Laparoscopic Cholecystectomy in Situs Inversus Totalis
Raghuveer MN1, Mahesh Shetty S2, Sunil Kumar BB3
1Postgraduate Student, Department of Surgical Gastroenerology, JSS Medical College and Hospital, Mysore, India.
2Assistant Professor and Head, Department of Surgical Gastroenerology, JSS Medical College and Hospital, Mysore, India.
3Assistant Professor, Department of Surgical Gastroenerology, JSS Medical College and Hospital, Mysore, India.
NAME, ADDRESS, E-MAIL ID OF THE CORRESPONDING AUTHOR: Dr. Raghuveer MN, No. 71, Second Floor,“Sri Rama Complex”, 3rd Cross, D.Devaraj Urs Road Mysore – 570024, Karnataka State, India.
Phone: +919916830019,
E-mail: dr.raghuveermn@gmail.com
Situs inversus totalis is a rare condition where the organs in the body is placed in the opposite side. When such patient presents with the diseases of the intra abdominal organs the diagnosis is challenging and the operative procedure to be performed will be difficult. This may require the anticipation of variations in anatomy, ergonomic changes required during surgery and mastery over the operative skills in reversed anatomy. Cholelithiasis in situs inversus totalis is one such situation. Herein we report a case of situs inversus totalis who underwent successful laparoscopic cholecystectomy for symptomatic gallbladder calculi.
Calot’s triangle, Laparoscopic cholecysytectomy, Situs inversus totalis, Transposition of internal organs
Case Report
A 55-year-old gentleman known case of situs inversus totalis presented with dull aching type of pain in the upper abdomen more in the epigastrium and non radiating. It was associated with fullness of stomach and dyspepsia.
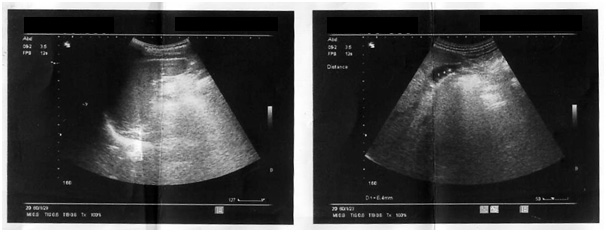
On examination no jaundice or pyrexia was noted. Apex beat was on the right fifth intercostal space in the mid clavicular line. WBC counts and amylase levels were normal. USG abdomen [Table/Fig-1] revealed left sided gallbladder with multiple calculi. There was no evidence of common bile duct or intrahepatic biliary radicals dilatation.
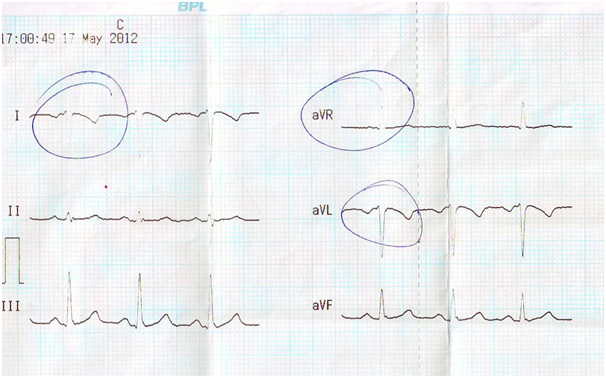
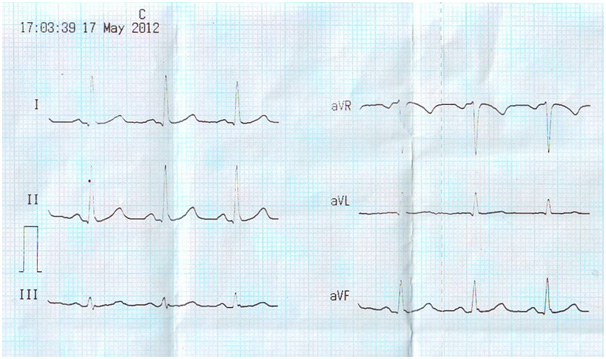
Situs inversus totalis was confirmed with ECG [Table/Fig-2] showing right axis deviation. Global negativity in lead I (a negative P-wave, QRS complex and T-wave). Positively deflected QRS complex in aVR. Negative P-wave in lead II. Reverse R-wave progression in precordial leads.The leads were placed in opposite direction and repeat ECG was obtained[Table/Fig-3].
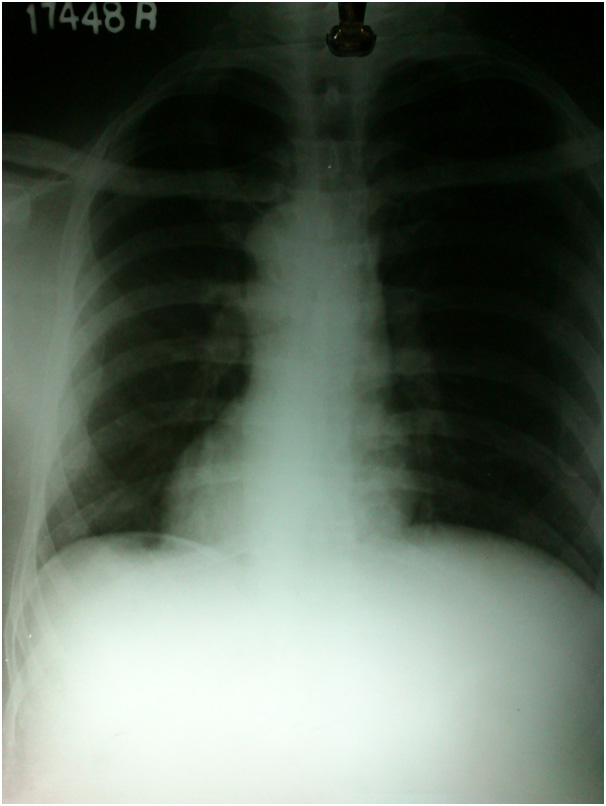
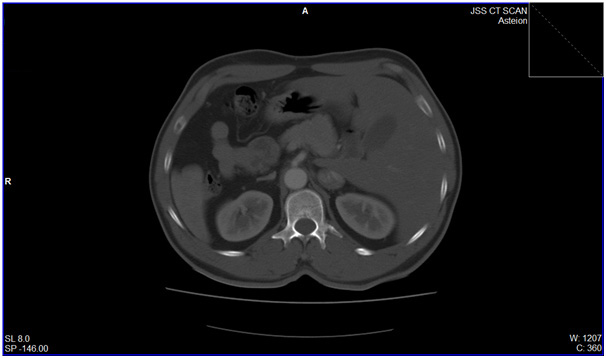
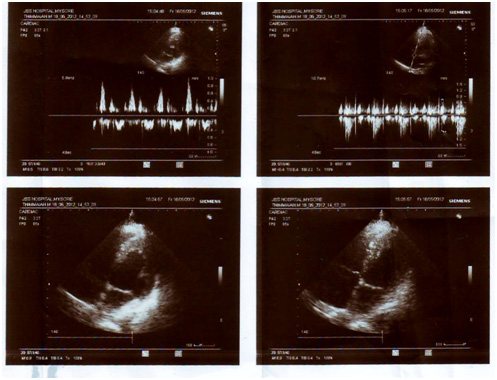
Chest X-Ray [Table/Fig-4], CT Scan [Table/Fig-5] and 2D Echo [Table/Fig-6] confirmed the clinical and ECG diagnosis. The diagnosis of cholelithiasis and situs inversus totalis was made.
There were no comorbid conditions. Laparoscopic cholecystectomy was planned after obtaining a valid informed written consent. The operating set up and the monitor were placed in the direction opposite to conventional surgery. The operating team also changed their positions, primary surgeon and first assistant were standing on the right side and second assistant was standing on the left side.
Under general anaesthesia on insertion of 10mm thirty degree storz system telescope camera all the contents were exactly found on the opposite side [Table/Fig-7],10mm epigastric port was put and two 5mm ports were put in midaxillary and anterior axillary line on left side [Table/Fig-8]. The primary operating surgeon was right handed.
He had to crossover his arms to retract the neck of the gallbladder with left hand and dissect the callot’s with right hand. To prevent this difficulty the first assistant was asked to retract the neck of gallbladder [1] and the primary surgeon dissected out the callots triangle with right hand [1].
Significance of position of surgeon to patient – The surgeon stood to the right of the patient to approach the callot’s triangle easily and the law of triangulation was established. But the dissection had to be done with left hand which was difficult. Dissection of callot’s triangle was also tried from the caudal end [2] with patient in Lloyd davis position but was still uncomfortable so the dissection was continued from right side only.
The common bile duct, cystic duct and cystic artery were identified. There were no structural abnormalities in these structures. The surgery proceeded uneventfully and the gallbladder was extracted through umbilical port. Total time consumed was 2h 15min.
Macroscopically the gallbladder measuring 6cm x 3cm x 2cm was congested oedematous. Cut section revealed partial loss of velvety appearance of mucosa. Multiple pigmented calculi seen in the lumen. Histopathology of sections from the Gallbladder revealed features suggestive of chronic cholecystitis
The patient was discharged on 5th postoperative day. He was given oral antibiotics for three days, NSAIDs for three days and proton pump inhibitors for one month. He was reviewed after one week for suture removal and one month later. The patient was asymptomatic.
Situs inversus totalis was confirmed with ECG showing right axis deviation
ECG obtained after placing the leads exactly in the mirror image of the regular ones
Echocardiogram (2D) revealed dextrocardia and no structural and functional abnormalities in the cardia
A thirty degree storz system 10mm telescope camera in the umbilical region revealed the abdominal contents found on the opposite side

A 10mm epigastric port was put and two 5mm ports were put in midaxillary and anterior axillary line on left side

Previous case reports published on laparoscopic cholecystectomy in situs inversus [3,4]
| S.No | Author | Year | Age in years | Sex | Diagnosis |
| 1 | Campos L | 1991 | 39 | Female | Cholelithiasis |
| 2 | Drover JW | 1992 | 29 | Female | Cholelithiasis |
| 3 | Goh P | 1992 | 62 | Male | Empyema |
| 4 | Huang SM | 1992 | 36 | Male | Cholelithiasis |
| 5 | Lipschutz JH | 1992 | 80 | Male | Cholelithiaisis choledocholithiasis |
| 6 | Takei HT | 1992 | 51 | Female | Cholelithiasis |
| 7 | Schiffino L | 1993 | 53 | Female | Cholelithiasis |
| 8 | McDermott | 1994 | 66 | Male | Cholelithiasis cholangitis |
| 9 | Malatini | 1996 | 25 | Female | Acute cholecystitis |
| 10 | Crosher Rf | 1996 | 63 | Male | Cholelithiasis |
| 11 | Ethomsy G | 1996 | 58 | Female | Acute cholecystitis |
| 12 | D’Agata A | 1997 | 72 | Female | Cholelithiasis |
| 13 | Habib | 1998 | 45 | Female | Cholelithiasis |
| 14 | Demetriadis H | 1999 | 61 | Female | Acute cholelithiaisis |
| 15 | Demetriadis H | 1999 | 37 | Male | Cholelithiasis |
| 16 | Djohan RS | 2000 | 20 | Female | Cholelithiasis |
| 17 | Wong J | 2001 | 68 | Female | Cholelithiasis choledocholithiasis |
| 18 | Al-Jumaily | 2001 | 46 | Female | Microlithiasis gallbladder |
| 19 | Nursal TZ | 2001 | 42 | Female | Cholelithiasis |
| 20 | Donthi R | 2001 | 43 | Female | Chronic cholecystitis |
| 21 | Donthi R | 2001 | 34 | Female | |
| 22 | Yaghan RJ | 2001 | 48 | Female | Cholelithiasis |
| 23 | Yaghan RJ | 2001 | 38 | Female | Cholelithiasis |
| 24 | Franklin ME | 2001 | 25 | Female | Cholelithiasis |
| 25 | Polychronidis M | 2002 | 68 | Male | Cholelithiasis |
| 26 | Tronge A | 2002 | 28 | Female | Cholelithiasis |
| 27 | Pitiakoudis M | 2005 | 47 | Female | Cholelithiasis |
| 28 | Das S | 2005 | 40 | Female | Cholelithiasis |
| 29 | Damian Mc Kay | 2005 | 32 | Female | Cholelithiasis |
| 30 | Kamitani S | 2005 | 76 | Male | Cholelithiasis |
| 31 | Kumar S | 2007 | 57 | Female | Cholelithiasis |
| 32 | Rosen H | 2008 | 36 | Male | Acute cholecystitis |
| 33 | Hamdi J | 2009 | 41 | Male | Acute cholecystitis |
| 34 | Eisenberg D | 2009 | 61 | Male | Cholelithiasis |
| 35 | Jindal V | 2010 | 55 | Female | Cholelithiasis pancreatitis |
| 36 | Bargaonkar V | 2010 | 47 | Female | Cholelithiasis |
| 37 | Present Study | 2014 | 55 | Male | Cholelithiasis |
Discussion
According to the article published by Vijay Bangaokar there were 36 reported cases of gallbladder pathology managed laparoscopically without any complications [3] [Table/Fig-9] Most of the cases included in the report were situs inversus totalis and few with partial situs inversus with gallbladder on the left side [3]. In the study most cases were females and within age group 20 and 80 years. The indications for surgery was varied from simple cholelithiasis to empyema gallbladder[3]. Our case is 37th one with situs inversus totalis and managed laparoscopically without any complications. In our case the surgery was performed from right side and from the caudal approach.
The condition may present diagnostic difficulty [2]. Pain of biliary colic may be located in the epigastrium or in the left subcostal region and that of cholecystitis radiates to the left infrascapular region and the left shoulder. It has been noted in 30% of previous reported cases of acute cholecystitis in patients with situs inversus that the pain was felt in the epigastrium alone and in 10% the pain was localised to the right upper quadrant. The proposed explanation for this is that the central nervous system may not share in the general transposition. High degree suspicion is required in such cases [5] .
The mirror image anatomy poses difficulty in orientation during laparoscopic cholecystectomy [1,6]. Various laparoscopy ports need to be positioned at sites that are mirror image of those in the usual patient [2].
Second, the surgeon needs to reorient visual images and surgical steps. In the reports described previously the surgeon dissected with his left hand or asked for assistance to grasp the neck of the gallbladder. Retraction on Hartmann’s pouch may be carried out by the assistant, thus allowing the surgeon to operate in a more ergodynamic fashion [1,3].
There is no evidence of bile duct injuries during laparoscopic cholecystectomy in situs inversus totalis [2,3].
Recommendations and future scope
There are several important aspects of the management of gallstones in patients with situs inversus that are worth highlighting.
Situs inversus totalis does not appear to be a contraindication [1,4] to laparoscopic cholecystectomy even in case of empyema [3].
The mirror image anatomy poses difficulty in diagnosis and orientation during laparoscopic cholecystectomy [1,6].
Though laparoscopic cholecystectomy in such patients is technically more demanding, an experienced laparoscopic surgeon can perform it safely [7].
Evaluation of vascular anatomical abnormalities may be done which requires CT Angiogram [2].
Due to requirement of meticulous dissection the time required for surgery is more [2].
Even a left handed surgeon may also find it difficult to perform this surgery as he is used to a right sided gall bladder.
In future Robotics may prevent this difficulty to some extent.
Conclusion
In situs inversus laparoscopic cholecystectomy can be performed safely in gallbladder pathologies even in empyema. But the associated anatomical variations of other structures also should be ruled out preoperatively to prevent untoward consequences. The surgeon should be prepared for the reverse orientation during surgery.
[1]. D McKay, G Blake, Laparoscopic cholecystectomy in situs inversus totalis: a case reportBMC Surg 2005 5(5) [Google Scholar]
[2]. Kumar Senthil, Fusai Giuseppe, Laparoscopic Cholecystectomy in Situs Inversus Totalis with Left-Sided GallbladderAnn R Coll Surg Engl 2007 89(2):186 [Google Scholar]
[3]. Borgaonkar Vijay D, Deshpande Sushil S, Kulkarni Vidyadhar V, Laparoscopic cholecystectomy and appendicectomy in situs inversus totalis: A case report and review of literature. JMinim Access Surg 2011 7(4):242-45. [Google Scholar]
[4]. HT Takei, JG Maxwell, TV Clancy, EA Tinsley, Laparoscopic cholecystectomy in situs inversus totalis.J Laparoendosc Surg 1992 2:171--76. [Google Scholar]
[5]. GM Naikoo, I Wani, I Mir, F Jan, S Mushtaq, MN Ahmad, Emergency Cholecystectomy in Situs Inversus Totalis: Report of a Case.Internet Journal of Medical Update 2008 3(1):50-52. [Google Scholar]
[6]. AY Shah, BC Patel, BA Panchal, Laparoscopic cholecystectomy in-patient with situs inversusJ Min Access Surg 2006 2:27-8. [Google Scholar]
[7]. Eisenberg Dan, Cholecystectomy in situs inversus totalis: a laparoscopic approach.International Medical Case Reports Journal 2009 2009:27-29. [Google Scholar]