Submucous Uterine Fibroid Mimicking Ruptured Ectopic Gestation: A Case Report
Rosemary N OGU1, Cosmose Enyindah2, Ngozic Orazulike3, Anthony OU Okpani4
1Senior Lecturer, Department of Obstetrics and Gynaecology, University of Port Harcourt, Port Harcourt, Rivers State, Nigeria.
2Senior Lecturer, Department of Obstetrics and Gynaecology, University of Port Harcourt, Port Harcourt, Rivers State, Nigeria.
3Senior Lecturer, Department of Obstetrics and Gynaecology, University of Port Harcourt, Port Harcourt, Rivers State, Nigeria.
4Professor, Department of Obstetrics and Gynaecology, University of Port Harcourt, Port Harcourt, Rivers State, Nigeria.
NAME, ADDRESS, E-MAIL ID OF THE CORRESPONDING AUTHOR: Dr. Rosemary N Ogu, Senior Lecturer, Department of Obstetrics and Gynaecology, University of Port Harcourt, Port Harcourt, Rivers State, Nigeria.
Phone: +234 803 3129937,
E-mail: dr.ogurosemary@yahoo.com
Ectopic pregnancy is the greatest mimic in gynaecology. Ruptured ectopic gestation usually presents with syncope and severe anaemia. We report the clinical dilemma exposed by the management of a 22-year-old student who presented with syncope and severe anaemia due to a small solitary submucous uterine fibroid.
Menorrhagia, Ruptured ectopic pregnancy, Severe anaemia, Submucous fibroid
Case Report
A 22-year-old P0+0 student presented at the emergency unit with complaints of syncope and extreme fatigue of one and five days duration respectively. She had been well until the week of her presentation when she started feeling extremely fatigued. Her last menstrual period was three weeks prior to presentation; it had lasted the usual eight days and she had used three to four pads daily as is usual for her. There was no associated passage of blood clots. On examination, she was markedly pale; her pulse was barely perceptible at a rate of 132 beats per minute while her blood pressure was markedly hypotensive at 80/40mmhg. Her chest was clinically clear. Her abdomen was soft with mild tenderness and no organs/masses were palpable. Vaginal examination revealed normal vulva and vagina; the pouch of Douglas and adnexa were unremarkable while the uterus was normal sized. Her packed cell volume was 14%. Urine beta human chorionic gonadotropin assay was negative. Preliminary ultrasound scan (USS) was suggestive of an adnexal mass. The impression made was severe anaemia secondary to slow leaking ectopic pregnancy. She was transfused with the available two units of blood and scheduled for exploratory laparotomy. The patient insisted she had no likelihood of pregnancy complications and left the hospital against medical advice. She was re-presented one week later with worsening symptoms of anaemic heart failure, but normal abdominal findings. Repeat USS was suggestive of a submucous fibroid. She was resuscitated, transfused with four units of blood and scheduled for abdominal myomectomy. Intra-operatively [Table/Fig-1], a solitary submucous nodule 5cm by 3cm was enucleated[Table/Fig-2]; and was confirmed a fibroid on histologic evaluation. She was discharged home on the fifth postoperative day in satisfactory clinical state. Three months after the surgery, she is in good clinical condition, with monthly menses lasting for four days.
Submucous fibroid in utero
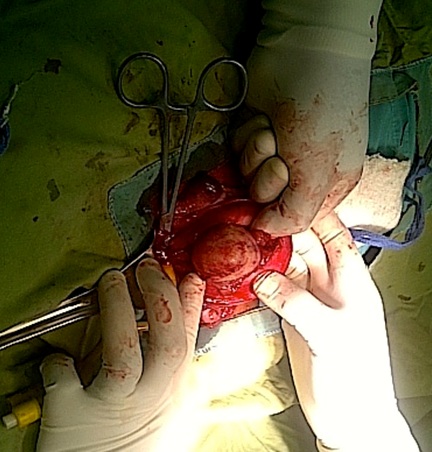
Shelled out submucous fibroid

Discussion
Ectopic pregnancy is the greatest mimic in gynaecology [1,2] and that when ruptured usually presents with syncope and severe anaemia [3]. It is particularly interesting when ubiquitous [4-6] uterine fibroid presents like ruptured ectopic gestation. Although, uterine fibroids may present with severe anaemia from menorrhagia, this is not common in 22-year-old with normal sized uterus. This case has however showed that an apparently normal sized uterus can harbour a submucous fibroid capable of inducing chronic blood loss leading to severe anaemia and anaemic heart failure.
Gynaecologists and specialists in reproductive endocrinology and infertility [7] commonly encounters submucous fibroids (leiomyomas or myomas), with patients presenting with one or a combination of symptoms that include heavy menstrual bleeding, infertility, and recurrent pregnancy loss. There exists a variety of interventions [7] that include those performed under hysteroscopic, laparoscopic and laparotomic direction; an evolving spectrum of image guided procedures, and an expanding number of pharmaceutical agents, each of which has value for the appropriately selected and counseled patient. This patient would have done very well with hysteroscopy. However, she had abdominal myomectomy via laparotomy, as this is the available therapeutic option in our centre.
Could another method of treatment have been offered to her? In settings where it is available, radio frequency volumetric thermal ablation (RFVTA) is a safe and effective treatment for menorrhagia in women with symptomatic fibroids, providing both clinically and statistically significant reduction in blood loss [8]. Hysteroscopic resection could also have been done for this single small submucous fibroid, thus negating the need for a laparotomy and scarred uterus with its consequences on future reproductive career.
If she had been sexually promiscuous, she may have had a laparotomy for suspected slow leaking ectopic gestation. Who knows the number of negative laparotomies in young females that are as a result of missed diagnoses from symptomatic submucous fibroids. It can never be overemphasized that an unprejudiced mind and excellent clinical examination of patients is necessary to overcome diagnostic dilemmas.
Conclusion
Submucous uterine fibroids may present with features suggestive of ruptured ectopic gestation. Thus, the role of history taking and thorough examination is very essential in the management of patients.
[1]. GO Igberase, PN Ebeigbe, OF Igbekoyi, BI B I Ajufoh, Ectopic pregnancy: an 11- year review in a tertiary centre in the Niger DeltaTrop Doct 2005 35:175-77. [Google Scholar]
[2]. BL Faleyimu, GO Igberase, MO Momoh, Ipsilateral ectopic pregnancy occurring in the stump of a previous ectopic site: a case reportCases J. 2008 :1-343. [Google Scholar]
[3]. JA Obuna, OU Umeora, BN Ejikeme, VE Egwuatu, Uterine fibroids in a tertiary health centre South East NigeriaNiger J Med 2008 17(4):447-51. [Google Scholar]
[4]. JI Ikechebelu, CO Ezeama, NJ Obiechina, The use of torniquet to reduce blood loss at myomectomy.Niger J Clin Pract 2010 13(2):154-58. [Google Scholar]
[5]. HE Onah, Preoperative pharmacological correction of severe anaemia due to uterine fibroid.Trop J Obstet Gynecol 2006 23(1):44-47. [Google Scholar]
[6]. L Vorvick, S Storck, D Zieve, Ectopic preg. 2012 http://www.ncbi.nlm.nih.gov/pubmedhealth/PMH0001897/ (Accessed 1st Feb 2013). [Google Scholar]
[7]. AAGL Practice Report. Practice Guidelines for the Diagnosis and Management of Submucous LeiomyomasJ Minim Invasive Gynecol 2012 19(2):152-71. [Google Scholar]
[8]. B Ellis, AAGL 2012: RFVTA Effectively Treats Menorrhagia in Women with Symptomatic Fibroids. Conference Report: 2012 American Association of Gynecologic Laparoscopists http://hcp.obgyn.net/conference- insider/aagl2012/content/article/1760982/2112886 Accessed on 14 Aug 2013. [Google Scholar]