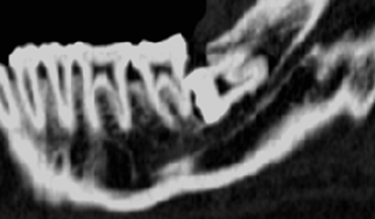
Panoramic & Orthoradial CT views showing clearly no contact with mandibular canal
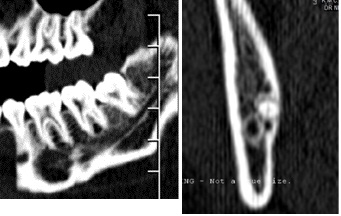
Orthoradial CT image clearly showing buccal and lingual aspects of tooth
Conclusion
Dental CT yields markedly better information than radiographs regarding impacted teeth with respect to divergence of the roots, relation of the impacted tooth with the adjacent tooth, nasal floor, maxillary sinus and mandibular canal. However, Dental CT was found to be only marginally better than Radiographs for assessment of number of roots, inclination of the impacted tooth and relation of the tooth with alveolar crest. Dental CT was also proved to be an indispensable diagnostic tool for the determination of the buccolingual inclination and relations of the impacted tooth. Dental CT served as a one stop modality for the evaluation of impacted tooth as it showed sinus disease as well along with the above mentioned findings. This study has shown the capabilities of Dental CT as an indispensable imaging tool for Dentistry.
[1]. H Meir, Scheinfeld Shifteh Keivan, L Laura, Avery Dym Harry, Teeth: What Radiologists should knowRadiographics. 2012 32:1927-44. [Google Scholar]
[2]. Abrahams James J, Dental CT Imaging: A Look at the Jaw.Radiology. 2001 219:334-45. [Google Scholar]
[3]. Bodner Lipa, Sarnat Haim, Bar-Ziv Jacob, Kaffe Israel, Computed tomography in the management of impacted teeth in children.Journal of Dentistry for Children 1994 370(77) [Google Scholar]
[4]. Chandel Siddhartha, Agrawal Amiya, Singh Nishi, Singhal Ankita, Dentascan: A Diagnostic BoonJournal Of Dental Sciences And Research 2013 4(1) [Google Scholar]
[5]. Gahleitner Andre, Watzek G, Imhof H, Dental CT: imaging technique, anatomy, and pathologic conditions of the jawsEur Radiol 2003 13:366-76. [Google Scholar]
[6]. Kundel Harold L, Polansky Marcia, Measurement of Observer AgreementRadiology. 2003 228:303-38. [Google Scholar]
[7]. Ezoddini Ardakani F, Zangouie Booshehri M, Navab Azam A, Fotoohi Ardakani F, Diagnostic accuracy of panoramic radiography in determining the position of impacted third molars in relation to the inferior dental canal compared with surgeryIran J Radiol 2010 7(2):91-96. [Google Scholar]
[8]. Haris PS, Balan A, Importance of localization of impacted teethDentomaxillofacial Radiology 2007 36:372-73. [Google Scholar]
[9]. Hofmann Elisabeth, Medelnik Jürgen, Fink Martin, Lell Michael, Hirschfelder Ursula, Three-dimensional volume tomographic study of the imaging accuracy of impacted teeth: MSCT and CBCT comparison—an in vitro studyEur J Orthod. 2013 35(3):286-94.(doi:10.1093/ejo/cjr030). [Google Scholar]
[10]. Krennmair G, Lenglinger FX, Traxier M, Imaging of unerupted and displaced teeth by cross sectional CT scansInternational Journal of Oral & Maxillofacial Surgery 1995 24:413-15. [Google Scholar]
[11]. B Koong, MJ Pharoah, M Bulsara, M Tennant, Methods of determining the relationship of the mandibular canal and third molars: a survey of Australian oral and maxillofacial surgeons.Aust Dent J. 2006 51(1):64-68. [Google Scholar]
[12]. J Szalma, E Lempel, S Jeges, G Szabó, L Olasz, The prognostic value of panoramic radiography of inferior alveolar nerve damage after mandibular third molar removal: retrospective study of 400 cases.Oral Surg Oral Med Oral Pathol Oral Radiol Endod. 2010 109(2):294-302. [Google Scholar]