Laryngeal Squamous Cell Carcinoma (SCC) in a 12-Year-old Boy with Cutaneous Metastasis:An Unusual Presentation
Sinha Reena1, Singh Reecha2, Kumar Kaushal3, Verma Pranav Kumar4, Singh J.K5
1Tutor, Department of Pathology, Patna Medical College & Hospital, Patna, India.
2Assistant Professor, Department of Pathology, Patna Medical College & Hospital, Patna, India.
3Senior DMO, Department of Medicine, Danapur Railway Hospital, Patna, India.
4Consultant Pathologist, Department of Pathology, MahavirCancer Sansthan, Patna, India.
5Consultant Radiation Oncologist & Director, Department of Radiation oncology, Mahavir Cancer Sansthan, Patna, India.
NAME, ADDRESS, E-MAIL ID OF THE CORRESPONDING AUTHOR: Dr. Reena Sinha, Tutor, Department of Pathology, Patna Medical College & Hospital, Patna, Bihar,India.
Phone: 9771450027,
E-mail: reenarozy@gmail.com
Laryngeal squamous cell carcinoma (SCC) in adolescents is a rare clinical entity and behaves aggressively. The mechanism of laryngeal oncogenesis is complex. Further studies need to be done to know the role that human papilloma virus plays in laryngeal SCC in adolescents.We report a rare case of laryngeal SCC in a 12-year-old boy presenting with cutaneous forehead metastasis.
Cutaneous, Laryngeal, Metastasis, Squamous cell carcinoma
Case Report
A 12-year-old boy attended the ENT Out Patient Department(OPD) at Mahavir Cancer Sansthan with chief complaint of prolonged persistent hoarseness, which was unassociated with dysphagia or odynophagia. A painless swelling measuring 6 x 7 cm, firm in consistency was seen on the forehead [Table/Fig-1]. The swelling was noticed three months back, was mobile, with normal overlying skin and was not fixed to underlying structures. The patient appeared malnourished and cachectic with anaemia. Systemic examination did not reveal any noticeable abnormalities. There was no palpable neck node. He reported no previous history of laryngeal papillomatosis, laryngeal surgery, trauma, intubation, radiation, alcohol or tobacco use, major medical illness, or sexual activity. There was no history of laryngeal cancer or papillomatosis in his siblings or cervical lesions in his mother. Fine needle aspiration (FNA) done from the swelling revealed moderately differentiated squamous cell carcinoma. Thereafter, a complete work up was done to confirm the primary which was in the larynx. The Indirect laryngoscopic examination revealed a globular exophytic growth involving the epiglottis, left aryepiglottic fold and anterior part of the right aryepiglottic fold. Left vocal cord could not be seen but movement of the left hemilarynx was found restricted with compromised airway. Tissue was taken from the growth for histopathological examination and that revealed well differentiated squamous cell carcinoma (SCC) [Table/Fig-2,3]. The patient was planned for chemotherapy and radiotherapy. He received external beam radiation therapy (66-70Gy). Concomitant chemotherapy was started. Local radiation therapy was given to forehead (30Gy). Palliative radiation therapy was given with minimal response. The patient was planned for chemotherapy with paclitaxel but could not afford. Therefore cisplatin was started, 4 cycles given but the patient developed loose motions and swelling of legs. The patient was discharged on request and lost to follow-up.
Metastatic swelling of forehead.

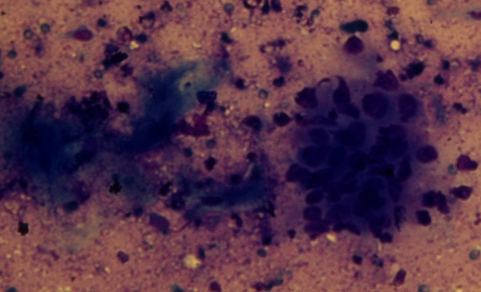
Photomicrograph showing cluster of malignant cells (MGG stain, original ×400).
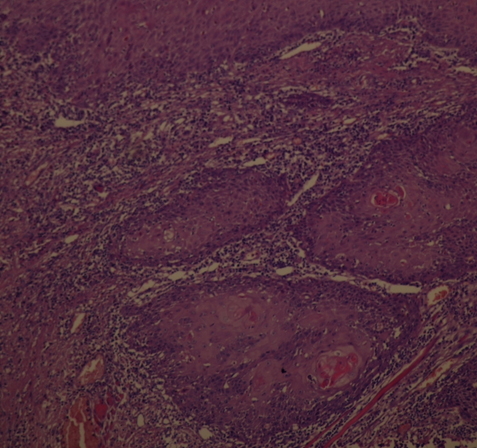
Histopathological section displays feature of squamous cell carcinoma in biopsy (Hematoxylin and eosin stain, original ×100)
Discussion
SCC of the larynx is more common in adults than adolescents and is essentially a lifestyle-related cancer occurring after decades of tobacco use. The first documented case of laryngeal cancer in a child was reported by Rehn in 1868 in a three year-old child [1] . For more than a century thereafter, only 54 cases of laryngeal carcinoma have been reported in children 15-years of age or younger [2] . Clinical manifestations of laryngeal carcinoma in adolescents may include hoarseness or cough, which may be mistaken for common respiratory infections, prepubertal voice change, or other benign childhood conditions [3] .The major risk factor for SCC in adolescents is prior radiation for juvenile papillomatosis, in contrast to adults, in whom smoking is the predominant etiological factor [3] . On biopsy, laryngeal squamous cell carcinoma in adolescents closely parallels the squamous histology seen in adult patients, although its behaviour has been thought to be more aggressive than that found in adults [4] . The management of laryngeal malignancy in children is more difficult than in adults because the tumours tend to behave more aggressively as in our case, likely due to their delayed diagnosis [5] . Cutaneous metastases from laryngeal carcinoma may present as non-tender firm nodules as in our case, as sclerodermoid lesions or may mimic an inflammatory process [6] . N Kumar et al.,[7] reported a rare case of laryngeal carcinoma presenting with metastases to all five distal phalanges of left hand with simultaneous metastasis to multiple sites after two years of receiving radical chemo-radiation to the head and neck region with complete local control. The exact mechanism of skin metastases in squamous cell carcinoma of head and neck is incompletely understood. Several hypotheses have been postulated. The skin metastases may evolve through three possible mechanisms, direct spread, local spread, and distant spread [8] . Direct extension is due to contiguous spread via tissue planes. Local spread can be ascribed to spread through dermal lymphatics with resultant implantation in the skin. Distant metastases are the result of hematogenous spread. This route of hematogenous spread could be either through pulmonary circulation or bypassing pulmonary circulation via azygous and vertebral venous plexus [9] .
Treatment protocols have not been well-established due to the scarcity of cases, but it is typically based upon the stage of the tumour, laryngeal cartilage involvement, and metastases [5] . The prognosis of laryngeal carcinoma in adolescents is unclear because survival rates have not been reported according to tumour stage due to the scarcity of cases [10] . Recently, studies have suggested that prognosis may be affected by the presence of chromosomal translocation (15;19) or the presence of HPV DNA within the tumor cells. Translocation (15;19) results in a BRD4-NUTfusion oncogene, which likely disrupts the normal BRD4 function of regulation of cell cycle progression [11] .
Conclusion
This brief report highlights the importance of clinical awareness of metastatic dissemination to unusual sites in view of increasing cancer survival. Although unusual, carcinoma of the larynx in children is probably more common than thought and the diagnosis should be considered in any case of a child with persistent hoarseness or cough.
[1]. MJ Cunningham, WF McGuirt, EN Myers, Malignant tumors of the head and neck. In: CD. Bluestone, SE. Stool and MA.Kenna, Editors, Pediatric otolaryngology 1996 3rd EditionPhiladelphiaSaunders:1557 [Google Scholar]
[2]. TD Gindhart, WH Johnston, SE Chism, Carcinoma of the larynx in childhood.Cancer 1980 46:1683-7. [Google Scholar]
[3]. A McDermott, P Raj, J Glaholm, De novo laryngeal carcinoma in childhood.J Laryngol Otol 2000 114(4):293-5. [Google Scholar]
[4]. GH Zalzal, RT Cotton, K Bove, Carcinoma of the larynx in a childInt J PediatrOtorhinolar 1987 13(2):219-25. [Google Scholar]
[5]. KC Prasad, P Abraham, R Peter, Malignancy of the larynx in a childEar Nose Throat J. 2001 80(8):508-11. [Google Scholar]
[6]. MH Brownstein, EB Helwig, Pattern of cutaneous metastasesArch Dermatol 1972 105:862-8. [Google Scholar]
[7]. K Narendra, B Anjan, K Ritesh, Squamous cell carcinoma of supraglottic larynx with metastasis to all five distal phalanges of left handIndian J Dermatol 2011 56(5):578-80. [Google Scholar]
[8]. ST Kmucha, JM Troxel, Dermal metastases in epidermoid carcinoma of the head and neckArch Otolaryngol Head Neck Surg 1993 119:326-30. [Google Scholar]
[9]. OV Batson, The role of the vertebral veins in metastatic processesAnn Intern Med. 1942 16:38-45. [Google Scholar]
[10]. N Laurian, R Sadov, M Strauss, Laryngeal carcinoma in childhood. Report of a case and review of the literatureLaryngoscope. 1984 94(5):684-7. [Google Scholar]
[11]. C French, I Miyoshi, I Kubonishi, BRDR4-NUT fusion oncogene: a novel mechanism in aggressive carcinoma.Cancer Res. 2003 63(2):304-7. [Google Scholar]