Erupted Odontoma: A Case Report
Nilesh Raval1, Dhaval Mehta2, Kanan Vachhrajani3, Abhishek Nimavat4
1Professor & HOD, Department of Oral Medicine & Radiology, Karnavati School of Dentistry, Gugrat, India.
2Reader, Department of Oral Medicine & Radiology, Karnavati School of Dentistry, Gugrat, India.
3Post Graduate student, Department of Oral Medicine & Radiology, Karnavati School of Dentistry, Gugrat, India.
4Post Graduate student, Department of Oral Medicine & Radiology, Karnavati School of Dentistry, Gugrat, India.
NAME, ADDRESS, E-MAIL ID OF THE CORRESPONDING AUTHOR: Dr. Dhaval N Mehta, Reader, Department of Oral Medicine and Radiology, Karnavati School of Dentistry, 907/A Uvarsad-38242, Gujarat, India.
Phone: +919825528915
E-mail:drdhaval80@gmail.com
Odontomas are nonaggressive, hamartomatous developmental malformations or lesions of odontogenic origin, which consist of enamel, dentin, cementum and pulpal tissue ‘Erupted odontoma’ is a term used to specifically denote odontomas, which are exposed into the oral cavity. These are rare entities with only 25-30 cases being reported so far in the dental literature. Here, we present a rare case of an erupted odontoma in an adolescent patient who came with a complaint of bad aesthetics due to the presence of multiple small teeth like structures in the upper front teeth region.
Developmental anomaly of odontogenic origin, Hamartomas, Impacted permanent teeth, Retained deciduous teeth, Tooth like structures
Case Report
A 22-year-old male patient came with a complaint of the presence of small teeth like structures in upper front teeth region and its undesirable appearance was a concern. He had no complaint of pain or any other previous infection.
Patient had no relevant past medical history. Intraoral examination revealed small whitish oval teeth like structures present in the maxillary anterior region. They were hard, nontender, and grade II mobile. Neither expansion of any cortical plates nor any pus discharge was present. There is a presence of retained deciduous left lateral and canine teeth. Upper left central incisor, lateral incisor and canine were missing [Table/Fig-1].
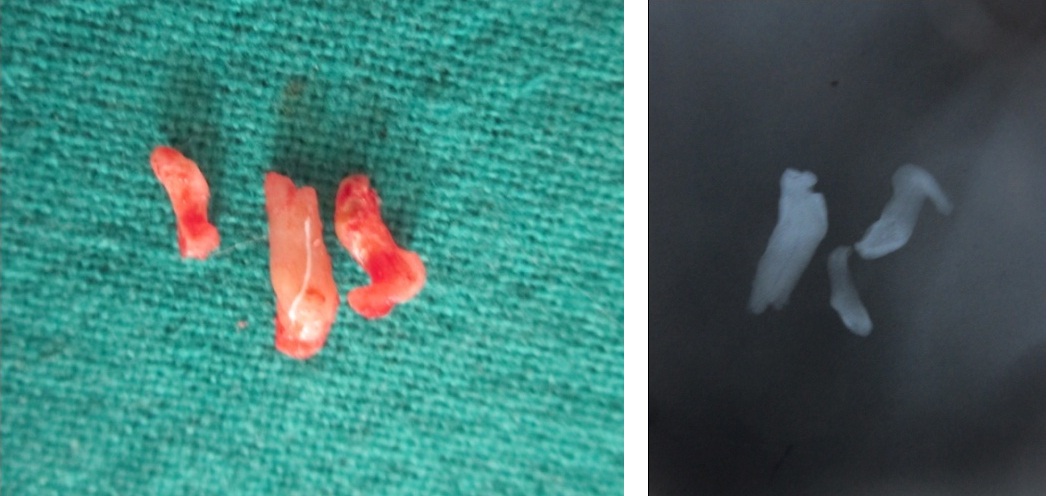
Intraoral periapical radiograph revealed multiple well-defined radiopaque masses similar to density of dental tissues in the alveolar region. It was placed coronal to crown of left impacted maxillary central incisor, lateral incisor and canine suggesting erupted odontoma [Table/Fig-2]. Removal of these teeth like structures and deciduous teeth were done and sent for histopathological report [Table/Fig-3]. Postoperatively there was no complication. After this surgical exposure of impacted teeth along with orthodontic treatment was advised.
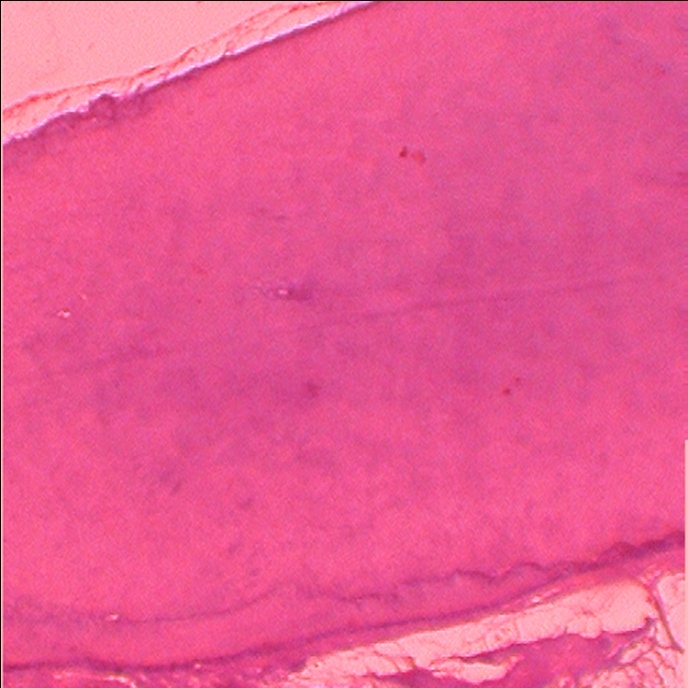
Histopathological examination revealed islands of enamel matrix partially surrounded by enamel epithelium and connective tissue suggestive of odontome [Table/Fig-4].
Small whitish oval teeth like structures present in the maxillary anterior region with retained deciduous teeth

Intraoral periapical radiograph showing multiple well-defined radiopaque masses similar to density of dental tissues in the alveolar region

Extracted odontoma and post operative radiograph of extracted odontome
Histopathological decalcified section showing islands of enamel matrix partially surrounded by enamel epithelium and connective tissue
Discussion
The term odontoma was first used by Paul Broca in 1867. In 1946, Thoma and Goldman formulated a classification for odontomas [1-3].Hitchin stated that odontomas are inherited through a mutant gene, possibly postnatal, with genetic control of tooth development. In human beings, there is a tendency for the lamina between the tooth germs to disintegrate into clumps of cells. The remnants of lamina may be an important factor in the aetiology of complex or compound odontomas and either of these may occur instead of a tooth [4]. Odontomas have been associated with trauma during primary dentition, as well as with inflammatory and infectious processes, hereditary anomalies like Gardner syndrome and Hermann syndrome, and odontoblastic hyperactivity. The mechanism of odontoma eruption appears to be different from tooth eruption because of the lack of periodontal ligament and root in odontoma.
Therefore, the force required to move the odontoma is not linked to the contractility of the fibroblasts, as in the case for teeth. Although, there is no root formation in odontoma, its increasing size may lead to the sequestration of the overlying bone and hence, occlusal movement or eruption. None of the above mentioned aetiology like trauma, infection or hereditary were present in this case.
Usually odontomas are asymptomatic. Clinical signs of odontoma may include retention of deciduous teeth, non eruption of permanent teeth, pain, expansion of cortical bone, and tooth displacement. Pain and swelling are the most common symptoms when odontomas erupt which occur in very few cases. In presented case, the complaint of patient was bad aesthetics due to crowding and multiple erupted teeth like structures- erupted odontome. No complaint of pain or swelling present in this case. As odontomas are associated with impacted permanent teeth and incidentally they diagnosed on radiograph, most of these patients are from very young age group [5]. In presented case patient is also from young age group. In this case also erupted odontome are resoponsible for impaction of maxillary left central incisor, lateral incisor and canine.
Radiographically, the odontoma presents as a well-defined radiopacity situated in bone, but with a density that is greater than bone and equal to or greater than that of a tooth. It contains foci of variable density. A radiolucent halo, typically surrounded by a thin sclerotic line, surrounds the radiopacity. The radiolucent zone is the connective tissue capsule of a normal tooth follicle. The thin sclerotic line resembles the corticated border seen in a normal tooth cryptIn presented case, multiple radio-opaque tooth like structures similar to density of dental tissues were [6,7] present coronal to crowns of left impacted maxillary central incisor, lateral incisor and canine.
Removal of the lesion and enveloping soft tissue with curettage to prevent cystic degeneration is treatment of choice. In case of impacted tooth with compound odontoma, surgical removal of odontome with orthodontic eruption of impacted tooth is indicated. Removal of erupted odontome with surgical exposure of impacted teeth along with orthodontic treatment was advised in present case [8,9].
Conclusion
Due to the rare occurrence of erupted odontoma, this case has been reported. Odontomas rarely erupt into the mouth and are most of the times associated with impacted teeth. Odontomas are benign in nature, but there eruption into the oral cavity can give rise to pain, inflammation and infection and other various clinical appearances. Since odontomas represent a large proportion of jaw tumours, adequate knowledge of their characteristics is necessary for establishment of proper and early diagnosis, followed by a proper treatment at the right time, which will further result in a favourable prognosis.
[1]. D Mehta, N Raval, S Udhani, V Parekh, C Modi, An unusual case report of erupted odontoma.Case Rep Dent 2013 2013:570954 [Google Scholar]
[2]. KV Arunkumar, Vijaykumar N Garg, Surgical management of an erupted complex odontoma occupying maxillary sinusAnn Maxillofac Surg 2012 2(1):86-9. [Google Scholar]
[3]. S Singh, M Singh, I Singh, D Kandelwal, Compound composite odontome associated with an unerupted deciduous incisors a rarityJ Indian Soc Pedod Prev Dent. 2005 23(3):146-50. [Google Scholar]
[4]. Shekar SE, RO Roopa S, Gunasheela B, Supriya N, Erupted compound odontomeJ Oral Maxillofac Pathol 2009 13(1):47-50. [Google Scholar]
[5]. M Vengal, H Arora, S Ghosh, KM Pai, Large erupting complex odontoma: a case report. J Can Dent Assoc 2007 73(2):169-73. [Google Scholar]
[6]. L Junquera, JC de Vicente, P Roig, S Olay, O Rodríguez-Recio, Intraosseus odontoma erupted into the oral cavity: an unusual PathologyMed Oral Patol Oral Cir Bucal 2005 10(3):248-51. [Google Scholar]
[7]. A Tejasvi M L, B Babu B, Erupted compound odontomas: a case report.J Dent Res Dent Clin Dent Prospects. 2011 5(1):33-6. [Google Scholar]
[8]. Y Ohtawa, S Ichinohe, E Kimura, S Hashimoto, Erupted complex odontoma delayed eruption of permanent molarBull Tokyo Dent Coll 2013 54(4):251-57. [Google Scholar]
[9]. MY Padmanabhan, RK Pandey, R Aparna, Erupted composite odontoma associated with malformed teeth - unusual dental aberrations following maxillofacial traumaRom J Morphol Embryol 2013 54(4):1153-56. [Google Scholar]