Basal Cell Carcinoma Arising within Seborrheic Keratosis
Recep Bedir1, Cüneyt Yurdakul2, Hasan Güçer3, Ibrahim Sehitoglu4
1Medical Faculty, Department of Pathology, Recep Tayyip Erdogan University, Rize, Turkey.
2Medical Faculty, Department of Pathology, Recep Tayyip Erdogan University, Rize, Turkey.
3Medical Faculty, Department of Pathology, Recep Tayyip Erdogan University, Rize, Turkey.
4Medical Faculty, Department of Pathology, Recep Tayyip Erdogan University, Rize, Turkey.
NAME, ADDRESS, E-MAIL ID OF THE CORRESPONDING AUTHOR: Dr. Recep Bedir, Assistant Professor, Department of Pathology, Recep Tayyip Erdogan University School of Medicine, Rize, Turkey. Telephone: +90 464.2130491, Fax : + 90 464 2170364,
E-mail: bedirrecep@gmail.com , Mobil Tlf: +90 5057331695
Malignant tumour development within a seborrheic keratosis (SK) is extremely rare. Though the most commonly developed malignant tumour is the basal cell carcinoma (BCC), other tumour types have also been reported in literature. Herein, we will report a superficial type BCC case developed within SK localized in hairy skin of a 78-year-old female patient. In immunohistochemical evaluation, diffuse positive staining with CK19 and over-expression in p53 compared with non-neoplastic areas were determined in neoplastic basaloid islands. It is always not easy to differentiate especially superficial type BCC cases from non-neoplastic epithelium of SK with histopathological evaluation. As far as this reason we believe that in difficult differentiation of these 2 lesions, in order to show the differentiation in basal epithelium, immunohistochemical evaluation may be helpful.
Immunohistochemistry, Seborrheic keratosis, Skin cancer
Case Report
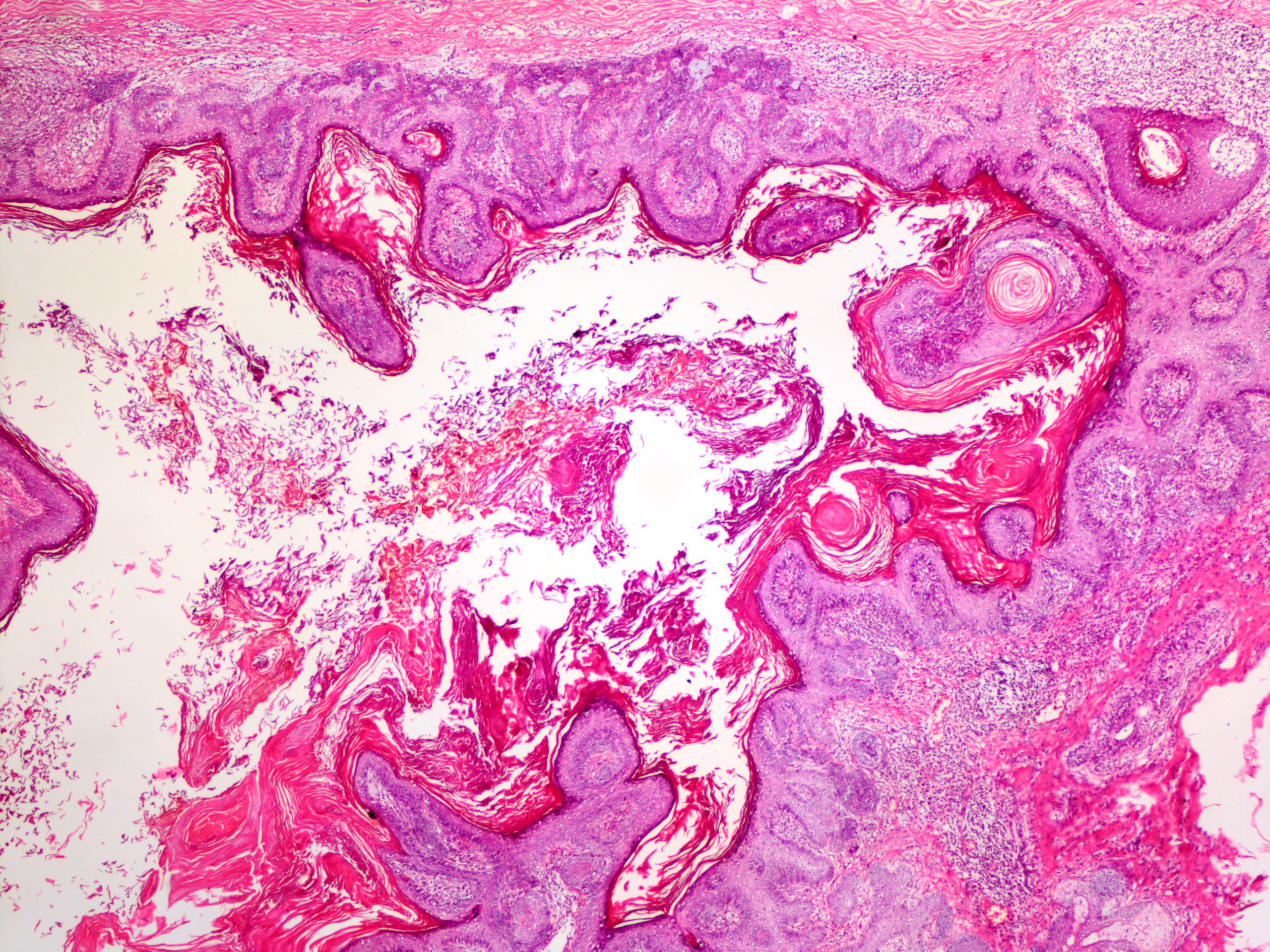
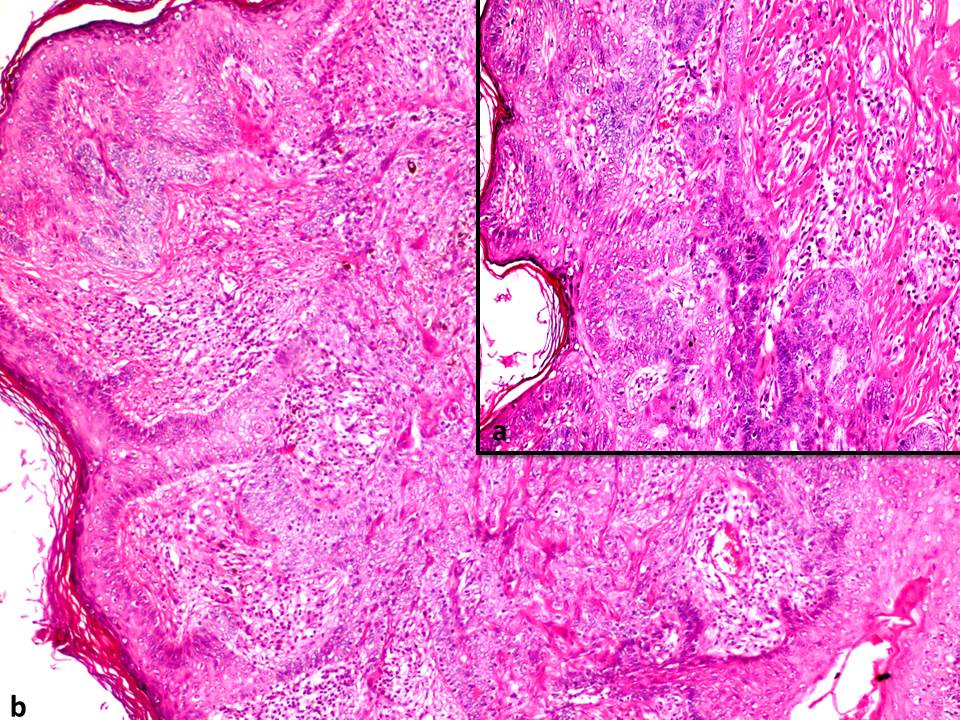
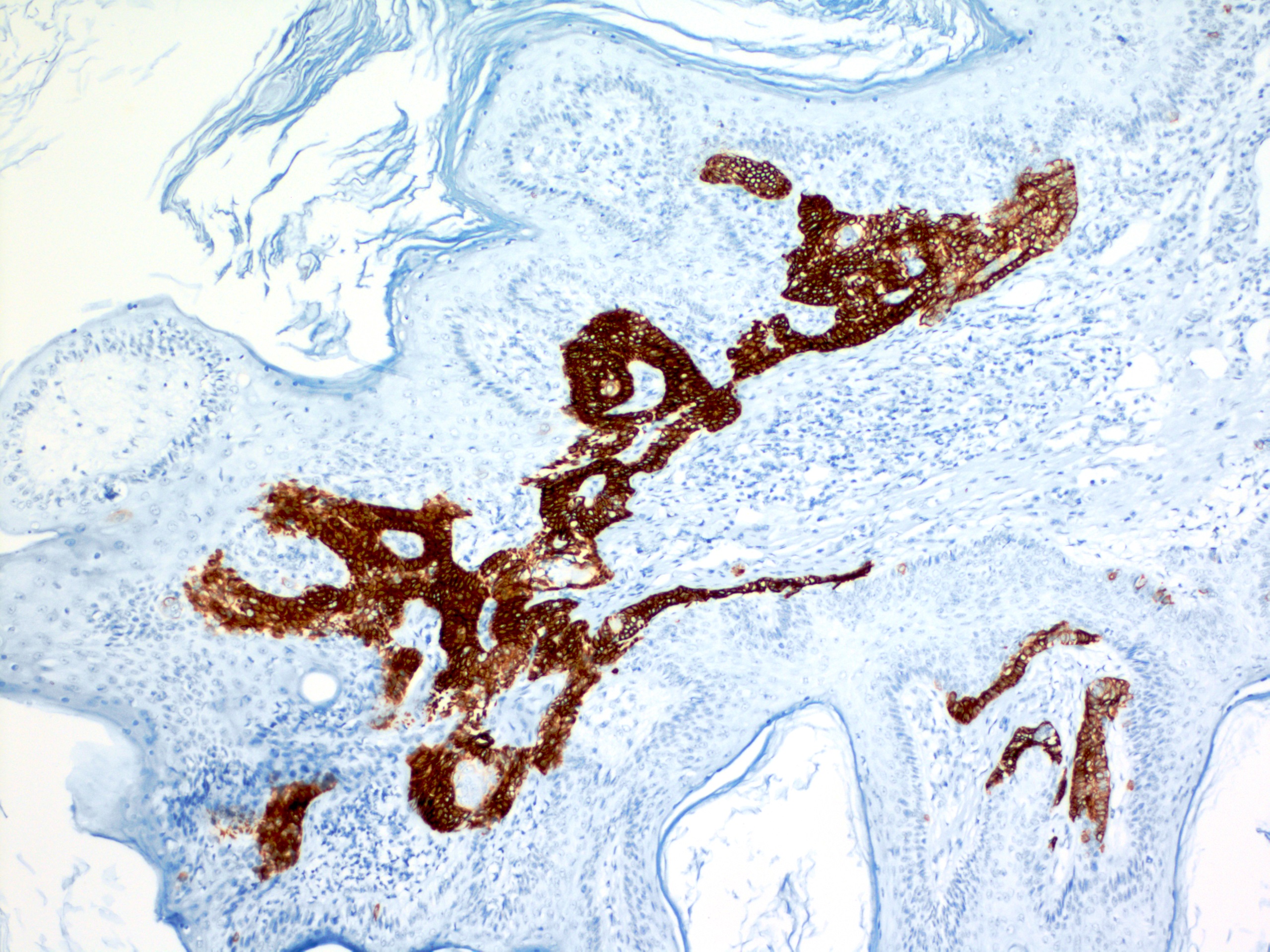
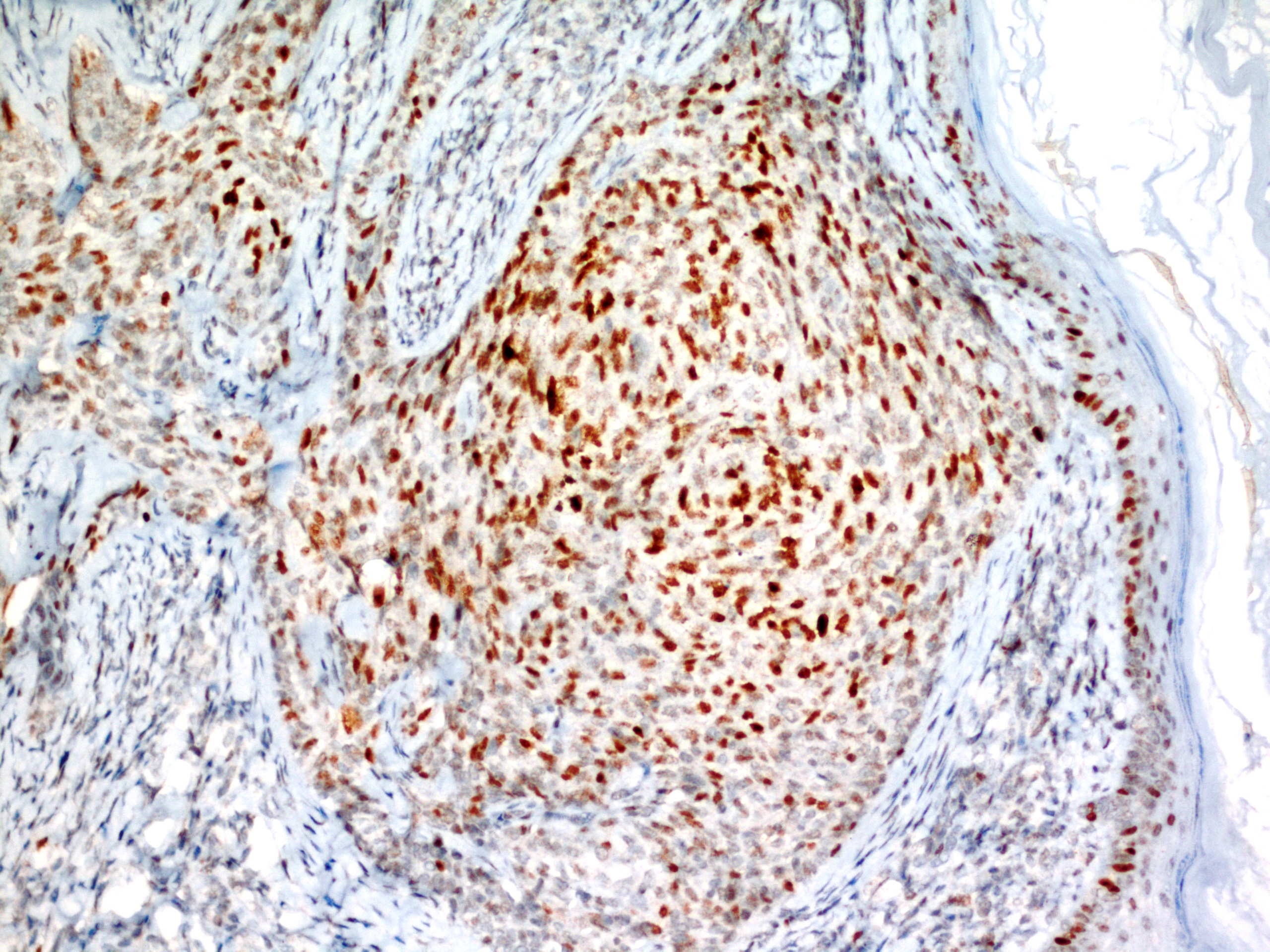
A 78-year-old female patient was admitted with flat, brown, warty lesion on hairy skin of her occipital region. This lesion was present for 10-years but slowly enlarging in last months. In physical examination a brown plaque with a 20 x 15 mm diameter, slightly elevated from skin was observed. The clinical differential diagnosis considered an irritated SK a pigmented BCC or a malignant melanoma. The lesion was totally excised by the plastic surgeon. In microscopic evaluation, there was marked hyperkeratosis and proliferation in basaloid cells in lower layers of epidermis showing acanthosis and containing pseudohorn cysts [Table/Fig-1]. In many foci, proliferation of peripherally palisading basaloid cells through papillary dermis was observed [Table/Fig-2]. In immunohistochemical evaluation, a strong positive staining with CK19 was determined in basaloid cells area [Table/Fig-3]. The p53 staining was established in basaloid islands more than non-neoplastic epithelium [Table/Fig-4]. With its morphological and immunohistochemical features; the lesion was reported as superficial type BCC arising within SK. There was no tumour identified in surgical borders. In two months follow up of the patient, recurrence was not observed.
Discussion
Seborrheic keratosis (SK) is one of the most common benign skin tumours. On the other hand, basal cell carcinoma (BCC) is the most common malignancy of the skin. Determination of a malignant tumour within SK is an extremely rare condition [1]. Seborrheic keratosis, one of the most common epidermal tumours, is frequently encountered in clinical practice. It is most commonly localized in head and neck region followed by body, upper and lower extremities [1,2]. Although malignant transformation is rare, malignant melanoma, eccrin porocarcinoma, and microinvasive squamous cell carcinoma cases within SK were also reported in the literature [3-5]. In a large, retrospective study of Lim et al., [2] on 639 cases, another lesion accompanying seborrheic keratosis was determined in 85 of the cases. These concomitant lesions included premalignant lesions, malignancies, melanocytic lesions and miscellaneous lesions. Miscellaneous lesions consisted of haemangiomas, fibroepithelial polyps, chondrodermatitis nodularis helices and keratoacanthoma. In that study, there were four cases reported with malignant transformation within SK; two of which were BCC, one was invasive squamous cell carcinoma and one was superficially spreading malignant melanoma. Seborrhoeic keratosis are composed of several cell types, the transformation to a variety of epithelial tumours derived from similar cell types could occur. Therefore, basal cell carcinomas could arise from basaloid cells, squamous cell carcinomas arise from squamous cells, and melanomas arise from melanocytes all within the seborrhoeic keratosis [2]. The most common malignant neoplasm reported within SK is the BCC, while the most common histological type is the superficial type, as in our case [1,2].
Ultraviolet light is a known risk factor for some malignant epithelial neoplasms such as basal cell carcinoma, squamous cell carcinoma and malignant melanoma [6]. Although the exact cause of malignant transformation within SK is not known, a prolonged sunlight and/or low-dose chronic ionized radiation exposures were suggested to be the reason [6,7].
Tumour arising within a SK is not easy to diagnose with a punch biopsy. For that reason, to determine the changes in lesion, complete excision or at least taking a biopsy larger than 1cm has been advised [8].
BCC is considered to originate from follicular germinative cells. In some immunohistochemical studies, the probable origin of BCC was determined as outer root sheath of hair follicles [9]. On the other hand, SK is thought to be a benign skin-appendage tumour especially resulting from follicular differentiation in follicular infundibula. For that reason, Cascajo et al., [10] speculated that there may be a pathogenic association in between BCC and SK owing to their common follicular origin. They supposed that the nomenclature as collision tumour is not reasonable because it is unknown whether the association of seborrheic keratosis with malignant neoplasms is a random event or whether there is, in fact, a pathogenic relationship in the development of two distinctive neoplasms together. Therefore, the term compound tumour is suggested to designate the finding of two distinctive neoplasms either directly contiguous with each other or immediately adjacent to each other [10]. Akasaka and Kon. [11] suggested that both basal cell carcinomas and seborrheic keratosis may be derived from a similar source pluripotential cells of either the epidermis or hair follicle epithelium. However, the immunohistochemical features of SK and BCC are different. Ishida et al., [1] used CK17, CK19, SOX9 and p53 in differentiation of neoplastic and nonneoplastic basaloid cells in an immunohistochemical evaluation of a case. In this evaluation; it has been determined that CK17, CK19 and SOX9 were expressed in BCC but not in SK. Then again p53 was established to be over-expressed in BCC but not determined in SK. In the light of all these data, they have suggested that, BCC does not directly originate from SK but arises within that nest. Similarly, in our case report there was CK19 expression in BCC but any staining was not determined in non-neoplastic SK areas. There was also p53 over-expression observed in BCC.
Seborrheic keratosis showing hyperkeratosis, acanthosis and papillomatosis (HE, x40)
Immature basaloid cell groups showing peripheral palisading through the basal layer of epidermis (a) and proliferating through upper dermis within SK (b) (HE, x200)
Diffuse positive staining of BCC and negative staining of SK with CK19 (Immunostaining, x100)
Positive nuclear staining on basaloid cell groups with p53 (Immunostaining, x200)
Conclusion
Sometimes it may be difficult to differentiate non-neoplastic basaloid cell proliferations from especially small foci of superficial type basal cell carcinoma. In those cases, we believe that using CK19 and p53 may be helpful in confirmation of superficial BCC diagnosis.
Conflicts of Interest
No potential conflict of interest relevant to this article was reported.
[1]. M Ishida, N Ohsato, H Okabe, Basal cell carcinoma arising within a seborrheic keratosis with respect to immunohistochemical characteristics.Oncol Lett. 2011 2:625-27. [Google Scholar]
[2]. C Lim, Seborrhoeic keratoses with associated lesions: a retrospective analysis of 85 lesions.Australas J Dermatol. 2006 47:109-13. [Google Scholar]
[3]. V Madan, NH Cox, M Gangopadhayay, Porocarcinoma arising in a broad clonal seborrhoeic keratosis.Clin Exp Dermatol. 2008 33:350-51. [Google Scholar]
[4]. AJ Birnie, S Varma, A dermatoscopically diagnosed collision tumour: malignant melanoma arising within a seborrhoeic keratosis.Clin Exp Dermatol. 2008 33:512-13. [Google Scholar]
[5]. T Terada, M Kamo, Y Baba, M Sugiura, Microinvasive squamous cell carcinoma arising within seborrheic keratosis.Cutis. 2012 90:176-78. [Google Scholar]
[6]. OS Kwon, EJ Hwang, JH Bae, Seborrheic keratosis in the Korean males: causative role of sunlight.Photodermatol Photoimmunol Photomed. 2003 19:73-80. [Google Scholar]
[7]. SK Suvarna, M Bagary, G Glazer, Radiation-induced squamous carcinoma arising within a seborrhoeic keratosis.Br J Dermatol. 1993 128:443-47. [Google Scholar]
[8]. ME Laing, C O’Keane, GM Murphy, Basal cell carcinoma arising in a seborrhoeic keratosis.Clin Exp Dermatol. 2009 34:e371-72. [Google Scholar]
[9]. M Ishida, R Kushima, H Okabe, Immunohistochemical demonstration of D2-40 in basal cell carcinomas of the skin.J Cutan Pathol. 2008 35:926-30. [Google Scholar]
[10]. CD Cascajo, M Reichel, JL Sanchez, Malignant neoplasms associated with seborrheiic keratoses. An analysis of 54 cases.Am J Dermatopathol. 1996 18:278-82. [Google Scholar]
[11]. T Akasaka, S Kon, Two cases of basal cell carcinoma arising in seborrheic keratosis.J Dermatol. 1997 24:322-27. [Google Scholar]