Study of Aortic- Common Iliac Bifurcation and Its Clinical Significance
Arvind Deswal1, Binod Kumar Tamang2, Anju Bala3
1Tutor, Department of Anatomy, Shri Guru Gobind Tricentuary Medical College, Gurgaon, Haryana, India.
2Associate Professor, Department of Anatomy, Sikkim Manipal Institute of Medical Sciences and Research, Tadong, Gangtok, Sikkim, India.
3Tutor, Department of Anatomy, Sikkim Manipal Institute of Medical Sciences and Research, Tadong, Gangtok, Sikkim, India.
NAME, ADDRESS, E-MAIL ID OF THE CORRESPONDING AUTHOR: Dr. Anju Bala, Tutor, Department of Anatomy, Sikkim Manipal Institute of Medical Sciences and Research, Tadong, Gangtok, Sikkim, India.
Phone: 9232094650, 9416495889,
E-mail: anju.bala1224@gmail.com
Objective: To determine the position of the aortic bifurcation, angle of aortic-common iliac bifurcation in relation to the lumbar vertebra, diameter of distal aorta, length of common iliac, diameter of iliac at bifurcation in cadavers.
Materials and Methods: The present study was done on 25 cadavers (16 males, 9 females) used for the dissection by 1st year MBBS students. The dissections were performed by anterior approach to the lumbar vertebra. The position of the aortic bifurcation, aortic bifurcation angle were measured in relation to lumbar vertebra. The remaining parameters were measured with the help of digital vernier caliper.
Results: The aortic bifurcation was seen in between L3 and L5 vertebra in all the cases. In majority of cases, 16 (64%), the bifurcation was observed at the level of L4 vertebra. During statistical analysis, significant differences were observed in the mean values of aortic-iliac take off angles and in mean diameter of distal aorta.
Conclusion: The exact location of aortic bifurcation is useful when invasive procedures are performed in the pelvis, laproscopic lumbar discectomy and lumbosacral total disc arthroplasty.
The aortic bifurcation mostly found at the level of L4 vertebra in the present study similar to previous studies. The aortic bifurcation can be a reliable landmark for determining the lumbar vertebral segments on MRI or CT.
Aortic bifurcation, Intervertebral disc, Lumbar vertebra, Lumbosacral spine, Parameter
Introduction
The abdominal aorta is the largest artery in the abdominal cavity. As part of the aorta, it is a direct continuation of the descending aorta (of the thorax). The abdominal aorta begins at the median aortic hiatus of the diaphragm, anterior to the inferior border of 12th thoracic vertebra (T12) and the thoraco-lumbar intervertebral disc. It descends anterior to lumbar vertebra to end at the lower border of the 4th lumbar vertebra (L4), a little to the left of midline, by dividing into two common iliac arteries. Common iliac arteries (right to left) diverge as they descend and divide at the level of sacro-iliac joint into external and internal iliac arteries [1] . The anatomical description of aortic -common iliac region is well known. The geometry of the arteries at or near arterial bifurcation influences the blood flow field, which is an important factor affecting artherogenesis. Thus, an individual’s unique arterial geometry might influence that person’s risk of arterial diseases. The anatomy of the aorta and its relationship to the vertebra would provide useful information to the surgeon for the anterior lumbosacral approach [2] . Since there is scarcity of the data on geometric measurements of aorta-common iliac bifurcation in north-east region of India. The present study may be of helpful for the future references. The aim of the present study was to determine the position of aortic bifurcation, diameter of distal aorta in relation to the lumbar vertebra, length of common iliac arteries, diameter of iliac at bifurcation, aortic bifurcation angle.
Material and Methods
The present study was done on 25 cadavers, 16 males and 9 females in the Department of Anatomy, Sikkim Manipal Institute of Medical Sciences. Digital caliper, scale in centimeters, two transparent protractors and a reference board at least of 30 cm long to obtain the measurements were used in this study. The measurements were done on cadavers without mobilization of the aortic-common iliac segments so that geometric orientation was not altered from its in vivo state in anyway. The measured Sectiondata were subjected to statistical analyses by calculation of mean, standard deviation and using unpaired t-test. The results were considered significant at a value of p<0.05.
Results
The aortic bifurcation in all the cases was seen in between L3 and L5, most often at the L4 vertebra (16 cases, 64%) [Table/Fig-1] . Remaining was seen at the level of L4-L5 intervertebral disc in 4 cases (16%), at the level of L5 vertebra in 3 cases (12%), at the level of L3 vertebra in 1 case (4%) and at the level of L3-L4 intervertebral disc in 1 case (4%) [Table/Fig-2,3] . The value of mean aortic bifurcation angle was 50.16 ± 8.64°, with a value of 49.37 ± 10.34° in male and 51.55 ± 4.50° in female. No significant difference was observed in the mean aortic angle between male and female (p>0.05).
The mean values of aortic-iliac take off angles on the right (αR) and left (αL) side were 27.24 ± 7.65° and 22.92 ± 7.01° respectively. Significant difference was observed in the mean values of aortic-iliac take off angles between right and left sides (p< 0.05). In females, the average values of aortic-iliac take off angle right (αR) and left (αL) were 23 ± 7.72° and 28.55 ± 7.38° respectively and in males 29.62 ± 6.70° and 19.75 ± 4.44° respectively. On comparison between right and left side, statistically significant values were observed in males, but not in females [Table/Fig-4].
The mean values of length of common iliac on the right and left side were 56.49 ± 17.82 mm and 53.75 ± 18.25 mm respectively. No statistically significant difference was observed in mean values of length of common iliac. In females, the average values of length of common iliac on the right and left side were 48.65 ± 13.23 mm and 46.63 ± 12.65 mm and in males, 60.90 ± 18.89 mm and 57.76 ± 20.01 mm respectively. On comparison of these measurements between females and males, no significant differences were observed [Table/Fig-4].
The mean values of diameter of common iliac distal to bifurcation on the right and left sides were 9.91 ± 1.86 mm and 9.22 ± 2.44 mm respectively. No significant difference was observed. In females, the average values of diameter of iliac distal to bifurcation on the right and left sides were 9.61 ± 1.25 mm and 9.03 ± 1.29 mm respectively and in males, 10.07 ± 2.15 mm and 9.32 ± 2.94 mm respectively. No significant differences were observed.
The mean diameter of distal aorta was 16.06 ± 2.4mm. In females, the average diameter of distal aorta was 14.59 ± 0.86 mm and in males, 16.88 ± 2.94 mm and statistically significant difference was observed between the two groups [Table/Fig-4].
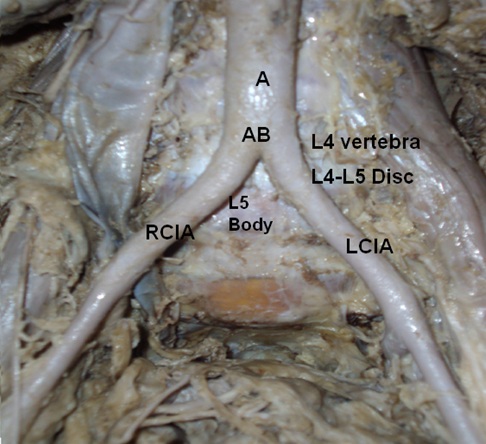
Aortic – common iliac Bifurcation level and position of aortic bifurcation angle in relation to lumbar vertebra (A- aorta, AB- aortic bifurcation level, RCIA- right common iliac artery, LCIA- left common iliac artery)
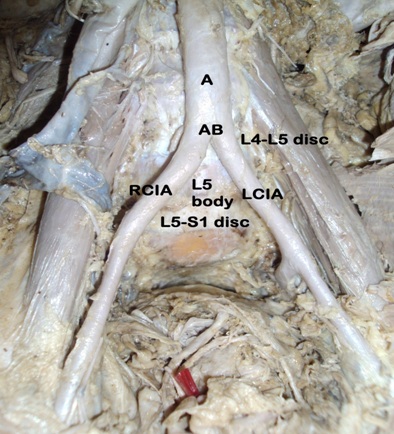
Anterior view of position of aortic bifurcation angle in relation to lumbar vertebra. (A- aorta, AB- aortic bifurcation, RCIA- right common iliac artery, LCIA- left common iliac artery, L4-L5 intervertebral disc, L5-S1 intervertebral disc)
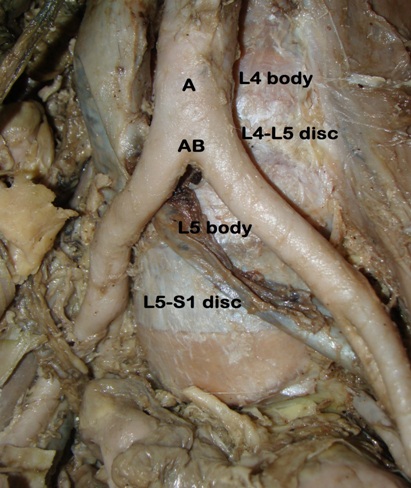
Anterior view of aortic bifurcation level in relation to lumbar vertebra. (A- aorta, AB- aortic bifurcation level)
Comparison of right and left parameters in males and in females
| Parameters | Male Mean ± SD | Female Mean ± SD |
| | R | L | R | L |
| Length of common iliac (mm) | 60.90 ± 18.89 | 57.76 ± 20.01 | 48.65 ± 13.23 | 46.63 ± 12.65 |
| Diameter of iliac at bifurcation (mm) | 10.07 ± 2.15 | 9.32 ± 2.94 | 9.61 ± 1.25 | 9.03 ± 1.29 |
| Take off angle of common iliac α (deg) | 29.62 ± 6.70 | 19.75 ± 4.44 | 23.0 ± 7.72 | 28.55 ± 7.38 |
| Diameter of distal aorta (mm) | 16.88 ± 2.64 | 14.59 ± 0.86 |
Discussion
The increased difficulty and morbidity in a laparoscopic approach at L4-L5 intervertebral disc has been linked to the prevertebral vascular anatomy and specifically at the level of bifurcation of the aorta [3] . When compared with previous literatures, the present study had shown some variations in result. Kawahara et al., studied 21 cadavers and reported the aorta descended and branched into two common iliac arteries at L3 in one cadaver, at L3-L4 in two cadavers, at L4 in eight cadavers, at L4-L5 in nine cadavers and at L5 in one cadaver [4] . Khamanarong K et al., examined the level of aortic bifurcation in Thai cadavers. They found that aortic bifurcation at the level of L4 vertebra in 131 cases (70.1%), at the 4th lumbar intervertebral disc in 23 cases (12.3%) and at the level of L5 vertebra in 33 cases (17.6%) [5] . Lee CH et al., studied 210 patients by MRI and found that aortic bifurcation level was at L4 vertebra (83%) [6] . In present study, the aortic bifurcation level was at L4 vertebra in 16 cases (64%) and at the level of L4-L5 intervertebral disc in 4 cases (16%).
Ganananda Nanayakkara B et al., studied 11 cadavers of which six were male and five were female. In females, the average values of the aortic-iliac take-off angle αR and αL were 7.18° and 14.58° respectively. In males, the average values of the aortic-iliac take-off angle αR and αL were 16.67° and 13.16° respectively [3] . In present study, the average values of aortic-iliac take off angle αR and αL in female were 23 ± 7.72° and 28.55 ± 7.38° and in males, were 29.62 ± 6.70° and 19.75 ± 4.44° respectively.
Lakchayapokorn K et al., found mean aortic bifurcation angle 54° (54 ± 16°) with a value of 55 ± 15° in males and 53 ± 18° in females [7] . While in present study, mean aortic bifurcation angle was 50.16 ± 8.64° with a value 49.37 ± 10.34° in males and 51.55 ± 4.50° in females.
The varying grade of aortic bifurcation angle would lead to the increase risk factor for aortic-iliac occlusive disease [2,3] . The main complications of the anterior transperitoneal approach and anterolateral retroperitoneum approach of lower lumbar vertebra are the vessels injuries mainly at the level of aortic bifurcation [7] . Access to this level requires careful dissection and mobilization of the vessels. The risk for vascular damage during anterior lumbosacral surgery varies from one to another individual depending on their vascular anatomy.
Conclusion
The geometry of the arteries at or near arterial bifurcations influences the blood flow field, which is an important factor affecting artherogenesis. Thus, an individual’s unique arterial geometry might influence that person’s risk of arterial disease. The ability to measure arterial geometry invivo would be helpful for testing this hypothesis and for screening purposes should it be found to be valid. It is also useful because anterior lumbar interbody fusion is gaining in popularity.
Clinical Implication: Knowledge of vascular anatomy of aorta is of great importance during surgical procedures, so it is necessary to know the most common patterns and variations. Therefore, a vertebral surgeon ought to be aware of preoperative planning if possible. He must identify the abnormality before the operation in order to prevent the difficulty of surgery and the complications that may occur. The data may be useful in the fields of medicine, surgery and forensic medicine. This study will be helpful for patients suffering from aortic-iliac atherosclerosis and abdominal aortic aneurysm.
[1]. S Standring, Gray’s anatomy: The anatomical Basis of Clinical Practice 2008 40th EditionEdinburg, London.Elsevier Churchill livingstone:710-11. [Google Scholar]
[2]. PM Shah, HA Scarton, MJ Tsapogas, Geometric anatomy of the aortic common iliac bifurcationJ Anat 1978 126(3):451-58. [Google Scholar]
[3]. B Ganananda Nanayakkara, CK Gunarathne, ADDS Sanjeewa, KAR Gajaweera, AS Dahanayake, UHC Sandaruwan, Geometric anatomy of aorticcommon iliac bifurcation.Galle Medical Journal 2007 12 [Google Scholar]
[4]. N Kawahara, K Tomita, H Baba, Y Toribatake, T Fujita, K Mizuno, Cadaveric vascular anatomy for total en bloc vertebral spondylectomy in malignant tumoursSpine. 1996 21(12):1401-07. [Google Scholar]
[5]. K Khamanarong, S Sae-Jung, C Supra-adirek, S Teerakul, P Prachaney, Aortic Bifurcation: A cadaveric study of its relationship to the spineJ Med Assoc Thai 2009 92(1):47-9. [Google Scholar]
[6]. CH Lee, BK Seo, YC Choi, HJ Shin, JH Park, HJ Jeon, Using MRI to evaluate anatomic significance of aortic bifurcation, right renal artery and conus medullaris when locating lumbar vertebral segments.Americal Journal of Roengenology 2004 182(5):1295-1300. [Google Scholar]
[7]. K Lakchayapakorn, Y Siriprakarn, Anatomical Variations of the position of the Aortic Bifurcation, Iliocava Junction and Iliac veins in relation to lumbar vertebra.J Med Assoc Thai 2008 91(10):1564-70. [Google Scholar]