The modified radical mastectomy (MRM) has become more common surgery in breast cancer cases and breast reconstruction after mastectomy [1]. Therefore, the surgeons are supposed to have thorough knowledge about the anatomy of the medial and lateral pectoral nerves and its possible variations to prevent and to minimise the possible complications due to injury to these nerves (denervation) [2]. Even cosmetic surgeons also deal with these nerves during breast augmentations (breast implants) for the females who desire to have better projection and attractive contour for their breasts [3]. This study also helps the plastic surgeons for the safe and functional transfer of the pectoralis major muscle in myocutaneous free flap surgery [4,5].
Usually, the medial pectoral nerve originates from the medial cord of the brachial plexus and runs along the lower border of the pectoralis minor muscle, supplying it and also supplying the lower half of the pectoralis major muscle by its distal branch. Similarly, the lateral pectoral nerve arises from the lateral cord of the brachial plexus and runs with the pectoral branch of thoracoacromial artery and vein on the under surface of the proximal portion of the pectoralis major muscle, finally innervating the upper half only or the whole of the pectoralis major muscle [6].
To find the possible variations in the origin, course, relations and the accompanying structures for the medial and lateral pectoral nerves.
To find the pattern of pectoral nerves distribution to the pectoralis major and minor muscles.
To find the possible location of piercing of the pectoral nerves in the pectoral muscles from the lateral margin of sternum and its relation with the extent of costal attachment of the pectoralis minor muscle.
The overall objective of this study is to determine the anatomy and its possible variations in the course of the pectoral nerves and their innervation to the pectoralis major and minor muscles for guiding the surgeons by making them to be aware of the possible variations to prevent and to minimise the possible complications due to injury to these nerves during mastectomy (in breast cancer), during breast augmentations, and in myocutaneous free flap transfer in head and neck or anterior chest wall.
Materials and Methods
After the approval of the Local Ethical Committee in Azeezia Medical College, Meeyyannoor, Kollam Dist, Kerala state, India a total of 50 pectoral region specimens (both right and left sided) from 25 embalmed adult human cadavers (20 female and 05 male) with an average age of 45-50 years, given for M.B.B.S – Ist year undergraduate students for dissection during the academic years from 2008–2013 in the Department of Anatomy, Azeezia Medical College.
In the cadavers, pectoral regions were dissected as per the Standard method of dissection. The skin and subcutaneous fat from the entire supraclavicular, infraclavicular and axillary areas had been removed. An axillary dissection was performed to find out the course of the medial pectoral nerve and its relationship with the pectoralis major muscle. Then, the brachial plexus was dissected carefully after removing the clavicle to find out the origin of the pectoral nerves. Finally, an infraclavicular dissection was done to reflect the pectoralis major muscle medially, to study the course and branches of the lateral pectoral nerve. Similarly, the pectoralis minor muscle was freed from the coracoid process to note the branches and course of the medial pectoral nerve.
The origin, location, course, relations and branches of the pectoral nerves were noted and recorded with tabulations and photographed.
Statistical Analysis
Data were collected from 50 embalmed adult human cadaveric specimens (20 female and 05 male) belonging to both right and left sides, and entered in Microsoft excel and analysed by using Statistical Package for Social Science (SPSS 17th version). Mean, Proportion, Standard deviation and Unpaired t-test was applied for analysing the data obtained.
Results
[Table/Fig-1,2,3,4,5,6,7,7a,7b,8,9and10] All these observations were recorded and tabulated as follows. The data collected was computerised and analysed by using Statistical Package for Social Science (SPSS 17th version).
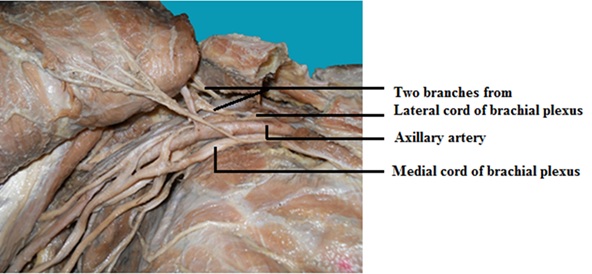
Two branches arising from lateral cord join to form LPN
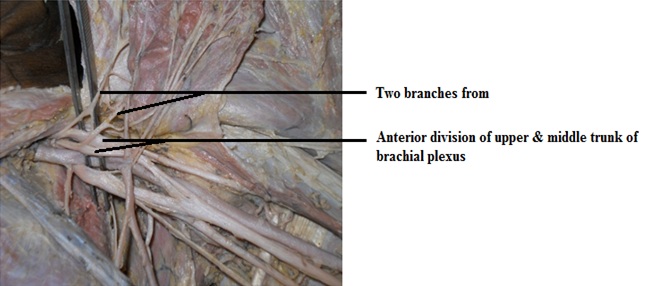
Two branches from anterior division of upper & middle trunk forms LPN
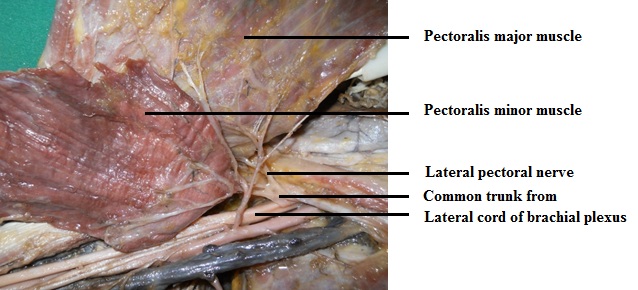
A common trunk from the lateral cord of brachial plexus gives both MPN & LPN
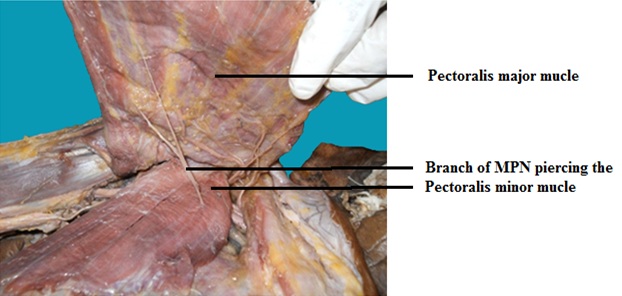
One branch of MPN piercing the pectoralis minor muscle
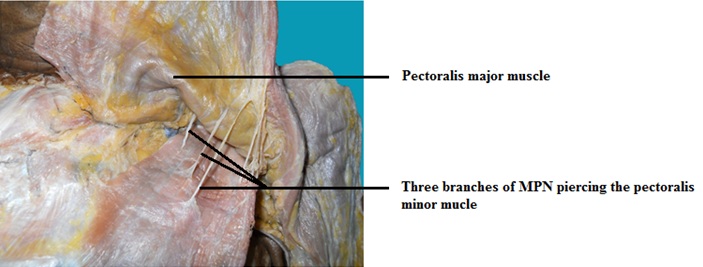
Three branches of MPN piercing the pectoralis minor muscle
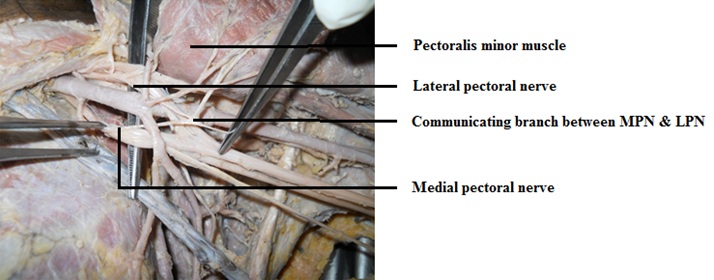
Communicating branch between MPN & LPN supplying the pectoralis minor muscle
Anatomical study of pectoral nerves (origin and size) and its implications in surgery
| Total cadavers | 25 |
|---|
| Sex of the cadavers | 20 Female & 05 Male |
| Total specimens | 50 (25 right & 25 left sided) |
| Approx. Age in years | 45 – 50 Yrs. |
| Features | Medial Pectoral Nerve (MPN) | Lateral Pectoral Nerve (LPN) |
| Origin | In 44 specimens, it arises as a branch from medial cord of brachial plexus | In 31 specimens, it arises as a branch from lateral cord of brachial plexus. In 08 specimens, two branches from lateral cord join to form LPN [Table/Fig-1]. In 05 specimens, two branches from anterior division of upper & middle trunk of brachial plexus forms LPN [Table/Fig-2] |
| In 06 specimens, a common trunk from the medial cord of brachial plexus gives both the medial & lateral pectoral nerves [Table/Fig-3] |
| Size | 42 specimens – small 08 specimens - large | 08 specimens – small 42 specimens – large |
| Extent of costal attachment of the pectoralis minor muscle (in cm) | In 38 specimens, it is less than 6.0cm (5 – 5.7cm) indicating that MPN pierces the pectoralis minor muscle as one branch or trunk and then ramifies in the muscle. In 12 specimens, it is more than 6.6cm (6.8-7.4cm) indicating that MPN divides into branches before piercing into the pectoralis minor muscle. |
Anatomical study of pectoral nerves (course) and its implications in surgery
| Medial Pectoral Nerve (MPN) | Lateral Pectoral Nerve (LPN) |
|---|
| Course | Piercing the pectoralis minor muscle | In all the specimens, branch of MPN pierces the pectoralis minor muscle – as one branch in 38 specimens[Table/Fig-4] as two branches in 06 specimens; as three branches in 04 specimens [Table/Fig-5] & as a branch from communicating branch in 02 specimens. | In 02 specimens, along with branch of MPN, LPN pierces the pectoralis minor muscle & runs under surface of the pectoralis major muscle. In other 48 specimens, LPN does not pierce the pectoralis minor muscle. |
| Running on the medial aspect (upper border) of the pectoralis minor muscle | Nil | In all the specimens, LPN runs along the upper border or medial aspect of the pectoralis minor muscle. |
| Running on the lateral aspect (lower border) of the pectoralis minor muscle | In all the specimens, after giving a branch that pierces the pectoralis minor muscle, then MPN runs along the lower border or the lateral aspect of the pectoralis minor muscle to reach the pectoralis major muscle. | Nil |
| Any other course | Nil | Nil |
| Runs under surface of the pectoralis major muscle | Nil | In all the specimens, LPN runs under surface of the pectoralis major muscle after emerging at the upper border of the pectoralis minor muscle. |
| Distance of nerve from lateral margin of sternum (in cm) | 8.8 – 10.8cm | 5.8 – 10.2cm |
Anatomical study of pectoral nerves (accompanying structures and distribution) and its implications in surgery
| Medial Pectoral Nerve (MPN) | Lateral Pectoral Nerve (LPN) |
|---|
| Accompanying vessels with the nerves | In 45 specimens, accompanied by lateral thoracic vessels. In 04 specimens, by direct branches from the axillary artery. In 01 specimen, by small pectoral branch of thoracoacromial artery. | In all the specimens, accompanied by pectoral branch of thoracoacromialartery. |
| Distribution (Supply) | Pectoralis minor muscle | In all the specimens, it is supplied by MPN | In 02 specimens, LPN supplies the pectoralis minor muscle along with MPN |
| A branch from lateral cord & from communicating branch supplies the pectoralis minor muscle in 01 specimen [Table/Fig-6] |
| Pectoralis major muscle | In all the specimens, MPN supplies lower portion (distal segment) of the pectoralis major muscle. | In all the specimens, LPN supplies upper portion (proximal segment) of the pectoralis major muscle. |
Statistical analysis of 50 samples (both female and male belonging to right and left side)
| Distance of branch of MPN piercing the pectoral muscle from lateral margin of sternum | Distance of branch of LPN piercing the pectoral muscle from lateral margin of sternum |
|---|
| Total samples | 50 | 50 |
| Mean | 10.0560 | 8.6040 |
| Std.Error of Mean | 0.05687 | 0.14303 |
| Std. Deviation | 0.40212 | 1.01136 |
| Variance | 0.162 | 1.023 |
| Minimum | 8.80 | 5.80 |
| Maximum | 10.80 | 10.20 |
Statistical analysis of male and female comparison (applying unpaired t-test)
| Sample | Sex | No | Mean | Std. Deviation | Std. Error of Mean | p-value | | Levene’s Test for Equality of Variances | t-test for Equality of Means |
|---|
| F | Sig. | t | df |
|---|
| Distance of branch of MPN piercing the pectoral muscle from lateral margin of sternum | F | 40 | 10.05 | 0.44 | 0.69 | 0.70 | MPN | Equal variances assumed | 3.71 | 0.06 | -0.38 | 48 |
| M | 10 | 10.10 | 0.22 | 0.68 | Equal variances not assumed | - | - | -0.57 | 29.75 |
| Distance of branch of LPN piercing the pectoral muscle from lateral margin of sternum | F | 40 | 8.68 | 1.05 | 0.17 | 0.29 | LPN | Equal variances assumed | 1.53 | 0.22 | 1.06 | 48 |
| M | 10 | 8.30 | 0.82 | 0.26 | Equal variances not assumed | - | - | 1.24 | 17.26 |
Statistical analysis of right and left side comparison (applying unpaired t-test)
| Sample | Side | No | Mean | Std. Deviation | Std. Error of Mean | p-value | | Levene’s Test for Equality of Variances | t-test for Equality of Means |
|---|
| F | Sig. | t | df |
|---|
| Distance of branch of MPN piercing the pectoral muscle from lateral margin of sternum | R | 25 | 10.02 | 0.39 | 0.08 | 0.58 | MPN | Equal variances assumed | 0.15 | 0.70 | -0.56 | 48 |
| L | 25 | 10.09 | 0.42 | 0.08 | Equal variances not assumed | - | - | -0.56 | 47.70 |
| Distance of branch of LPN piercing the pectoral muscle from lateral margin of sternum | R | 25 | 8.61 | 1.04 | 0.21 | 0.98 | LPN | Equal variances assumed | 0.00 | 0.96 | 0.03 | 48 |
| L | 25 | 8.60 | 1.00 | 0.20 | Equal variances not assumed | - | - | 0.03 | 47.94 |
The mean distance of the branch of the Medial pectoral nerve (MPN) and Lateral pectoral nerve (LPN) from the lateral margin of sternum is 10.06 cm and 8.60 cm, with standard deviation 0.40 and 1.011, with standard error of mean 0.057 and 0.143 respectively. The minimum distance is 8.8cm and 5.8cm; the maximum distance is 10.80cm and 10.20cm respectively for MPN and LPN [Table/Fig-8].
When (50 samples i.e. 40 female and 10 male) subjected to Unpaired t-test [Table/Fig-9] to the sex and to the mean distance of the branch of the medial pectoral nerve and lateral pectoral nerve piercing the pectoral muscle from the lateral margin of sternum, it is found to be not significant with p-value 0.70 for MPN and with p-value 0.29 for LPN (in both p-value is greater than 0.05). This indicates there is no sex variation in the mean distance of branch of MPN and LPN piercing the pectoral muscles from the lateral margin of sternum.
When Unpaired t-test [Table/Fig-10] to the sides (Right and Left) and to the mean distance of the branch of the medial pectoral nerve and lateral pectoral nerve piercing the pectoral muscle from the lateral margin of sternum, it is found to be not significant with p-value 0.58 for MPN and with p-value 0.98 for LPN (in both p-value is greater than 0.05). This means that there is no variation with respect to the sides (Right and Left) in the mean distance of branch of MPN and LPN piercing the pectoral muscles from the lateral margin of sternum.
Discussion
In a cadaveric dissection study [2,7], It was reported that, the lateral pectoral nerve arises most frequently with two branches from the anterior divisions of the upper & middle trunks (33.8%) or as a single root from the lateral cord (23.4%) & the medial pectoral nerve usually arises from the medial cord (49.3%), from anterior division of the lower trunk (43.8%), or from the lower trunk (4.7%). They found that 02 pectoral nerves are usually connected immediately distal to the thoracoacromial artery. The medial pectoral nerve shows communications with the intercostobrachial nerve, and in 50% -100% cases, it passes through the pectoralis minor muscle, and the lateral pectoral nerve supplies the upper part of the pectoralis major muscle and the medial pectoral nerve supplies the lower part of the pectoralis major muscle.
In cadaveric dissection studies [4,5], it has been found that in 62% cases, the medial pectoral nerve courses through the pectoralis minor muscle innervating it and also supplies the lower half or lower 2/3rd of the pectoralis major muscle and in 38% of patients, it exits around the lateral aspect of the pectoralis minor muscle. Similarly, the lateral pectoral nerve found to run on the under surface of the pectoralis major muscle, innervating the proximal 1/3rd or upper half of the muscle. And, also observed that the lateral pectoral nerve being larger in all the specimens than the medial pectoral nerve, indicating its greater importance in an innervation of the pectoral muscles. In a study of 25 cadavers (50 specimens), [8] the lateral pectoral nerve found to course on the medial side of the pectoralis minor muscle in 90% cases, while a majority of the medial pectoral nerves appear only lateral to this muscle.
In our present study, the medial pectoral nerve arises as a branch from the medial cord of brachial plexus in 44 specimens (88%) and the lateral pectoral nerve arises as a branch from the lateral cord of brachial plexus in 31 specimens (62%); as two branches from the lateral cord joining together to form LPN in 08 specimens (16%) [Table/Fig-1] in 05 specimens (10%), two branches from the anterior division of upper and middle trunk of brachial plexus forms LPN [Table/Fig-2]. In another 06 specimens (12%), the medial and the lateral pectoral nerves arises from a common trunk from the lateral cord of the brachial plexus [Table/Fig-3]. From our study, it has been concluded that the medial pectoral nerve pierces the pectoralis minor muscle – as a single branch in 38 specimens (76%) [Table/Fig-4] as two branches in 06 specimens (12%); as three branches in 04 specimens (08%) [Table/Fig-5]; as a branch from communicating branch in 02 specimens (04%) and finally, the medial pectoral nerve runs along the lower border or lateral aspect of the pectoralis minor muscle to reach the pectoralis major muscle. Similarly, the lateral pectoral nerve pierces the pectoralis minor muscle along with the medial pectoral nerve in 02 specimens (04%) whereas in 48 specimens (96%), the lateral pectoral nerve runs along the upper border or on the medial aspect of the pectoralis minor muscle without piercing it and finally runs undersurface of the pectoralis major muscle.
The patients who underwent modified radical mastectomy with preservation of the medial pectoral nerve, presented no significant muscle loss and strength of the pectoralis major, as evaluated after 15 & 45 days of mastectomy, compared with the group of women in whom this nerve was sectioned and the outcome of the Patey modified radical mastectomy with the excision of the pectoralis minor muscle, found the following sequence: fibrosis, atrophy, shortening of the pectoralis major muscle, limitations to the shoulder movements and skeletonisation of the chest wall [9–11].This indicates that just the medial pectoral nerve injury alone will not cause any significant loss in the strength of the pectoralis major muscle. In a dissection study of 30 specimens of pectoral regions from 15 embalmed adult human cadavers [12], it was concluded that the pectoralis major muscle is mainly innervated by the lateral pectoral nerve, supplemented by the medial pectoral nerve branches; and the proximal segment of the muscle is separately supplied by the lateral pectoral nerve, therefore, allowing it to use as a myocutaneous free flap transfer.
In another study of 15 fresh cadavers [3], they found 03 constant branches of pectoral nerves – superior branch supplying clavicular fibres of the pectoralis major muscle; middle branch coursing undersurface of the pectoralis major muscle along with the pectoral branch of thoracoacromial artery, supplies the sternal part of the pectoralis major muscle; the inferior branch passes beneath the pectoralis minor muscle supplying it and also the costal part of the pectoralis major muscle. In a similar study, [13] aiming to find the importance of preserving the pectorals minor muscle in a modified radical mastectomy reported an atrophy rate up to 06% in the pectoralis major muscle compared with an atrophy rate of 54% in woman who had their pectoralis minor muscle removed. The main reason for such impairment in the pectoralis major muscle after a Patey MRM is due to the injury to both the middle and inferior branches of the pectoral nerves. In our present study, inferior branch corresponds to the medial pectoral nerve that supplies the pectoralis minor muscle as whole and a branch of it also supplies the lower portion of pectoralis major muscle; and superior and middle branches correspond to the branches of the lateral pectoral nerve supplying mainly the pectoralis major muscle especially proximal or upper segment.
In our present study, in all the specimens, the pectoralis minor muscle is supplied by the branch of the medial pectoral nerve only, whereas, the pectoralis major muscle – upper portion or proximal 2/3rd is supplied only by the branch of lateral pectoral nerve; lower portion or distal 1/3rd of the muscle is supplied by the branches of both the medial pectoral nerve and the lateral pectoral nerve. In this current study, the medial pectoral nerve is accompanied by lateral thoracic vessels in 45 specimens (90%); by the direct branches from axillary artery in 04 specimens (08%); by a small pectoral branch of thoracoacromial artery in 01 specimen (02%). And the lateral pectoral nerve is accompanied by the pectoral branch of thoracoacromial artery in all the specimens of our study.
In a cadaveric dissection study of 08 embalmed female cadavers [10], it was observed that the lateral pectoral nerve always run on the deep surface of the pectoralis major muscle under its fascia along with the thoracoacromial vessels, and the medial pectoral nerve showed two main patterns of branching correlating with the extent of the costal attachment of the pectoralis minor muscle – when the costal attachment of the muscle is narrower than 6.0cm (56%), then the nerve pierces the pectoralis minor muscle as a single trunk, ramify in the muscle supplying it and give branches to the pectoralis major muscle; if the costal attachment of the muscle is wider than 6.6 cm, then the nerve divides into branches before piercing the pectoralis minor muscle and the medial branch among the two branches direct towards the pectoralis major for innervating it (lower half) [14]. This medial branch of the medial pectoral nerve present 10.3 cm lateral to the margin of sternum.
In this current study, we observed the same findings that the medial pectoral nerve pierces the pectoralis minor muscle as a single trunk or as a single branch and ramify into the muscle supplying it when the length of the costal attachment of the pectoralis minor is narrower than 6.0 cm (5.0 cm – 5.7 cm) in 38 specimens (76%), and if the length of the costal attachment of the pectoralis minor muscle is broader than 6.6 cm (6.8 cm-7.4 cm) in 12 specimens (24%), then the medial pectoral nerve divides into branches before piercing the pectoralis minor muscle supplying it. In this present study, the medial pectoral nerve is observed to be smaller in size compared to the lateral pectoral nerve in 42 specimens (84%), but in 08 specimens (16%), the medial pectoral nerve found to be bit larger compared to the lateral pectoral nerve indicating the dominance of LPN in supplying the pectoral muscles. This study also revealed the distance of the branches of the medial pectoral nerve and the lateral pectoral nerve piercing the pectoral muscles from the lateral margin of the sternum being 8.8 cm-10.8 cm and 5.8 cm-10.2 cm respectively on both sides (right and left).
Conclusion
To guide the surgeons (in mastectomy, breast augmentation and myocutaneous free flap surgery in head and neck) with respect to possible variations in the origin, course, relation and supply of pectoral nerves, a total of 50 pectoral region specimens (both right and left sided) from 25 embalmed adult human cadavers (20 female & 05 male) were studied by Standard dissection method, and concluded that in all the specimens, the medial pectoral nerve pierces the pectoralis minor muscle as a single trunk (76%), and as dividing branches in 34% specimens. The extent of costal attachment of the pectoralis minor muscle found to be less than 6.0cm in cases of the medial pectoral nerve piercing the pectoralis minor muscle as a single trunk. The medial pectoral nerve takes origin from the medial cord of brachial plexus in 44 specimens (88%) and in 06 cases (12%), a common trunk from the lateral cord of brachial plexus gives both the medial and lateral pectoral nerves. The medial pectoral nerve after piercing the pectoralis minor, ramify in the muscle supplying it, finally runs along the lateral aspect (lower border) of the pectoralis minor to supply the lower portion or distal segment of the pectoralis major muscle. Similarly, the lateral pectoral nerve takes origin from the lateral cord of brachial plexus in 31 specimens (62%); in 08 specimens (16%) two branches from the lateral cord join to form the lateral pectoral nerve; in 05 specimens (10%), two branches from the anterior division of upper and middle trunk of brachial plexus forms the lateral pectoral nerve; in 06 specimens (12%), a common trunk from the medial cord of brachial plexus gives both the medial & lateral pectoral nerves, then runs along the upper border (medial aspect) of the pectoralis minor muscle (98%) and then runs under surface of the pectoralis major muscle along with pectoral branch of thoracoacromial artery, supplying the upper portion or most of the proximal 2/3rd of the pectoralis major muscle. In maximum number of specimens (42 i.e. 84%), the lateral pectoral nerve is larger in size compared to the medial pectoral nerve showing its importance in innervation of the pectoral muscles. The distance of the branches of the lateral pectoral nerve and the medial pectoral nerve piercing the pectoral muscles from the lateral margin of sternum is 10.06 cm and 8.6 cm respectively on both sides (right and left).